CANNABIS AS AN EXIT DRUG
As part of its official religion, alcohol has been protected in
Slovenia, and users wishing to transition to a safer drug have been
told the cure is illegal and immoral or something, stigmatised,
criminalised, and used as a cash cow by the judiciary, in the way
alcoholics tend to see the economy.
Typically, Slovenia has not noticed anything non-economic about
cannabis. To Slovenia, a suicide is not a wasted life, but a waste of
educational resources. But it has been observed that alcohol and
cannabis are substitutes when it comes to user expenditure.
https://www.tandfonline.com/doi/full/10.1080/1331677X.2018.1561321
[806]
"L'alcoolisme a conduit 2 membres de ma famille au suicide. Le
cannabis a permis 2 autres d'arrter l'alcool."
https://twitter.com/ConradMaj
[808]
According to Tod H Mikuriya (2004):
"No clinical trials of the efficacy of cannabis as a substitute for
alcohol are reported in the literature, and there are no papers
directly on point prior to my own account (Mikuriya 1970) of a patient
who used cannabis consciously and successfully to discontinue her
problematic drinking. There are ample references, however, to the use
of cannabis as a substitute for opiates (Birch 1889) and as a
treatment for delirium tremens (Clendinning 1843; Moreau 1845), which
were among the first uses by European physicians. The 1873 Indian
Government Finance Department Resolution recommended against
suppressing cannabis use for fear that people (p. 1395) 'would in all
probability have recourse to some other stimulant such as alcohol.'
"The Indian Hemp Drugs Commission Report of (1893-1894) articulated
the same concern (p. 359): '. . . driving the consumers to have
recourse to other stimulants or narcotics which may be more
deleterious.
"Birch (1889) described a patient weaned off alcohol by use of opiates
who then became addicted and was weaned off opiates by use of
cannabis. He noted (p. 625), 'Ability to take food returned. He began
to sleep well; his pulse exhibited some volume; and after three weeks
he was able to take a turn on the verandah with the aid of a stick.
After six weeks he spoke of returning to his post, and I never saw him
again.'"
Reviewing his own 92 patients using cannabis as an alcohol
substitute:
"All patients reported benefit, indicating that for at least a subset
of alcoholics, cannabis use is associated with reduced drinking."
https://hams.cc/mikuriya.pdf
[3822]
In "Reductions in alcohol use following medical cannabis initiation:
results from a large cross-sectional survey of medical cannabis
patients in Canada", Lucas et al (2020) found the same, rather
obvious, thing, publishing their results almost 21 years after the
ZPPPD in the International Journal of Drug Policy:
"Background: Evidence details how cannabis can influence the use of
other psychoactive substances, including prescription medications,
alcohol, tobacco and illicit drugs, but very little research has
examined the factors associated with these changes in substance use
patterns. This paper explores the self-reported use of cannabis as a
substitute for alcohol among a Canadian medical cannabis patient
population.
"Methods: Data was derived from a survey of 2102 people enrolled in
the Canadian medical cannabis program. We included 973 (44%)
respondents who reported using alcohol on at least 10 occasions over a
12 month period prior to initiating medical cannabis, and then used
retrospective data on the frequency and amount of alcohol use pre-and
post medical cannabis initiation to determine which participant
characteristics and other variables were associated with reductions
and/or cessation of alcohol use.
"Results: Overall, 419 (44%) participants reported decreases in
alcohol usage frequency over 30 days, 323 (34%) decreased the number
of standard drinks they had per week, and 76 (8%) reported no alcohol
use at all in the 30 days prior to the survey. Being below 55 years of
age and reporting higher rates of alcohol use in the pre-period were
both associated with greater odds of reducing alcohol use, and an
intention to use medical cannabis to reduce alcohol consumption was
associated with significantly greater odds of both reducing and
ceasing alcohol use altogether.
"Conclusions: Our findings suggest that medical cannabis initiation
may be associated with self-reported reductions and cessation of
alcohol use among medical cannabis patients. Since alcohol is the most
prevalent recreational substance in North America, and its use results
in significant rates of criminality, morbidity and mortality, these
findings may result in improved health outcomes for medical cannabis
patients, as well as overall improvements in public health and
safety."
https://www.sciencedirect.com/science/article/abs/pii/S0955395920303017?via%3Dihub
[399]
Pince et al (2025) found similar support for substitution:
"We investigated the effects of legal-market cannabis on alcohol
self-administration and craving using a within-subjects human
laboratory drug administration paradigm. We tested whether cannabis
serves as a substitute for alcohol (i.e., attenuating alcohol
consumption and craving) in a sample of community adults who drink
heavily and use cannabis regularly. Consistent with our hypothesis, we
found that across the entire sample, self-administering cannabis
before alcohol significantly reduced alcohol consumption compared to
when alcohol was offered without cannabis. Furthermore, we found that
cannabis and alcohol co-administration was associated with significant
acute reduction in alcohol craving compared to alcohol administration
alone."
In "the first study to test effects of legal-market cannabis on
alcohol intake...Cannabis use was associated with a reduction in
alcohol intake...Those who drank less after cannabis reported greater
decreases in alcohol craving" reported Pince et al (2025):
"While human laboratory studies are comparatively limited, Mello and
colleagues instructed participants to complete a basic operant task
wherein they could earn cannabis or money after 30 min of work
and alcohol after 15 min, and found that individuals
self-administered less alcohol when cannabis was concurrently
available (Mello et al., 1978). Later, Ballard and DeWitt found that
co-administration of low doses of THC and alcohol reduced alcohol
craving (Ballard and de Wit, 2011). An unpublished laboratory study
also observed that cannabis use was associated with acute reductions
in alcohol intake and some measures of craving in a within-subjects
design with individuals who engage in heavy drinking (Metrik et al.,
unpublished). Other observational studies have reported similar
reductions in alcohol consumption when cannabis was used before
alcohol (Gunn et al., 2021; Karoly et al., 2023, Karoly et al., 2024;
Rootman, 2020). The effects of cannabis on alcohol craving and
consumption during simultaneous use may be mediated in part by
subjective effects (i.e., relaxation versus stimulation), as
simultaneous use predicted discontinuation of drinking via increased
relaxation and decreased alcohol craving at the event-level in an
ecological momentary assessment study (Waddell et al., 2024).
Together, these findings suggest the potential for cannabis to act as
a substitute for alcohol. Further research is needed to elucidate
variables that may predict such substitution behavior."
https://www.sciencedirect.com/science/article/abs/pii/S0376871625003138
[4933]
Gunn et al (2025) think "Working memory capacity predicts
cannabis-induced effects on alcohol urge":
"Participants aged 21 to 44 (N = 125, 32 % female) reporting heavy
alcohol use and cannabis use ≥ twice weekly completed a laboratory
protocol across three days where they smoked a placebo, 3.1 % delta-9
tetrahydrocannabinol (THC), and 7.2 % THC cannabis cigarette.
Participants were asked to rate their alcohol urge pre and post
smoking. Prior to the experimental sessions, participants completed
WMC measures including the n-back and the complex span tasks,
operation span (OS) and symmetry span (SS).
"Results
Those with higher WMC, as assessed via the SS task, reported
significantly lower alcohol urge after smoking the 7.2 %, but not the
3.1 %, THC dose, relative to placebo. Performance on the OS task was
not associated with alcohol urge. Lower WMC as determined via n-back
scores was associated with higher alcohol urge overall, but n-back
scores did not moderate the impact of cannabis on alcohol urge.
"Conclusion
Findings suggest individuals with higher but not lower working memory
experience lower alcohol urge under acute effects of cannabis.
Although cannabis is increasingly perceived as a substitute for
alcohol, individuals with lower working memory may be less likely to
experience such benefits when attempting to reduce their drinking."
https://www.sciencedirect.com/science/article/pii/S030646032500334X?via%3Dihub
[5664]
In "Acute cannabidiol administration reduces alcohol craving and
cue-induced nucleus accumbens activation in individuals with alcohol
use disorder: the double-blind randomized controlled ICONIC trial" and
using CBD only, Zimmermann et al (2024) were able to confirm the
effect of cannabis on craving found in alcoholism and addiction in
general [see
2978].
"Here we report data from the double-blind randomized controlled
ICONIC trial that compared the effects of a single dose of
800 mg cannabidiol against placebo (PLC) in
N = 28 individuals with AUD. Cue-induced nucleus
accumbens (NAc) activation, alcohol craving during a combined stress-
and alcohol cue exposure session, as well as craving during an fMRI
alcohol cue-reactivity task and CBD plasma levels served as outcomes.
Individuals receiving CBD showed lower bilateral cue-induced NAc
activation (tleft_NAc(23) = 4.906,
p < 0.001, d = 1.15; tright_NAc
(23) = 4.873, p < 0.001,
d = 1.13) and reported significantly lower alcohol
craving after a combined stress- and alcohol cue exposure session
(Fgroup(1,26) = 4.516, p = 0.043,
eta2 = 0.15) and during the fMRI cue-reactivity task
(Fgroup(1,24) = 6.665, p = 0.015,
eta2 = 0.23). CBD levels were significantly higher in
the CBD group (t(25) = 3.808,
p < 0.001, d = 1.47) and showed a
significant negative association with alcohol craving during the cue
exposure experiment (r = −0.394,
pFDR = 0.030) and during fMRI
(r = −0.389, pFDR = 0.030), and with
left and right NAc activation (rleft_NAc = −0.459,
pFDR = 0.030; rright_NAc = −0.405,
pFDR = 0.030). CBDs capacity to reduce stress- and
cue-induced alcohol craving and to normalize NAc activation a region
critical to the pathophysiology of AUD contribute to understanding the
neurobiological basis of its clinical effects and support its
potential as a treatment option for AUD."
https://www.nature.com/articles/s41380-024-02869-y
[3787]
Pince et al (2026) are researching "Behavioral phenotypes associated
with cannabis and alcohol substitution":
"This study is an exploratory analysis of data from a within-subjects,
crossover laboratory study on alcohol and cannabis co-administration.
Participants completed two sessions: one in which they
self-administered alcohol after using cannabis, and one in which they
self-administered alcohol but did not use cannabis. We aim to compare
behavioral phenotypes of individuals who self-administered less
alcohol after cannabis ('substituters'; n = 23), more
alcohol after cannabis ('complementers'; n = 7), or the
same amount of alcohol regardless of whether cannabis was used
('non-substituters'; n = 16). We utilized Welch's ANOVAs
and Kruskal-Wallis tests to compare baseline group differences,
drawing on domains from the Addictions Neuroclinical Assessment (ANA)
framework. Wilcoxon tests were employed to test differences in
laboratory self-administration measures between sessions for each
group.
"Results
Substituters had significantly lower scores on measures corresponding
to ANA domains of negative emotionality (BDI-II, DASS-Depression) and
executive function (UPPS-P Lack of Premeditation) than
non-substituters. Substituters endorsed higher positive cannabis
expectancies than non-substituters, though expectancy differences did
not reach significance.
"Conclusions
Individuals who use cannabis and alcohol and have lower levels of
negative emotionality and impulsivity may be more likely to substitute
cannabis for alcohol. Future research is needed to explore long-term
outcomes of cannabis substitution."
https://link.springer.com/article/10.1186/s12954-026-01432-y
[6002]
CBD was an exit drug for fruit flies in "Long term exposure to dietary
cannabinoids inhibits rapid functional tolerance to ethanol in
Drosophila melanogaster adults" by Vidal et al (2025):
"Given that CBD acts as a natural antagonist of CB1R, and CB1R
antagonists have been shown to reduce the self-administration and
appetitive value of ethanol in rodent models (Arnone et al., 1997;
Economidou et al., 2006), as well as inhibit the development of rapid
tolerance to ethanol in rats (Lemos et al., 2007), CBD had long been
viewed as a promising pharmacotherapy candidate to treat alcohol used
disorders (AUD). Accordingly, CBD treatment was shown to inhibit the
context-dependent relapse into alcohol seeking in rats with a history
of alcohol consumption (Gonzalez-Cuevas et al., 2018), and their
ability to develop tolerance to sedation by alcohol following
re-exposure (Szulc et al., 2023). Not surprisingly, most previous work
has focused on the potential role of CB1/2R-dependent signaling in the
cross-talk between ethanol and CBD. Notably, Viudez-Martinez and
colleagues showed that a 5HT1A serotonin receptor antagonist could
block the reduction in alcohol self-administration triggered by the
combined treatment with CBD and naltrexone (Viudez-Martnez et al.,
2018), establishing a precedent for the potential involvement of
non-canonical cannabinoid signaling in the cross-talk between CBD and
alcohol."
https://www.micropublication.org/journals/biology/micropub-biology-001825
[5816]
In a prelude to their larger 2021 study "Cannabis Significantly
Reduces the Use of Prescription Opioids and Improves Quality of Life"
[2815] in 2017 Lucas and Walsh published a study in which they surveyed
271 medical cannabis patients in research funded by Tilray.
"Findings include high self-reported use of cannabis as a substitute
for prescription drugs (63%), particularly pharmaceutical opioids
(30%), benzodiazepines (16%), and antidepressants (12%). Patients also
reported substituting cannabis for alcohol (25%), cigarettes/tobacco
(12%), and illicit drugs (3%). A significant percentage of patients
(42%) reported accessing cannabis from illegal/unregulated sources in
addition to access via LPs, and over half (55%) were charged to
receive a medical recommendation to use cannabis, with nearly 25%
paying $300 or more."
https://www.sciencedirect.com/science/article/abs/pii/S0955395917300130
[3083]
Holman et al
"...conducted an anonymous, cross-sectional online survey in May 2021
for seven days with adult Canadian federally-authorized medical
cannabis patients (N = 2697) registered with two global cannabis
companies to evaluate patient perceptions of Primary Care Provider
(PCP) knowledge of medical cannabis and communication regarding
medical cannabis with PCPs, including PCP authorization of licensure
and substitution of cannabis for other medications. Overall, 47.1% of
participants reported substituting cannabis for pharmaceuticals or
other substances (e.g., alcohol, tobacco/nicotine).
https://jcannabisresearch.biomedcentral.com/counter/pdf/10.1186/s42238-022-00141-0.pdf
[1826]
Similar results for alcohol came from Kruger et al (2026) at Buffalo
University, NY, for whom cannabis is a "novel harm reduction
strategy":
"Alcohol consumption is associated with nearly 200 health conditions.
As cannabis-infused beverages emerge in the legal market, their
potential as a substitute for alcohol is of growing interest. This
study investigates whether cannabis beverages may reduce alcohol use.A
total of 438 anonymous adults who used cannabis in the past year
completed a survey including cannabis use and alcohol consumption
items from the Behavioral Risk Factor Surveillance System (BRFSS).
Chi-square and t-tests compared alcohol use between cannabis beverage
users and non-users, and before vs. after cannabis beverage
initiation.About one-third (33.6%) of respondents used cannabis
beverages, typically consuming one per session. Users were more likely
to report substituting cannabis for alcohol (58.6%) than non-users
(47.2%). They also reported fewer weekly alcoholic drinks after
starting cannabis beverages (M = 3.35) compared to before (M = 7.02),
and binge drank less frequently (80.7% reported less than monthly or
never, vs. 47.2% before). Those who cited reducing other substance use
were more likely to use cannabis beverages (45.8%).Findings suggest
cannabis beverages may support alcohol substitution and reduce
alcohol-related harms, offering a promising alternative for
individuals seeking to lower alcohol intake."
https://pubmed.ncbi.nlm.nih.gov/41533430/
[5873]
Anderson et al at the National Bureau of Economic Research:
"...find that both state MMLs and RMLs are associated with decreases
in teen marijuana consumption, consistent with the hypothesis that
selling to minors becomes a relatively risky proposition for licensed
marijuana dispensaries. In addition, we find that MMLs are associated
with decreases in teen cigarette use."
https://www.nber.org/system/files/working_papers/w26780/w26780.pdf
[400]
Raman and Bradford (2022) find "Recreational cannabis legalizations
associated with reductions in prescription drug utilization among
Medicaid enrollees":
"We use quarterly data for all Medicaid prescriptions from 2011 to
2019 to investigate the effect of state-level RCLs [recreational
cannabis laws] on prescription drug utilization. We estimate this
effect with a series of two-way fixed effects event study models. We
find significant reductions in the volume of prescriptions within the
drug classes that align with the medical indications for pain,
depression, anxiety, sleep, psychosis, and seizures. Our results
suggest substitution away from prescription drugs and potential cost
savings for state Medicaid programs.
https://onlinelibrary.wiley.com/doi/10.1002/hec.4519
[1827]
In Canada, Jeddi et al examined "Cost-Effectiveness of Medical
Cannabis Versus Opioids for Chronic Noncancer Pain" (in Canadian
dollars):
"Total mean annual cost per patient was $1,980 for oral medical
cannabis and $1,851 for opioids, a difference of $129 (95% confidence
interval [CI]: -$723 to $525). Mean QALYs were 0.582 for both oral
medical cannabis and opioids (95% CI: -0.007 to 0.015).
Cost-effectiveness acceptability curves showed that oral medical
cannabis was cost-effective in 31% of iterations at willingness-to-pay
thresholds up to $50,000/QALY gained. Use of opioids is associated
with nonfatal and fatal overdose, whereas medical cannabis is not.
Discussion: Our findings suggest that medical cannabis as an
alternative to opioids for chronic pain may confer similar, but
modest, benefits to patients, and reduce the risk of opioid overdose
without substantially increasing costs."
https://www.liebertpub.com/doi/10.1089/can.2024.0120?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub++0pubmed
[5182]
On this side of the Atlantic, a report by Sapphire Clinics on opioid
prescription in the UK found that one in seven (14%) chronic pain
patients prescribed opioid medications claim they became dependent or
addicted, while strong side effects reportedly stopped one in four
(23%) from living a normal life.
57 million prescriptions for opioids such as tramadol, codeine and
fentanyl, were issued to UK patients in 2022, an average of one 108
every minute.
https://www.sapphireclinics.com/wp-content/uploads/2023/06/opioid-campaign-whitepaper.pdf
[2852]
Marrinan et al (2024) in the UK determined that increasing access to
medical cannabis on the NHS for chronic pain could save the state
healthcare provider almost 4 billion annually, 729 per
patient.
"An early cost-effectiveness model was developed to estimate the
impact of prescribing CBMPs alone and/or in addition to analgesics,
physiotherapy, and cognitive behavioral therapy for chronic pain in
the UK for 1 year.
"Results
Due to their comparative effectiveness, CBMPs were found to be cost
saving."
https://www.tandfonline.com/doi/full/10.1080/14737167.2024.2412248
[3629]
In "Perceived Efficacy, Reduced Prescription Drug Use, and Minimal
Side Effects of Cannabis in Patients with Chronic Orthopedic Pain"
(2022) Greis et al explain:
"Extant inventories for measuring cannabis use were not designed to
capture the medically relevant features of cannabis use, but rather
were designed to detect problematic use or cannabis use disorder.
Thus, we sought to capture the medically relevant features of cannabis
use in a population of patients with orthopedic pain and pair these
data with objective measures of pain and prescription drug
use."
The results show:
"Medical cannabis use was associated with clinical improvements in
pain, function, and quality of life with reductions in prescription
drug use; 73% either ceased or decreased opioid consumption and 31%
discontinued benzodiazepines. This work provides a direct relationship
between the initiation of cannabis therapy and objectively fewer
opioid and benzodiazepine prescriptions.
https://www.liebertpub.com/doi/10.1089/can.2021.0088
[1828]
In Israel, Aviram et al (2021) found
Patients with chronic pain, licensed to use MC in Israel, reported
weekly average pain intensity (primary outcome) and related symptoms
before and at 1, 3, 6, 9 and 12 months following MC [medical cannabis]
treatment initiation.. 43% of the patients who had been using
analgesic medications prior to MC treatment initiation were no longer
using them. This was true for all classes of analgesic drugs including
over the counter analgesics, non-steroidal anti-inflammatory drugs,
anticonvulsants and antidepressants. As for opioid use, 24% and 20% of
the participants who had been using weak or strong opioids,
respectively, at baseline stopped using them by the time they reached
the 12-month follow-up.
https://pubmed.ncbi.nlm.nih.gov/33065768/
[1829]
In "Utilization of medicinal cannabis for pain by individuals with
spinal cord injury" Stillman et al found non-users live in a different
reality:
"Never users were less likely than current and past users to agree
that cannabis should be legalized (CU + PU = 98.00%; NU = 88.10%;
χ2 = 10.92, p = .001) (Table 2) and more likely to believe that
cannabis is a 'gateway drug' (CU + PU = 7.40%; NU = 22.50%; χ2 =
12.80, p = 0.00), a 'very dangerous' drug (CU + PU = 1.30%; NU =
7.00%; χ2 = 5.90, p = 0.026), and that it is safer to take
prescription pain killers than to use MC (CU + PU = 4.00%; NU =
11.80%; χ2 = 5.91, p = 0.021). There was widespread agreement
among participants that cannabis could have medicinal effects (CU + PU
= 96.00%; NU = 95.30%; χ2 = 0.07, p = 1.00) and that its use
carries either no or only slight health risks (CU + PU = 91.20%; NU =
83.60%; χ2 = 3.61, p = 0.067). There were no significant
differences in perceptions of social or legal risks between the user
groups."
But these authors did not find any difference in pain interference.
On the other hand:
"Subjects were asked to select from a list of 33 possible effects
that could be ascribed to MC and/or prescription medications and that
could be considered either positive, negative, or neutral. On average,
MC was assigned 7.6 positive effects while prescription medications
were assigned 5.35 (t = 3.9, df = 234; p = .000). Medicinal cannabis
was assigned an average of 6.0 negative effects while prescription
medications were assigned 9.9 (t = −3.76, df = 203; p = .001).
"When asked to compare the relative efficacy of MC with that of other
medications in providing symptom relief (98 CU and 30 PU), 63.3%
reported that cannabis works better than prescription medications,
17.20% reported the opposite, and 10.20% answered that only cannabis
offered them relief (χ2 = 7.93, p = 0.047). When asked if they
suffer or had suffered from symptoms or conditions that had not been
helped by MC, 35.20% replied yes (CU = 31.60%; PU = 46.70%; NS) and
64.80% replied no (CU = 68.40%; PU = 53.30%; NS)."
Among our subjects, over 90 percent of CU [cannabis users] and PU
[past users] reported a little or great relief from symptoms with MC
[medical cannabis] and 61.20 percent claimed that MC had allowed them
to reduce or discontinue use of other medications.
https://www.nature.com/articles/s41394-019-0208-6.pdf
[1830]
In "The Impact of Isolated Baseline Cannabis Use on Outcomes
Following Thoracolumbar Spinal Fusion: A Propensity Score-Matched
Analysis" Shah et al write:
"704 patients were identified (n=352 each), with comparable age, sex,
race, primary insurance, Charlson/Deyo scores, surgical approach, and
levels fused between cohorts (all, p>0.05). Cannabis users (versus
non-users) incurred lower 90-day overall and medical complication
rates (2.4% vs. 4.8%, p=0.013; 2.0% vs. 4.1%, p=0.018). Cohorts had
otherwise comparable complication, revision, and readmission rates
(p>0.05). Baseline cannabis use was associated with a lower risk of
90-day medical complications (OR=0.47, p=0.005). Isolated baseline
cannabis use was not associated with 90-day surgical complications and
readmissions, or two-year revisions.
"Isolated baseline cannabis use, in the absence of any other
diagnosed substance abuse disorders, was not associated with increased
odds of 90-day surgical complications or readmissions or two-year
revisions, though its use was associated with reduced odds of 90-day
medical complications when compared to non-users undergoing TLF
(thoracolumbar spinal fusion) for ASD (adult spinal
deformity)."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9210439/
[1942]
In 2020's "The impact of cannabis access laws on opioid prescribing",
(2020) McMichael et al point out that
"...the number of opioid prescriptions quadrupled in the first
fifteen years of the new millennium."
and
"The five specialties that have the highest prescribing rates, as
measured by MMEs, reduce their opioid use by 28.3 percent when an RCL
is passed and 6.9 percent when an MCL is passed."
"Table A1 reports the means of each of our outcome variables across
different cannabis legal regimes for all specialties for which we have
at least 2,000 provider-year observations."
"In general, we find consistent evidence that both RCLs and MCLs
reduce the use of prescription opioids. These laws reduce the amount
of annual MMEs prescribed by individual providers by 6.9 and 6.1
percent, respectively. However, our results are not unique to the MME
measure of opioid prescriptions, and both types of cannabis access
laws similarly reduce the total days supply of opioids, the number of
patients to whom providers prescribe opioids, and the probability that
a provider prescribes any opioids. Interestingly, while we find
evidence that RCLs and MCLs reduce opioid use across a wide array of
medical (and other) specialties, the magnitude of this reduction is
not uniform across specialties."
Summary Statistics by Specialty Panel A compares MMEs [morphine
milligram equivalents] for All Providers and Providers Not Subject to
Any Cannabis Access Law. Only two of the 48 specialties listed -
Clinical Nurse Specialist and Physician Assistant - show modestly
lower MMEs where there is no cannabis access law, and so 46 were
higher.
https://scholarship.law.ua.edu/cgi/viewcontent.cgi?article=1150&context=fac_working_papers
[1831]
"Our sample included 888 individuals receiving treatment for chronic
pain, of whom 99.4% received treatment with prescription opioids or
MC.
"Methods. Problematic use of prescription opioids and MC was assessed
using DSM-IV criteria, Portenoys Criteria (PC), and the Current Opioid
Misuse Measure (COMM) questionnaire. Additional sociodemographic and
clinical correlates of problematic use were also assessed.
"Results. Among individuals treated with prescription opioids,
prevalence of problematic use of opioids according to DSM-IV, PC, and
COMM was 52.6%, 17.1%, and 28.7%, respectively. Among those treated
with MC, prevalence of problematic use of cannabis according to DSM-IV
and PC was 21.2% and 10.6%, respectively. Problematic use of opioids
and cannabis was more common in individuals using medications for
longer periods of time, reporting higher levels of depression and
anxiety, and using alcohol or drugs. Problematic use of opioids was
associated with higher self-reported levels of pain, and problematic
use of cannabis was more common among individuals using larger amounts
of MC.
"Conclusions. Problematic use of opioids is common among chronic pain
patients treated with prescription opioids and is more prevalent than
problematic use of cannabis among those receiving MC. Pain patients
should be screened for risk factors for problematic use before
initiating long-term treatment for pain-control."
https://academic.oup.com/painmedicine/article-pdf/18/2/294/10452408/pnw134.pdf
[1832]
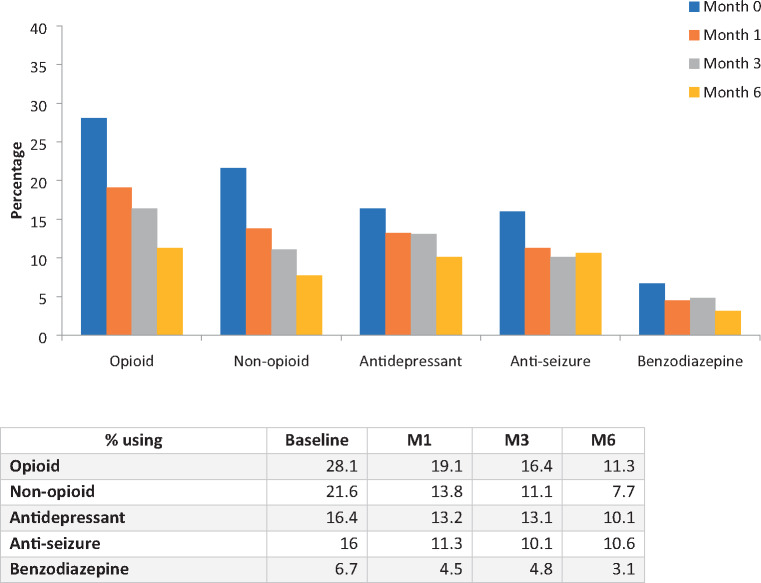
Another medical cannabis study by Lucas et al (2021) focuses
"...on the impacts of cannabis on prescription opioid use and quality
of life over a 6-month period."
using 1145 patients and
"...a comprehensive cannabis use inventory, the World Health
Organization Quality of Life Short Form (WHOQOL-BREF), and a detailed
prescription drug questionnaire."
and
"Participants were 57.6% female, with a median age of 52 years.
Baseline opioid use was reported by 28% of participants, dropping to
11% at 6 months. Daily opioid use went from 152 mg morphine milligram
equivalent (MME) at baseline to 32.2 mg MME at 6 months, a 78%
reduction in mean opioid dosage. Similar reductions were also seen in
the other four primary prescription drug classes identified by
participants, and statistically significant improvements were reported
in all four domains of the WHOQOL-BREF."
and
"The high rate of cannabis use for chronic pain and the subsequent
reductions in opioid use suggest that cannabis may play a harm
reduction role in the opioid overdose crisis, potentially improving
the quality of life of patients and overall public health."
Other pharmaceuticals suffered terribly as well:
"Over 6 months, the percentage of patients using non-opioid pain
medications went from 21.6% (n=241) to 7.7% (n=32), use of
antidepressants declined from 16.4% (n=183) to 10.1% (n=42), use of
antiseizure medications went from 16% (n=178) to 10.6% (n=44), and
benzodiazepine use decreased from 6.7% of participants at baseline
(n=75) to 3.1% at M6."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7971472/
[2815]
Dranitsaris et al (2021) examined opioid prescribing before and after
legalisation in Canada:
"Purpose: On 17 October 2018 recreational cannabis became legal in
Canada, thereby increasing access and reducing the stigma associated
with its use for pain management. This study assessed total opioid
prescribing volumes and expenditures prior to and following cannabis
legalization.
"Methods: National monthly claims data for public and private payers
were obtained from January 2016 to June 2019. The drugs evaluated
consisted of morphine, codeine, fentanyl, hydrocodone, hydromorphone,
meperidine, oxycodone, tramadol, and the non-opioids gabapentin and
pregabalin. All opioid volumes were converted to a mean morphine
equivalent dose (MED)/claim, which is analogous to a prescription from
a physician. Gabapentin and pregabalin claims data were analyzed
separately from the opioids. Time-series regression modelling was
undertaken with dependent variables being mean MED/claim and total
monthly spending. The slopes of the time-series curves were then
compared pre- versus post-cannabis legalization.
"Results: Over the 42-month period, the mean MED/claim declined
within public plans (p < 0.001). However, the decline in MED/claim
was 5.4 times greater in the period following legalization (22.3
mg/claim post vs. 4.1 mg/claim pre). Total monthly opioid spending was
also reduced to a greater extent post legalization ($Can267,000 vs.
$Can95,000 per month). The findings were similar for private drug
plans; however, the absolute drop in opioid use was more pronounced
(76.9 vs. 30.8 mg/claim). Over the 42-month period, gabapentin and
pregabalin usage also declined.
"Conclusions: Our findings support the hypothesis that easier access
to cannabis for pain may reduce opioid use for both public and private
drug plans."
https://pubmed.ncbi.nlm.nih.gov/33491149/
[2143]
According to Beasley and Dundas (2024) in "Recreational cannabis
dispensary access effects on prescription opioid use and mortality",
in Oregon:
"Results suggest that communities located closer to recreational
dispensaries are associated with lower rates of prescription opioids
per capita. We also show that reasonable bounds to our primary
specification suggest communities located within a mile from a
recreational dispensary have prescription opioid rates per capita that
are 1.03.9 percent lower than surrounding communities."
The study acknowledges that while opioid-related mortality rates
appeared unaffected by proximity to retail marijuana, its possible
that other measures of opioid harms, for example hospitalizations, may
nevertheless show an impact.
While mortality rates do not appear to be driven by changes in
cannabis access, it says, hospitalizations related to overdoses may be
impacted. An extension of this work assessing hospitalizations in lieu
of mortalitymay yield further insight.
Authors said in the email to Marijuana Moment that the issue of
hospitalizations was raised during peer review of the article and our
discussion in the paper on hospitalizations is meant to convey that
mortality reduction is just one metric that could be impacted by
reduced opioid prescriptions.
For example, it may be possible that the same number of people
succumb to opioid misuse, while fewer people are hospitalized, they
added.
https://www.sciencedirect.com/science/article/abs/pii/S016604622400067X?via%3Dihub
[3128]
In Utah, most patients who reduced opioid prescriptions were using
cannabis products with a ratio of 1:0 (64%), a ratio of 1:1 (19%) and
0:1 (16%):
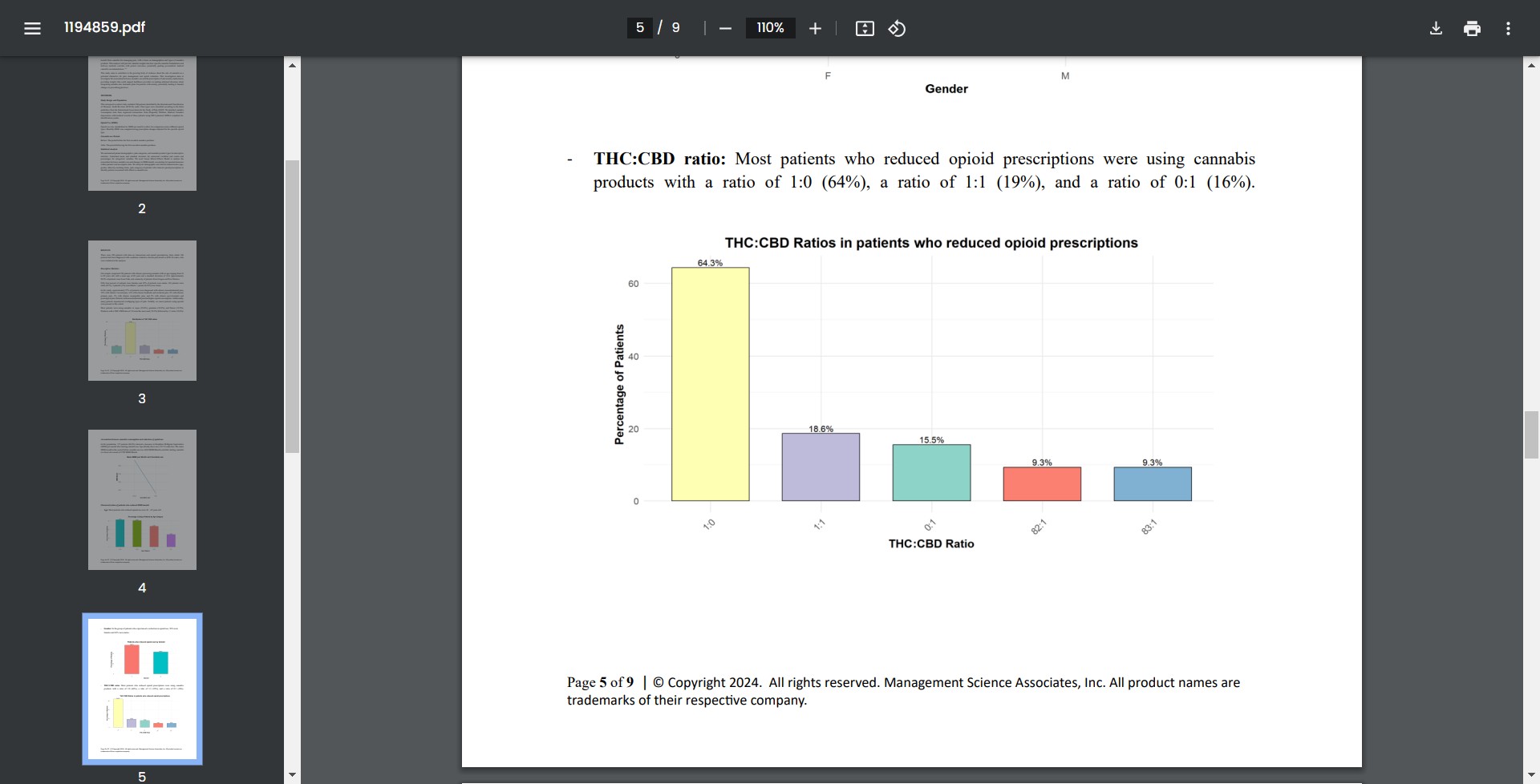
84% showed a decrease in Morphine Milligram Equivalents (MME) per
month after starting cannabis use.
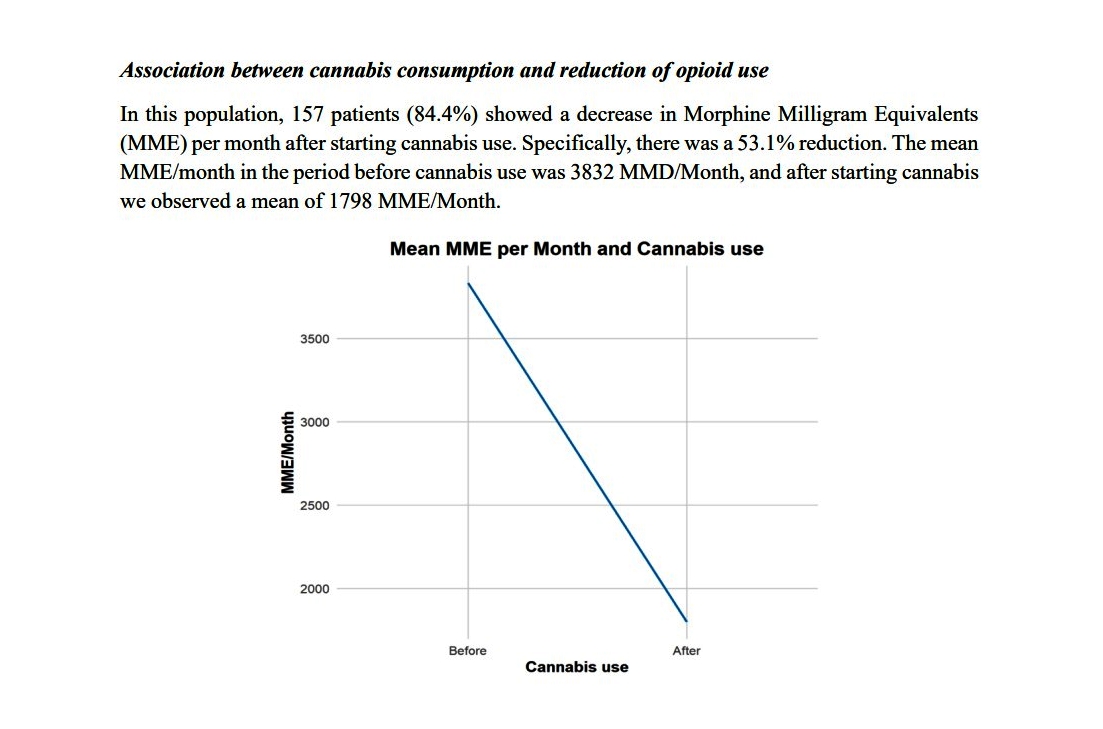
https://www.utah.gov/pmn/files/1194859.pdf
[3742]
In Israel, Feingold et al examined "Depression and anxiety among
chronic pain patients receiving prescription opioids and medical
marijuana"...or both:
"Prevalence of depression among patients in the OP (opioids), MM
(medical marijuana) and OPMM groups was 57.1%, 22.3% and 51.4%,
respectively and rates of anxiety were 48.4%, 21.5% and 38.7%,
respectively. Levels of depression and anxiety are higher among
chronic pain patients receiving prescription opioids compared to those
receiving MM. Findings should be taken into consideration when
deciding on the most appropriate treatment modality for chronic pain,
particularly among those at risk for depression and anxiety."
https://www.ncbi.nlm.nih.gov/pubmed/28453948
[1833]
Hsu and Kovcs (2021) reported an "Association between county level
cannabis dispensary counts and opioid related mortality rates in the
United States: panel data study" of 812 counties in the United States
in the 23 states that allowed legal forms of cannabis dispensaries to
operate by the end of 2017.
"Participants The study used US mortality data from the Centers for
Disease Control and Prevention combined with US census data and data
from Weedmaps.com on storefront dispensary operations. Data were
analyzed at the county level by using panel regression methods.
"Main outcome measure The main outcome measures were the log
transformed, age adjusted mortality rates associated with all opioid
types combined, and with subcategories of prescription opioids,
heroin, and synthetic opioids other than methadone. The associations
of medical dispensary and recreational dispensary counts with age
adjusted mortality rates were also analyzed.
"Results County level dispensary count (natural logarithm) is
negatively related to the log transformed, age adjusted mortality rate
associated with all opioid types (β=−0.17, 95% confidence
interval −0.23 to −0.11). According to this estimate, an
increase from one to two storefront dispensaries in a county is
associated with an estimated 17% reduction in all opioid related
mortality rates. Dispensary count has a particularly strong negative
association with deaths caused by synthetic opioids other than
methadone (β=−0.21, 95% confidence interval −0.27 to
−0.14), with an estimated 21% reduction in mortality rates
associated with an increase from one to two dispensaries. Similar
associations were found for medical versus recreational storefront
dispensary counts on synthetic (non-methadone) opioid related
mortality rates.
"Conclusions Higher medical and recreational storefront dispensary
counts are associated with reduced opioid related death rates,
particularly deaths associated with synthetic opioids such as
fentanyl. While the associations documented cannot be assumed to be
causal, they suggest a potential association between increased
prevalence of medical and recreational cannabis dispensaries and
reduced opioid related mortality rates. This study highlights the
importance of considering the complex supply side of related drug
markets and how this shapes opioid use and misuse.
https://www.bmj.com/content/372/bmj.m4957
[4778]
Looking at cannabis use for pain management and harm reduction,
Kitchen et al (2025) report:
"Between June 2014 and May 2022, 2340 PWUD were initially recruited
and of those 1242 PWUD reported chronic pain, use of unregulated
opioids and completed at least two follow-up visits. Of these 1242
participants, 764 experienced a cessation event over 1038.2
person-years resulting in a cessation rate of 28.5 per 100
person-years (95% confidence interval [CI] 25.4-31.9). Daily cannabis
use was positively associated with opioid cessation (adjusted hazard
ratio 1.40, 95% CI 1.08-1.81; p = 0.011). In the sex-stratified
sub-analyses, daily cannabis use was significantly associated with
increased rates of opioid cessation among males (adjusted hazard ratio
1.50, 95% CI 1.09-2.08; p = 0.014)."
https://pubmed.ncbi.nlm.nih.gov/40011075/
[5174]
Steuart et al (2025) took a long-term look at "Recreational Cannabis
Laws and Fills of Pain Prescriptions in the Privately Insured":
"Using data from a national sample of commercially insured adults, we
examine the effect of recreational cannabis legalization (through two
sequential policies) on prescribing of opioids, NSAIDS, and other pain
medications by implementing synthetic control estimations and
constructing case-study level counterfactuals for the years
2007-2020.
"Results:
Overall, we find recreational cannabis legalization is associated with
a decrease in opioid fills among commercially insured adults in the
U.S., and we find evidence of a compositional change in prescriptions
of pain medications more broadly. Specifically, we find marginally
significant increases in prescribing of non-opioid pain medications
after recreational cannabis becomes legal in some states. Once
recreational cannabis dispensaries open, we find statistically
significant decreases in the rate of opioid prescriptions (13%
reduction from baseline, p < .05) and marginally significant
decreases in the average daily supply of opioids (6.3% decrease, p
< .10) and number of opioid prescriptions per patient (3.5%
decrease, p < .10).
"Conclusions:
These results suggest that substitution of cannabis for traditional
pain medications increases as the availability of recreational
cannabis increases. There appears to be a small shift once
recreational cannabis becomes legal, but we see stronger results once
users can purchase cannabis at recreational dispensaries. The decrease
in opioids and marginal increase in non-opioid pain medication may
reflect patients substituting opioids with cannabis and non-opioid
pain medications, either separately or concomitantly. Reductions in
opioid prescription fills stemming from recreational cannabis
legalization may prevent exposure to opioids in patients with pain and
lead to decreases in the number of new opioid users, rates of opioid
use disorder, and related harms."
https://pmc.ncbi.nlm.nih.gov/articles/PMC11831899/
[4911]
Drake et al of the University of Pittsburghs School of Public Health
found "a significant reduction in pharmacy-based codeine distribution
in states that have legalized recreational cannabis use. The finding
is promising from a public health policy perspective because misuse of
prescription opioids annually contributes to more than 10,000 overdose
deaths."
and
"The study is believed to be among the first to separately examine
the impact of recreational cannabis laws on shipments of opioids to
hospitals, pharmacies and other endpoint distributors. Previous
studies have focused on medical cannabis laws or use of opioids by
subsets of consumers, such as Medicaid beneficiaries."
and
"Key findings from states that passed recreational cannabis
laws:
"A 26% reduction in pharmacy-based distribution of codeine and as
much as a 37% reduction after recreational cannabis laws have been in
effect for four years.
"Minimal impact on distribution of other opioids such as oxycodone,
hydrocodone and morphine in any setting.
"Minimal impact on codeine distribution by hospitals, which often
have less permissive policies than pharmacies."
"'This finding is particularly meaningful,' said senior author
Coleman Drake of the University of Pittsburghs School of Public
Health. 'Where previous studies have focused on more potent opioids,
codeine is a weaker drug with a higher potential for addiction. It
indicates people may be obtaining codeine from pharmacies for misuse,
and that recreational cannabis laws reduce this illicit
demand.'"
https://news.cornell.edu/stories/2023/01/when-recreational-cannabis-legal-codeine-demand-drops
[2037]
B. Karmakar is an Assistant Professor in the Department of
Statistics, University of Florida, G. Mukherjee is an Associate
Professor in the Department of Data Sciences & Operations,
University of Southern California and W. Kar is an Assistant Professor
of Purdue University. Karmakar, Mukherjee and Kar (2023) studied the
"Effect of Marijuana Legalization on Direct Payments to Physicians by
Opioid Manufacturers" and say:
"Our analysis finds a significant decrease in direct payments from
opioid manufacturers to pain medicine physicians as an effect of MML
passage. We provide evidence that this decrease is due to the
availability of medical marijuana as a substitute. Additionally,
physicians in states with an MML are prescribing fewer opioids.
Finally, the substitution effect is comparatively higher for female
physicians and in localities with higher white, less affluent, and
more working-age populations."
As they explain:
"In the wake of this evolving pain management paradigm, physicians
must remain updated on drugs for appropriate patient care. Without the
latest information regarding the drugs, physicians may be unable to
prescribe opioids appropriately for pain management (Guo et al.,
2021). There is significant concern that a subsequent decrease in
opioid prescription could lead to opioid being a niche product or, in
the extreme, could potentially lead to severely diminished usage of
opioids (Feinberg, 2019, Szalavitz, 2023). Further, as a cascading
effect, it can negatively affect research and development on opioids
as well as decrease in the number of opioid manufacturers. Therefore,
opioid manufacturers use different forms of interactions to engage
with physicians on a regular basis. One of the most common conduits to
facilitate such interactions is through direct payments to physicians
from opioid manufacturers (Jones and Ornstein, 2016, Schwartz and
Woloshin, 2019). These direct payments may be in the form of
consulting and speaker fees, conference travel reimbursements, or meal
vouchers."
and
"...due to the 'Sunshine Act,' pharmaceutical manufacturers are now
mandated by law to report such payments (Richardson et al., 2014). The
act was a federal response to concerns of potential conflict of
interest in physicians accepting these payments, the subsequent
possibility of bias in treatment, and rising health-care costs (Carey
et al., 2021, DeJong et al., 2016, Engelberg et al., 2014, Jones and
Ornstein, 2016). In September 2014, the first batch of data was made
public. This dataset contains the dollar value of the gift/payment
that transpired between a named physician and a named pharmaceutical
manufacturer, associated products for their interaction, and payment
date."
Using a customised synthetic control method:
"Our primary analysis considers all pain medicine physicians from 13
states, of which three (PA, OH, LA) were treated states that passed an
MML in the second quarter of 2016. The method, described in Section
3.4, produces synthetic controls for each physician in the treated
states using physicians in the control states, and likewise produces
synthetic counterparts for each physician in the control states using
physicians in the treated states."
So
"The results reported in Table 4 show a significant negative
correlation between an increase in marijuana patients in preceding
period as well as presence of a marijuana dispensary with
opioid-prescribing physician payment; however, there is no significant
association between physician payment and change in marijuana patients
in the following period. These results provide us with further support
that the substitution effect of marijuana is indeed the dominating
factor in reducing payments to pain medicine physicians post-passage
of MML."
Some tears are necessary for the "opioids ecosystem":
"Our study finds a significant decrease in financial interactions
between opioid manufacturers and physicians as an effect of MML
passage. The finding that the opioid manufacturers in states that
passed MML are stepping away from this particular form of interaction
is concerning, for such activity can significantly affect the opioids
ecosystem."
But back with the patients themselves:
"Analyzing the annual prescription data (mentioned in Section 2), we
found that, in 2015, they prescribed 49% more opioids than non-opioids
in 30 days fill and a similar 49% more days of prescription for opioid
vs non-opioid. From 2015 to 2017, in the states not passing an MML, 30
days fill of opioid vs non-opioid remained flat at a 1.38:1 ratio.
However, in the states passing an MML, from 2015 to 2017, 30 days fill
of opioid vs non-opioid decreased from a 1.57:1 ratio to a 1.52:1
ratio. The ratios for the number of days of prescription in the MML
states also decreased from a 1.57:1 ratio in 2015 to a 1.52:1 ratio in
2017. In particular, the pattern of opioid vs non-opioid prescriptions
did not change in the control states, while there was a relative
decrease in opioid prescriptions in the MML states from 2015 to
2017."
https://people.clas.ufl.edu/bkarmakar/files/2023/03/physicians_opioids.pdf [2328]
In "'I got a bunch of weed to help me through the withdrawals':
Naturalistic cannabis use reported in online opioid and opioid
recovery community discussion forums" Meachem et al (2022)
"...extracted all posts mentioning cannabis-related keywords (e.g.,
'weed', 'cannabis', marijuana) from December 2015 through August 2019
from an opioid use subreddit and an opioid recovery subreddit. The
most frequent phrases from the recovery subreddit referred to time
without using opioids and the possibility of using cannabis as a
treatment. The most common motivations for using cannabis were to
manage opioid withdrawal symptoms in the recovery subreddit, often in
conjunction with anti-anxiety and GI-distress 'comfort meds.' Despite
limitations in generalizability from pseudonymous online posts, this
examination of reports of naturalistic cannabis use in relation to
opioid use identified withdrawal symptom management as a common
motivation.
https://journals.plos.org/plosone/article/file?id=10.1371/journal.pone.0263583&type=printable
[1834]
In 2021's "The association between cannabis use and outcome in
pharmacological treatment for opioid use disorder" Rosic et al in the
Harm Reduction Journal
"Participants receiving pharmacological treatment for OUD
(n = 2315) were recruited from community-based addiction
treatment clinics in Ontario, Canada, and provided information on
past-month cannabis use (self-report). Participants were followed for
3 months with routine urine drug screens in order to assess opioid use
during treatment. We used logistic regression analysis to explore (1)
the association between any cannabis use and opioid use during
treatment, and (2) amongst cannabis-users, specific cannabis use
characteristics associated with opioid use. We found that amongst
cannabis users, those who use cannabis daily are less likely to have
opioid use than people who use cannabis occasionally. This association
was present for both men and women. Future studies should further
examine specific characteristics and patterns of cannabis use that may
be protective or problematic in MAT [medication-assisted
treatment]."
Sex differences were observed:
"Interaction analysis revealed no significant moderating effect of
sex on our cannabis use characteristics of interest (age of onset of
cannabis use by sex: OR = 0.99, 95% CI 0.94, 1.05,
p = 0.725; daily cannabis use by sex:
OR = 0.92, 95% CI 0.53, 1.57, p 0.748; side effects from
cannabis by sex: OR = 1.53, 95% CI 0.93, 2.50,
p = 0.092; marijuana cravings score by sex:
OR = 1.01, 95% CI 0.99, 1.03, p = 0.100).
Using subgroup analysis by sex, we found the association between
reporting cannabis-related side effects and lower odds of opioid use
to hold for men (OR = 0.55, 95% CI 0.40, 0.75,
p < 0.001), but not for women
(OR = 0.86, 95% CI 0.59, 1.26, p = 0.442).
Additionally, for women, but not men, higher marijuana cravings score
was associated with increased odds of opioid use (scaled for each
10-point increase in score: OR = 1.14, 95% CI 1.01,
1.28, p = 0.034)."
Overall
"For cannabis users, daily cannabis use was associated with lower
odds of opioid use, when compared with occasional use
(OR = 0.61, 95% CI 0.470.79, p < 0.001)
as was older age of onset of cannabis use (OR = 0.97,
95% CI 0.94, 0.99, p = 0.032), and reporting
cannabis-related side effects (OR = 0.67, 95% CI 0.51,
0.85, p = 0.001)."
And adopting a rather melancholy angle, they go on:
"Altogether, 75% of cannabis users perceived no impact of cannabis on
their OUD treatment."
https://harmreductionjournal.biomedcentral.com/articles/10.1186/s12954-021-00468-6
[1835]
For Johns Hopkins University School of Medicine, Bergeria et al
(2020)
"Two hundred individuals recruited through Amazon Mechanical Turk
with past month opioid and cannabis use and experience of opioid
withdrawal completed the survey. Participants indicated which opioid
withdrawal symptoms improved or worsened with cannabis use and
indicated the severity of their opioid withdrawal on days with and
without cannabis. 62.5% of 200 participants had used cannabis to treat
withdrawal. Participants most frequently indicated that cannabis
improved: anxiety, tremors, and trouble sleeping. These results show
that cannabis may improve opioid withdrawal symptoms and that the size
of the effect is clinically meaningful."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7212528/
[1836]
Wiese and Wilson-Poe reviewed the evidence in 2018.
"The endocannabinoid and opioidergic systems are known to interact in
many different ways, from the distribution of their receptors to
cross-sensitization of their behavioral pharmacology. Cannabinoid-1
(CB1) receptors and mu opioid receptors (MORs) are distributed in many
of the same areas in the brain, including but not limited to the
periaqueductal gray, locus coeruleus, ventral tegmental area (VTA),
nucleus accumbens, prefrontal cortex (PFC), central amygdala (CeA),
bed nucleus of stria terminalis (BNST), caudate putamen (CP),
substantia nigra, dorsal hippocampus, raphe nuclei, and medial basal
hypothalamus. The extent of this overlapping expression and frequent
colocalization of the CB1 and MOR provide clear morphological
underpinnings for interactions between the opioid and cannabinoid
systems in reward and withdrawal."
Besides,
"Interestingly, microinjections of CB1 agonists into the medial PFC
creates an aversion to doses of morphine that are normally rewarding
(CPP), while CB1 antagonism in this brain region creates a rewarding
effect of subthreshold morphine doses."
"The evidence summarized in this article demonstrates the potential
cannabis has to ease opioid withdrawal symptoms, reduce opioid
consumption, ameliorate opioid cravings, prevent opioid relapse,
improve OUD treatment retention, and reduce overdose deaths. The
compelling nature of these data and the relative safety profile of
cannabis warrant further exploration of cannabis as an adjunct or
alternative treatment for OUD."
https://www.liebertpub.com/doi/10.1089/can.2018.0022
[1837]
In a 2025 paper "Cannabidiol attenuates heroin seeking in male rats
associated with normalization of discrete neurobiological signatures
within the nucleus accumbens with subregional specificity" from
Chisholm et al of the Icahn School of Medicine at Mount Sinai,
Departments of Neuroscience, Psychiatry; Addiction Institute of Mount
Sinai:
"Heroin-trained animals exhibited high levels of cue-induced
heroin-seeking behavior. Importantly, CBD attenuated cue-induced
heroin-seeking behaviors. Postmortem RNA-sequencing of the NAcC and
NAcS revealed shared transcriptomic alterations the NAc subregions in
response to heroin, with a more robust impact of heroin in the NAcS.
Though CBD had minimal impact on the heroin-induced perturbations in
the NAcC, it normalized components of the transcriptomic signature
altered by heroin in both NAc subregions including transcripts that
correlated with heroin-seeking behavior. In contrast, CBD normalized a
particular subset of NAcS genes that correlated to heroin-seeking
behavior. Those genes were specifically linked to the extracellular
matrix, astrocyte function, and their upstream regulators related to
immune function."
https://www.sciencedirect.com/science/article/abs/pii/S0006322325014623
[5449]
Raman et al examined codeine sales at pharmacies in US states which
had passed recreational cannabis laws as of November 2022.
"We implement two-way fixed-effects regressions and leverage
variation from eleven U.S. states that adopted a recreational cannabis
law (RCL) between 2010 and 2019. We find that RCLs lead to a reduction
in codeine dispensed at retail pharmacies. Among prescription opioids,
codeine is particularly likely to be used non-medically. Thus, the
finding that RCLs appear to reduce codeine dispensing is potentially
promising from a public health perspective."
"We are the first study, to our knowledge, to leverage ARCOS data
which details distribution by endpointpharmacies, hospitals,
specialists, and narcotic treatment programsto study the effects of"
recreational legalization, the authors wrote.
They further said that the effect of legalization on codeine
prescribing became more pronounced over years, "increasing from -17.5
percent one year after RCL implementation to -37.3 percent four years
after implementation."
https://onlinelibrary.wiley.com/doi/10.1002/hec.4652
[2057]
A commonplace reason for using marijuana in Ptuj is as an exit drug.
Even without any LSD or mushrooms, a proportion of the
alcoholically-inclined realise at some point that things are not
getting better. When you go drinking, it starts out good and goes
downhill from there. Perhaps if I have some more it will get even
better. It doesn't. In the long run most fortunately realise that the
alcohol sweet spot really only lasts a very short time, and the older
you get the shorter that sweet spot is.
If you want to use marijuana as an exit drug that's not a medical
issue. You didn't need a prescription to get the drug that caused the
problem, but you can't get one for the cure, because it's illegal.
Clearly this interferes with the desire of the self-aware person in
trouble with alcohol who wants an easy path to harm
reduction."
A 2021 paper from Scripps Research Institute and the University of
California report, which only looked at CBD, reports:
"Cannabidiol reduces craving in animal models of alcohol and cocaine
use."
because...
"CBD prevented rats from exhibiting somatic signs of withdrawal and
hyperalgesia during acute and protracted abstinence. There was no
dose-response observed for CBD, suggesting a ceiling effect at the
doses used and the potential for lower effective doses of
CBD."
https://pubmed.ncbi.nlm.nih.gov/33909102/
[839]
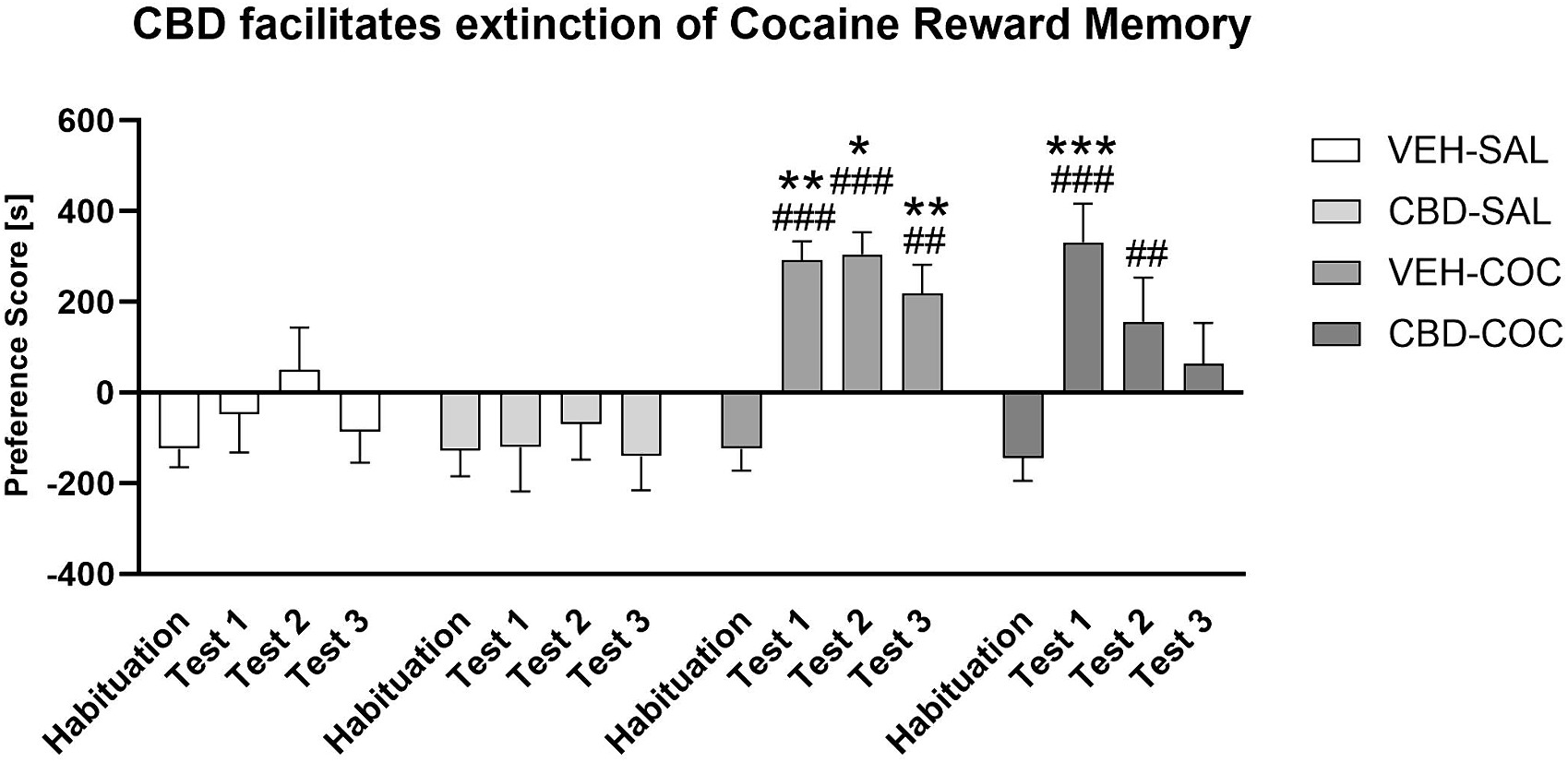
"Cannabidiol (CBD) facilitates cocaine extinction and ameliorates
cocaine-induced changes to the gut microbiome in male C57BL/6JArc
mice" say Chesworth et al (2024).
"Cocaine use disorder (CUD) is a global health problem with no
approved medications. One potential treatment target is the gut
microbiome, but it is unknown if cocaine induces long-lasting effects
on gut microbes. A novel therapeutic candidate for CUD, cannabidiol
(CBD), can improve gut function in rodent models. It is possible that
protective effects of CBD against cocaine use are mediated by
improving gut health. We examined this question in this experiment.
Cocaine conditioned place preference (CPP) was conducted in adult male
C57BL/6JArc mice. Mice were treated with vehicle or 20 mg/kg CBD prior
to all cocaine CPP sessions (N = 1113/group). Mice were tested drug
free 1, 14 and 28 days after cessation of cocaine and CBD treatment.
Fecal samples were collected prior to drug treatment and after each
test session. Gut microbiome analyses were conducted using 16 s rRNA
sequencing and correlated with behavioural parameters. We found a
persistent preference for a cocaine-environment in mice, and
long-lasting changes to gut microbe alpha diversity. Cocaine caused
persistent changes to beta diversity which lasted for 4 weeks. CBD
treatment reduced cocaine-environment preference during abstinence
from cocaine and returned gut beta diversity measures to control
levels. CBD treatment increased the relative abundance of Firmicutes
phyla and Oscillospira genus, but decreased Bacteroidetes phyla and
Bacteroides acidifaciens species. Preference score in cocaine-treated
mice was positively correlated with abundance of Actinobacteria,
whereas in mice treated with CBD and cocaine, the preference score was
negatively correlated with Tenericutes abundance. Here we show that
CBD facilitates cocaine extinction memory and reverses persistent
cocaine-induced changes to gut microbe diversity. Furthermore, CBD
increases the abundance of gut microbes which have anti-inflammatory
properties. This suggests that CBD may act via the gut to reduce the
memory of cocaine reward. Our data suggest that improving gut health
and using CBD could limit cocaine abuse."
https://www.sciencedirect.com/science/article/pii/S0278584624000824?via%3Dihub
[3360]
Prohibition, if observed, makes it harder for people giving up
smoking and cocaine.
The Defence anticipates the Court will be interested in obsessive
craving. As Bnsch et al reveal in Human Molecular Genetics in 2005,
"Various studies have linked alcohol dependence phenotypes to
chromosome 4. One candidate gene is NACP (non-amyloid component of
plaques), coding for alpha synuclein. Recently, it has been shown that
alpha synuclein mRNA is increased in alcohol-dependent patients within
withdrawal state. This increase is significantly associated with
craving, especially obsessive craving. On the basis of these
observations, the present study analysed two polymorphic repeats
within the NACP gene. We found highly significant longer alleles of
NACP-REP1 in alcohol-dependent patients compared with healthy controls
(KruskalWallis test, χ2=99.5; df=3, P<0.001). In addition,
these lengths significantly correlate with levels of expressed alpha
synuclein mRNA (χ2=8.83; df=2, P=0.012). The present results point
to a novel approach for a genetic determination of craving, a key
factor in the genesis and maintenance not only of alcoholism but also
of addiction in general."
https://academic.oup.com/hmg/article/14/7/967/626665?login=false
[2978]
According to Hallbeck et al (2024) "Accumulation of alpha-synuclein
pathology in the liver exhibits post-translational modifications
associated with Parkinsons disease"
"In previous work, we showed that human hepatocytes can take up
α-syn assemblies via the gap junction protein connexin-32
(Cx32). Furthermore, we found an age-dependent accumulation of human
α-syn pathology within the liver in multiple animal models of PD
(L61, (Thy-1)-h[A30P])), and MSA (MBP29). Importantly, the
accumulation of α-syn within the liver was not due to hepatic
mRNA expression, indicating that α-syn deposits are derived
directly from the brain or indirectly from other peripheral tissues.
Moreover, we corroborated that α-syn pathology in
neuropathologically confirmed PD cases can be found to a higher degree
than in controls with no α-syn pathology in the brain. In the
current report, we investigated the presence of α-syn
post-translational modifications (PTMs) in the liver from aged
(Thy-1)-h[A30P] mice (A30P). We now report the presence of hallmark
PTMs associated with PD, including tyrosine nitration (nY39),
phosphorylation (pY39, pS87 and pS129, Y133) and C-terminal truncation
events (X-122). Ex vivo, we demonstrate that human hepatocytes (HuH-7)
degrade pre-formed fibrils (PFF) more efficiently than oligomeric
assemblies. However, by increasing autophagy using the pharmacological
inhibitor rapamycin, we could enhance oligomeric α-syn
degradation in a concentration-dependent manner. Moreover, ex vivo we
also observe several PTMs that have been demonstrated in vivo. Taken
together, our results demonstrate the presence of key pathological
modifications associated with PD, also present in the liver of a mouse
model of PD. Our findings suggest that α-syn aggregates are
transported from the brain to the liver in a modified state or upon
arrival, they undergo specific PTMs to facilitate their clearance and
detoxification, suggesting a new role for the liver in the clearance
of PD-associated pathology."
https://www.cell.com/iscience/fulltext/S2589-0042(24)02675-0
[3903]
What are the effects of cannabis on synuclein?
In "The Neuroprotective Effects of Cannabis-Derived Phytocannabinoids
and Resveratrol in Parkinsons Disease: A Systematic Literature Review
of Pre-Clinical Studies" (2021) by Prakash and Carter:
"A total of 1034 publications were analyzed, of which 18 met the
eligibility criteria for this review. Collectively, the majority of PD
rodent studies demonstrated that treatment with CDCs or RSV produced a
significant improvement in motor function and mitigated the loss of
dopaminergic neurons. Biochemical analysis of rodent brain tissue
suggested that neuroprotection was mediated by anti-oxidative,
anti-inflammatory, and anti-apoptotic mechanisms. This review
highlights the neuroprotective potential of CDCs and RSV for in vivo
models of PD and therefore suggests their potential translation to
human clinical trials to either ameliorate PD progression and/or be
implemented as a prophylactic means to reduce the risk of development
of PD."
and
"Seven studies investigated the effects of RSV and CDCs on
neuroinflammation in rodent brain tissue of the striatum and SNpc, and
included neurotoxin models, a genetic model, as well as specific
induction of neuroinflammation via LPS treatment. The results of these
studies are summarized in Table 6 and have been divided by their
intervention group (BCP [β-caryophyllene], THCV
[tetrahydrocannabivarin], and RSV [resveratrol]), and then ascending
year of study. Five studies showed increased markers of microglia and
astrocytes activation via quantification of glial fibrillary acidic
protein (GFAP) and ionized calcium-binding adaptor molecule 1 (Iba-1)
protein or mRNA levels, and these were significantly reduced via
administration of THCV, BCP, or RSV. Inflammatory protein markers and
their complementary mRNA levels were significantly increased in the PD
model groups and this was significantly countered with BCP or RSV
treatment. The suppressor of cytokine signaling protein 1 (SOCS-1) was
detected in α-synuclein transgenic mice and was significantly
upregulated by RSV treatment."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8699487/
[2979]
In "Neuroprotective effects of cannabidiol on dopaminergic
neurodegeneration and α-synuclein accumulation in C. elegans
models of Parkinson's disease" (2022) Muhammad et al found
that:
"CBD at 0.025 mM (24.66 %), 0.05 mM (52.41 %) and 0.1 mM (71.36 %)
diminished DA neuron degenerations induced by 6-hydroxydopamine
(6-OHDA), reduced (0.025, 27.1 %), (0.05, 38.9 %), (0.1, 51.3 %)
food-sensing behavioural disabilities in BZ555, reduced 40.6 %, 56.3
%, 70.2 % the aggregative toxicity of α-Syn and expanded the
nematodes' lifespan up to 11.5 %, 23.1 %, 28.8 %,
dose-dependently....these findings supported CBD as an
anti-parkinsonian drug and may exert its effects by raising lipid
depositions to enhance proteasome activity and reduce oxidative stress
via the antioxidative pathway."
https://pubmed.ncbi.nlm.nih.gov/36108815/
[2980]
In Sao Paulo, Erustes et al (2025) found "Cannabidiol induces
autophagy via CB1 receptor and reduces α-synuclein cytosolic
levels":
"To investigate the participation of each cannabinoid receptor in the
induction of autophagy, cells were treated with selective cannabinoid
agonists that interact specifically with receptors of the human
endocannabinoid system. In this way, autophagic flux was evaluated in
cells treated with agonists and antagonists of cannabinoid receptors:
ACEA/AM251 (10 M/10 M, CB1R), GW405833/AM630 (1 M/3 M, CB2R) and
capsaicin/capsazepine (10 M/10 M, TRPV1). Cells were treated with
these compounds for 4 h both in the presence or absence of NH4Cl (10
mM added during the last hour of treatment), which is used as an
inhibitor of lysosomal degradation. In the groups treated with the
agonist and antagonist, the antagonists were added during the first 30
min, followed by the addition of the agonists.
"The evaluation of autophagic flux demonstrated that compared with
control cells and cells treated with ACEA [Arachidonoyl
2-chloroethylamide] in the absence of an inhibitor, cells stimulated
with ACEA in the presence of NH4Cl accumulated LC3-II (Fig. 3a).
Autophagic flux was inhibited when cells were treated with ACEA in the
presence of AM251 (a CB1R antagonist); in this way, the addition of an
antagonist blocked the effect of the agonist on the induction of
autophagy."
https://www.sciencedirect.com/science/article/pii/S0006899324006693?via%3Dihub
[3831]
Wang et al (2022) also found that:
"Cannabidivarin alleviates α-synuclein aggregation via DAF-16 in
Caenorhabditis elegans"
https://faseb.onlinelibrary.wiley.com/doi/abs/10.1096/fj.202200278RR
[2981]
"DAF-16 is the sole ortholog of the FOXO family of transcription
factors in the nematode Caenorhabditis elegans....The gene has played
a large role in research into longevity and the insulin signalling
pathway as it is located in C. elegans, a successful ageing model
organism."
https://en.wikipedia.org/wiki/Daf-16
[2984]
These studies point to the conclusion that cannabinoids inhibit
synuclein. Therefore they reduce cravings as well as inhibiting
neuroinflammatory pathways:
"Glycine receptors are expressed mainly in Purkinje cells. In
hyperammonemic rats, enhanced glycinergic neurotransmission leads to
reduced membrane expression of ADAM17, resulting in increased surface
expression and activation of TNFR1 and of the associated NF-kB
pathway. This increases the expression in Purkinje neurons of TNFa,
IL-1b, HMGB1, and glutaminase. Increased glutaminase activity leads to
increased extracellular glutamate, which increases extracellular GABA.
Increased extracellular glutamate and HMGB1 potentiate microglial
activation. Blocking glycine receptors with strychnine or
extracellular cGMP completely prevents the above pathway in
hyperammonemic rats."
And rats in this condition were used to test this because:
"Rats with chronic hyperammonemia reproduce the cognitive impairment
and motor in-coordination shown by cirrhotic patients with minimal
hepatic encephalopathy and are a good model to identify the underlying
mechanisms and to test treatments to improve them. Chronic
hyperammonemia induces neuroinflammation which alters glutamatergic
and GABAergic neurotransmission in cerebellum and hippocampus leading
to cognitive and motor impairment.
https://jneuroinflammation.biomedcentral.com/articles/10.1186/s12974-020-01941-y
[3832]
Wang et al (2022) also found that:
"Cannabidivarin alleviates α-synuclein aggregation via DAF-16
in Caenorhabditis elegans"
https://faseb.onlinelibrary.wiley.com/doi/abs/10.1096/fj.202200278R
[2981]
"DAF-16 is the sole ortholog of the FOXO family of transcription
factors in the nematode Caenorhabditis elegans....The gene has played
a large role in research into longevity and the insulin signalling
pathway as it is located in C. elegans, a successful ageing model
organism."
https://en.wikipedia.org/wiki/Daf-16
[2984]
These studies point to the conclusion that cannabinoids inhibit
synuclein. Therefore they reduce cravings as well as inhibiting
neuroinflammatory pathways. As Arenas et al (2020) of the Prncipe
Felipe Research Center in Valencia explain:
"Glycine receptors are expressed mainly in Purkinje cells. In
hyperammonemic rats, enhanced glycinergic neurotransmission leads to
reduced membrane expression of ADAM17, resulting in increased surface
expression and activation of TNFR1 and of the associated NF-kB
pathway. This increases the expression in Purkinje neurons of TNFa,
IL-1b, HMGB1, and glutaminase. Increased glutaminase activity leads to
increased extracellular glutamate, which increases extracellular GABA.
Increased extracellular glutamate and HMGB1 potentiate microglial
activation. Blocking glycine receptors with strychnine or
extracellular cGMP completely prevents the above pathway in
hyperammonemic rats."
And rats in this condition were used to test this because:
"Rats with chronic hyperammonemia reproduce the cognitive impairment
and motor in-coordination shown by cirrhotic patients with minimal
hepatic encephalopathy and are a good model to identify the underlying
mechanisms and to test treatments to improve them. Chronic
hyperammonemia induces neuroinflammation which alters glutamatergic
and GABAergic neurotransmission in cerebellum and hippocampus leading
to cognitive and motor impairment.
https://jneuroinflammation.biomedcentral.com/articles/10.1186/s12974-020-01941-y
[3832]
In the main, however, study of alpha-synucleinopathies is focussed on
PD. A summary of the findings around alpha-synuclein can be found in
Table 1 (PD), and other alpha-synucleinopathies in "Peripheral Tissues
as a Possible Marker for Neurological Diseases and Other Medical
Conditions" by Jimnez-Jimnez et al (2023).
https://www.researchgate.net/publication/373232996_Alpha-Synuclein_in_Peripheral_Tissues_as_a_Possible_Marker_for_Neurological_Diseases_and_Other_Medical_Conditions/link/64e191cd14f8d173380c05fe/download[2982]
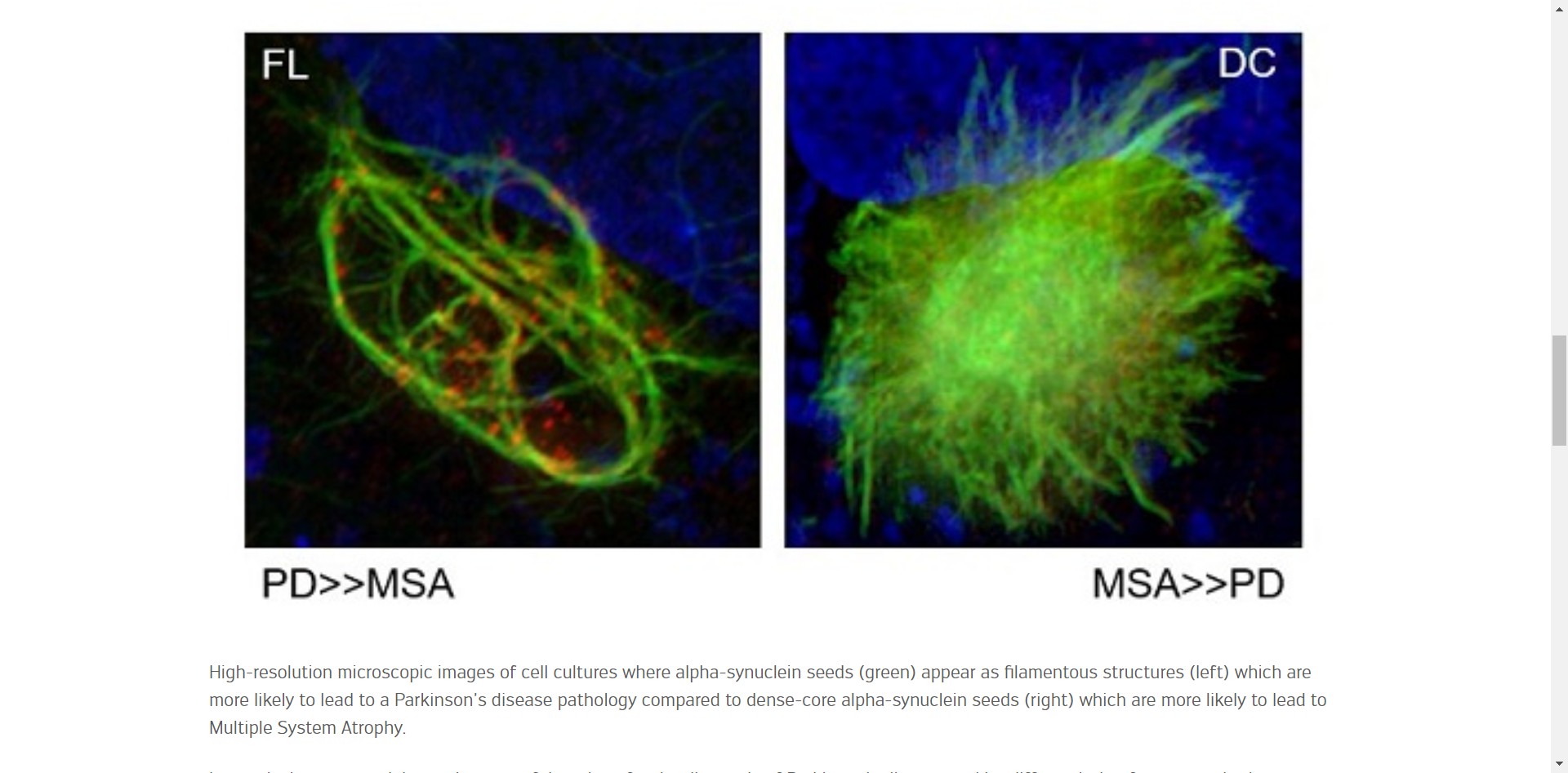
Here we can see the difference between PD and MSA [multiple system
atrophy] filamentous structures which was found to be significant
enough for a distinguishing diagnosis.
Says Prof. Nobutaka Hattori, at the Department of Neurology of
Juntendo University and current head of the Neurodegenerative
Disorders Collaboration Laboratory at RIKEN Centre for Brain
Science,
"'Our team has also discovered, for the first time, that these
α-synuclein seeds have structures and properties characteristic
of each disease, suggesting that they shape the pathology of each
synucleinopathy.'"
https://www.uni.lu/en/news/ground-breaking-discovery-for-diagnosing-neurodegenerative-diseases/
[2983]
How many person years have been lost to alpha-synucleinopathies due
to cannabis prohibition? The Defence believes it is lots. More than
zero.
In a study published in Drug Alcohol Dependency by Cano, Oh et al
(2022)
"Peer-reviewed studies and doctoral dissertations published in
English between 1990 and July 19, 2022 were identified from PubMed,
Web of Science, ProQuest Dissertations & Theses, PsycINFO, CINAHL,
and EconLit. Eligible studies examined at least one county-level
predictor of drug overdose mortality in US counties."
and
"Of 56 studies included, 42.9% were subnational, and 53.6% were
limited to opioid overdose. In multiple studies, measures related to
opioid prescribing, illness/disability, economic distress, mining
employment, incarceration, family distress, and single-parent families
were positively associated with drug overdose mortality outcomes,
while measures related to cannabis dispensaries, substance use
treatment, social capital, and family households were negatively
associated with drug overdose mortality outcomes."
https://www.sciencedirect.com/science/article/abs/pii/S0376871622004513?via%3Dihub
[1823]
Patients undergoing primary THA (total hip arthroplasty) or TKA
(total knee arthroplasty) with minimum 6-month follow-up who
self-reported cannabis use were retrospectively reviewed. A total of
210 patients (128 TKAs and 82 THAs) were matched by age; gender; type
of arthroplasty. Self-reported perioperative cannabis use appeared to
significantly reduce the number of patients that persistently used
opioids greater than 90 days after TJA from 9.5% to 1.4%.
[P<.001]
With cannabis, three patients instead of 20 showed persistent opioid
use.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9493281/
[1824]
In "Use of Cannabis for Harm Reduction Among People at High Risk for
Overdose in Vancouver, Canada (20162018)" Mok et al (2021) report that
it's a common strategy for people trying to recover:
"We drew data about recent cannabis use and intentions from 3
prospective cohort studies of marginalized people who use drugs based
in Vancouver, Canada, from June 2016 to May 2018. The primary outcome
was use of cannabis for harm reduction, defined as using cannabis for
substitution for licit or illicit substances such as heroin or other
opioids, cocaine, methamphetamine, or alcohol; treating withdrawal; or
coming down off other drugs.
"Results. Approximately 1 in 4 participants reported using cannabis
for harm reduction at least once during the study period. The most
frequent reasons included substituting for stimulants (50%) and
substituting for illicit opioids (31%)."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8033988/
[3149]
Another meth study "Cannabidiol mechanism of action on modulating
extinction and reinstatement of methamphetamine-seeking behavior:
Targeting D2-like dopamine receptors in the hippocampus" by Omidiani
et al (2025):
"Multiple lines of evidence suggest that CBD exerts its effects by
modulating the mesocorticolimbic dopamine system. D2-like receptors in
the CA1 region of the hippocampus play a significant role in relaying
memory and emotional signals related to the processing of drug-related
cues. Therefore, this study aims to investigate the role of CA1
D2-like receptors in mediating the effects of CBD on METH-seeking
behavior during extinction and reinstatement in the conditioned place
preference (CPP) model. For this purpose, rats were administered
various doses of Sulpiride (0.25,1, or 4 μg/0.5 μl) as a D2-like
receptor antagonist before intracerebroventricular (ICV) injection of
CBD (10 μg/5 μl) during a 10-day extinction period.
Additionally, a separate group of rats received Sulpiride (0.25,1, or
4 μg/0.5 μl) before a single CBD injection (50 μg/5 μl) on
the reinstatement day. The findings indicated that Sulpiride (1 and 4
μg) significantly attenuated CBD's acceleration of METH-CPP
extinction (p < 0.01 and p < 0.05, respectively). Moreover,
Sulpiride (1 and 4 μg) during the reinstatement phase notably
reversed CBD's preventive effects on the reinstatement of
reward-seeking behavior (p < 0.05 and p < 0.001, respectively).
In summary, these results suggest that CBD's ability to shorten the
extinction period and suppress METH reinstatement is partially
mediated through interactions with D2-like dopamine receptors in the
CA1 region of the hippocampus. These findings offering insight into
more precise and effective interventions for METH use disorder."
https://www.sciencedirect.com/science/article/abs/pii/S0022395625004091
[5402]
Danesh et al (2025) conclude that "D1-like dopamine receptors in the
dentate gyrus mediate cannabidiol's facilitation of extinction and
prevention of reinstatement in methamphetamine-induced conditioned
place preference":
"Methamphetamine (METH) is a highly addictive psychostimulant, and
despite its widespread abuse, there are no FDA-approved treatments for
METH use disorder (MUD). Cannabidiol (CBD), a non-psychoactive
cannabinoid, has shown promise in reducing behaviors linked to
psychostimulant use, including METH. However, the underlying
neurobiological mechanisms remain unclear. Emerging evidence suggests
that CBD may act on the dopamine system to influence drug-seeking
behavior. D1-like dopamine receptors (D1Rs) in the hippocampus (HPC)
are involved in memory processes related to rewards, which may
contribute to CBD's effects. This study examined whether D1Rs in the
dentate gyrus (DG) region of the HPC play a role in CBD's modulation
of METH-induced conditioned place preference (CPP) during extinction
and reinstatement. Adult male Wistar rats received the D1Rs antagonist
SCH23390 (0.25, 1, and 4 μg/0.5 μl saline) into the DG region
before intracerebroventricular injection of CBD (10 and 50 μg/5
μl of 12 % DMSO). Results show that the highest dose of SCH23390 (4
μg) significantly blocked CBD's ability to enhance extinction of
METH-CPP. Moreover, SCH23390 (1 and 4 μg) reversed CBD's prevention
of reinstatement of METH-CPP. These findings suggest that D1Rs in the
DG region are involved in mediating CBD's effects and offer insights
into its therapeutic potential for MUD."
https://www.sciencedirect.com/science/article/abs/pii/S0091305725001418
[5403]
Balu et al (2021) report:
"Overall, the average change in prescribed opioid use was found to be
-12.3 morphine milligram equivalent (MME) units when including all
individuals (p < 0.00001)."
They break it down.
In this study, we examined individuals who were provided with legal;
medical cannabis certifications in the state of Delaware between June
2018 and October 2019 and were concurrently being treated with opioid
medications for chronic pain at a private pain management practice.
For non-outlier individuals with positive baseline opioid use before
receiving medical marijuana certification (n=63), the average percent
change in opioid use was found to be -31.3 percent. Examining
subgroups based upon pain location, individuals with low back pain
(n=58) displayed a 29.4 percent decrease in MME [morphine milligram
equivalent] units, while individuals with neck pain (n=27) were
observed to have a 41.5 percent decrease in opioid use. Similarly,
individuals with knee pain (n=14) reduced their opioid use by 32.6
percent. Since the underlying pathology and their source of pain in
the individuals was unlikely to significantly change during the period
examined, medical marijuana use could have played a large role in
allowing the individuals to decrease their opioid use."
https://www.cureus.com/articles/77114-medical-cannabis-certification-is-associated-with-decreased-opiate-use-in-patients-with-chronic-pain-a-retrospective-cohort-study-in-delaware
[1825]
More than a quarter of U.S. adults suffering from chronic pain have
turned to using cannabis to manage their discomfort, according to a
study published in JAMA Open Network.
Researchers at Michigan Medicine surveyed 1,661 adults last spring
with chronic pain who lived in one of the 36 states with active
medical cannabis programs and Washington, D.C.
About 26 percent of survey participants reported using cannabis
within the past year to manage pain, Bicket et al found.
Moreover:
"More than half of adults who used cannabis to manage their chronic
pain reported that use of cannabis led them to decrease use of
prescription opioid, prescription nonopioid, and over-thecounter pain
medications, and less than 1% reported that use of cannabis increased
their use of these medications (Figure 1). Fewer than half of
respondents reported that cannabis use changed their use of
nonpharmacologic pain treatments. Among adults with chronic pain in
this study, 38.7% reported that their used of cannabis led to
decreased use of physical therapy (5.9% reported it led to increased
use), 19.1% reported it led to decreased use of meditation (23.7%
reported it led to increased use), and 26.0% reported it led to
decreased used of cognitive behavioral therapy (17.1% reported it led
to increased use) (Figure 2)."
https://jamanetwork.com/journals/jamanetworkopen/articlepdf/2800119/bicket_2023_ld_220293_1671719838.02096.pdf [2011]
"Δ8-Tetrahydrocannabivarin has potent anti-nicotine effects in
several rodent models of nicotine dependence" revealed Xi et al in
2019:
"Both types of cannabinoid receptorsCB1 and CB2 regulate brain
functions relating to addictive drug-induced reward and relapse. CB1
receptor antagonists and CB2 receptor agonists have anti-addiction
efficacy, in animal models, against a broad range of addictive drugs.
Δ9-Tetrahydrocannabivarin (Δ9-THCV)a cannabis
constituentacts as a CB1 antagonist and a CB2 agonist.
Δ8-Tetrahydrocannabivarin (Δ8-THCV) is a Δ9-THCV
analogue with similar combined CB1 antagonist/CB2 agonist
properties.
"Experimental Approach: We tested Δ8-THCV in seven different
rodent models relevant to nicotine dependencenicotine
self-administration, cue-triggered nicotine-seeking behaviour
following forced abstinence, nicotine-triggered reinstatement of
nicotine-seeking behaviour, acquisition of nicotine-induced
conditioned place preference, anxiety-like behaviour induced by
nicotine withdrawal, somatic withdrawal signs induced by nicotine
withdrawal, and hyperalgesia induced by nicotine withdrawal.
"Key Results: Δ8-THCV significantly attenuated intravenous
nicotine self-administration and both cue‐induced and nicotine-induced
relapse to nicotine-seeking behaviour in rats. Δ8-THCV also
significantly attenuated nicotine-induced conditioned place preference
and nicotine withdrawal in mice."
and
"In summary, most studies on animal models for substance use
disorders reported some beneficial effects for the cannabinoids under
investigation, except for CBDA (see Fig. 3). Δ8-THCV showed
anti-nicotine-dependence properties, while CBN, Δ8-THC, and
11-OH-Δ8-THC appeared to reduce morphine-withdrawal symptoms.
Δ8-THC also seemed to have some capacity to inhibit the
reinstatement of METH-seeking behavior. CBDA was not effective in
reducing METH-induced or cocaine-seeking behaviors."
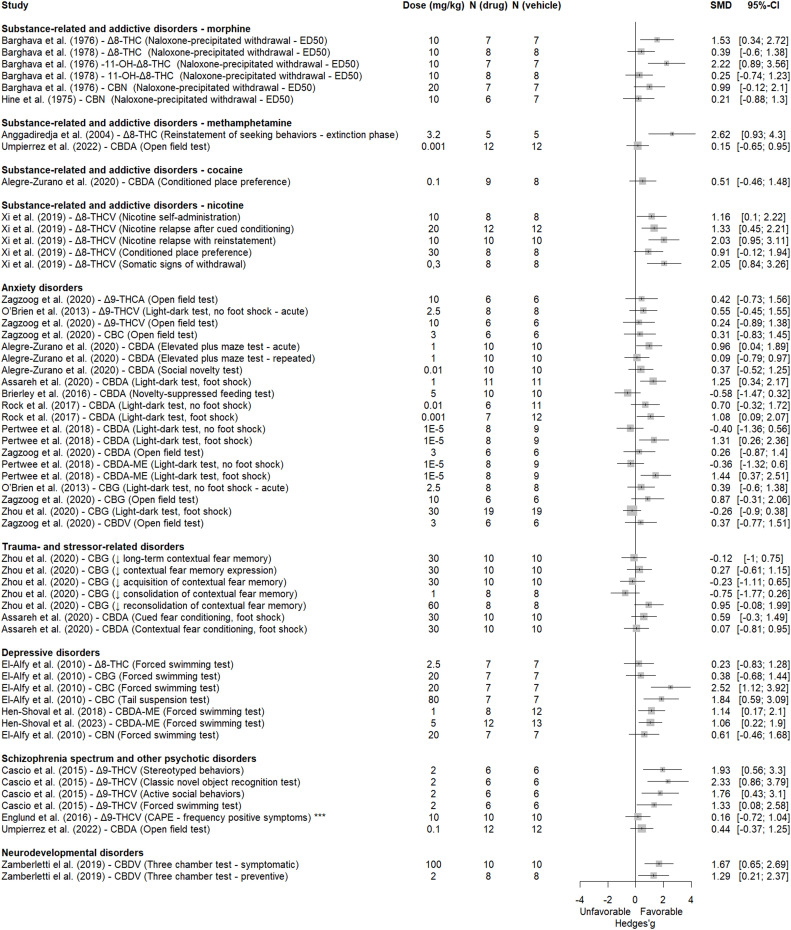
https://bpspubs.onlinelibrary.wiley.com/doi/pdfdirect/10.1111/bph.14844[3808]
Kitchen et al (2025) examined "Cannabis use and illicit opioid
cessation among people who use drugs living with chronic pain":
"Between June 2014 and May 2022, 2340 PWUD were initially recruited
and of those 1242 PWUD reported chronic pain, use of unregulated
opioids and completed at least two follow-up visits. Of these 1242
participants, 764 experienced a cessation event over 1038.2
person-years resulting in a cessation rate of 28.5 per 100
person-years (95% confidence interval [CI] 25.431.9). Daily cannabis
use was positively associated with opioid cessation (adjusted hazard
ratio 1.40, 95% CI 1.081.81; p = 0.011).
In the sex-stratified sub-analyses, daily cannabis use was
significantly associated with increased rates of opioid cessation
among males (adjusted hazard ratio 1.50, 95%
CI 1.092.08; p = 0.014)."
https://onlinelibrary.wiley.com/doi/abs/10.1111/dar.14014
[4794]
"Efficacy of cannabidiol alone or in combination with
Δ-9-tetrahydrocannabinol for the management of substance use
disorders: An umbrella review of the evidence" from Bertrand Redonnet
et al (2025)
"...searched PubMed, Web of Science and Epistemonikos databases for
SRs, with or without a meta-analysis, of randomized controlled trials
focusing on interventions dispensing CBD, alone or in combination with
THC, to treat SUDs, published from 1 January 2000 to 15 October
2024.
The results supported combined THC and CBD:
"22 SRs were included, 5 of which performed a meta-analysis. We found
mixed evidence regarding the efficacy of CBD to manage and treat SUDs.
Findings were interpreted in light of the quality of the SRs.
Nabiximols, which contains CBD and THC, demonstrated positive effects
on cannabis withdrawal and craving symptoms. Evidence supporting the
efficacy of CBD is limited and inconclusive for abstinence, reduction
or cessation of use of cannabis, tobacco, alcohol, opiates and other
psychoactive substances.
"Conclusion
Cannabidiol (CBD) monotherapy does not appear to be efficacious for
treatment of substance use disorders. CBD primarily exhibits effects
on cannabis withdrawal and craving when combined with
Δ-9-tetrahydrocannabinol (THC). Existing data on the efficacy of
CBD alone with regard to other outcomes related to substance use
disorders are limited."
https://onlinelibrary.wiley.com/doi/10.1111/add.16745
[4755]
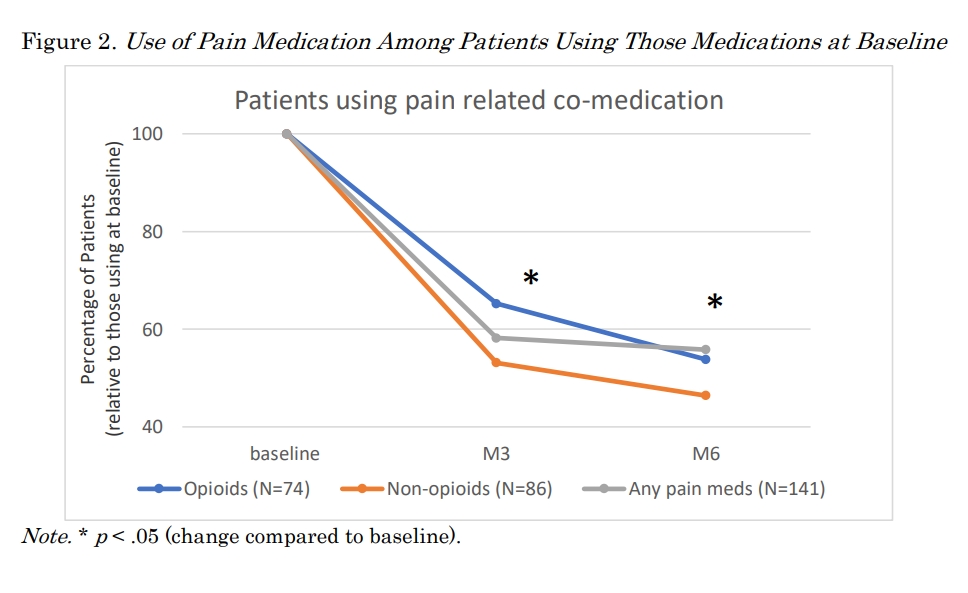
https://publications.sciences.ucf.edu/cannabis/index.php/Cannabis/article/download/239/169
[4767]
Several descriptive commentaries from opoid users fighting addiction
are featured in Ganesh et al (2024) "'Smoking weed it gets you over
the hump': Cannabis co-use as a facilitator of decreased opioid use
among people who inject drugs in Los Angeles, California" including
this one:
"Participants also described using cannabis to mitigate opioid
cravings after they had stopped regular use and were no longer
experiencing withdrawal symptoms. This person reported that it helped
them to 'get over the hump' of craving opioids and continue not to
use.
"'I was really trying to get off of opiates and using weed, really
helps to not have the first urge to use opiates. When you're addicted
and you have a habit, then you have to use opiates. But when you don't
have a habit and you're not getting sick from it every day, when
you're smoking weed it gets you over the hump and that urge to get
high for the first time. And that's what's so special out [sic] weed.'
(5115 26, Male, Housed)"
https://www.sciencedirect.com/science/article/pii/S2772724624000416
[5063]
Looking at "Recreational Cannabis Laws and Fills of Pain Prescriptions
in the Privately Insured" Steuart et al (2025) found no good cheer for
the manufacturers and distributors of opioids:
"Objective: Almost half of U.S. states have passed recreational
cannabis laws as of May 2024. While considerable evidence to date
indicates cannabis may be a substitute for prescription opioids in the
treatment of pain, it remains unclear if patients are treating pain
with cannabis alone or concomitantly with other medications.Method:
Using data from a national sample of commercially insured adults, we
examine the effect of recreational cannabis legalization (through two
sequential policies) on prescribing of opioids, NSAIDS, and other pain
medications by implementing synthetic control estimations and
constructing case-study level counterfactuals for the years 2007-2020.
Results: Overall, we find recreational cannabis legalization is
associated with a decrease in opioid fills among commercially insured
adults in the U.S., and we find evidence of a compositional change in
prescriptions of pain medications more broadly. Specifically, we find
marginally significant increases in prescribing of non-opioid pain
medications after recreational cannabis becomes legal in some states.
Once recreational cannabis dispensaries open, we find statistically
significant decreases in the rate of opioid prescriptions (13%
reduction from baseline, p<.05) and marginally significant
decreases in the average daily supply of opioids (6.3% decrease,
p<.10) and number of opioid prescriptions per patient (3.5%
decrease, p<.10). Conclusions: These results suggest that
substitution of cannabis for traditional pain medications increases as
the availability of recreational cannabis increases. There appears to
be a small shift once recreational cannabis becomes legal, but we see
stronger results once users can purchase cannabis at recreational
dispensaries.The decrease in opioids and marginal increase in
non-opioid pain medication may reflect patients substituting opioids
with cannabis and non-opioid pain medications, either separately or
concomitantly. Reductions in opioid prescription fills stemming from
recreational cannabis legalization may prevent exposure to opioids in
patients with pain and lead to decreases in the number of new opioid
users, rates of opioid use disorder, and related harms."
https://publications.sciences.ucf.edu/cannabis/index.php/Cannabis/article/view/268/181
[5073]
Carey et al (2025) created some junkie monkeys to test the "Effects
of Δ9-tetrahydrocannabinol (THC), cannabidiol (CBD), and THC:CBD
mixtures on behavioral and physiological signs of morphine withdrawal
in rhesus monkeys":
"Monkeys received escalating doses of morphine up to 3.2 mg/kg twice
daily. After at least 2 weeks of morphine treatment, saline was
substituted for morphine for 2 days. Behavioral and physiological
signs of opioid withdrawal, including blood pressure, heart rate, body
temperature, and activity were measured before and after
administration of THC (0.321.0 mg/kg), CBD (1017.8 mg/kg), mixtures of
THC (0.32 mg/kg) and CBD (1017.8 mg/kg), lofexidine (0.0320.32 mg/kg),
or vehicle. Discontinuing morphine treatment markedly increased
unusual tongue movements, a characteristic behavioral sign of opioid
withdrawal in monkeys, and all physiological signs. The largest THC
dose (1.0 mg/kg) decreased unusual tongue movements and heart rate,
and the largest lofexidine dose (0.32 mg/kg) decreased unusual tongue
movements, blood pressure, heart rate, and activity. CBD alone or with
THC had no significant effect. These data demonstrate that THC
attenuates some signs of opioid withdrawal; however, THC was not more
effective than the currently available medication lofexidine."
https://www.sciencedirect.com/science/article/abs/pii/S0022356525398848
[5326]
In "Cannabis Use, Problem-Gambling Severity, and Psychiatric
Disorders: Data from the National Epidemiological Survey on Alcohol
and Related Conditions" (2019) Hammond et al
"... examined data from the first wave (20012002) of the National
Epidemiological Survey on Alcohol and Related Conditions (NESARC), a
large, national survey of non-institutionalized U.S. adults, to
examine relationships between problem-gambling severity and
psychopathology in individuals with and without cannabis use. At the
time of data collection of the first wave of the NESARC, medical
cannabis use had been legalized in eight states; however, its
recreational or non-medical use had not been legalized in any state.
In addition, prevalence estimates of past-year use during this time
period has ranged from 4.1% (Hasin et al., 2015) to 11% (Azofeifa,
Mattson, Schauer, McAfee, Grant, & Lyerla, 2016). "In all cases,
associations between problem-gambling severity and psychopathologies
were weaker among the lifetime-cannabis-using group as compared to the
never-using group.. Cannabis use moderates the relationships between
problem-gambling severity and psychiatric disorders, with cannabis use
appearing to account for some of the variance in the associations
between greater problem-gambling severity and specific forms of
psychopathology."
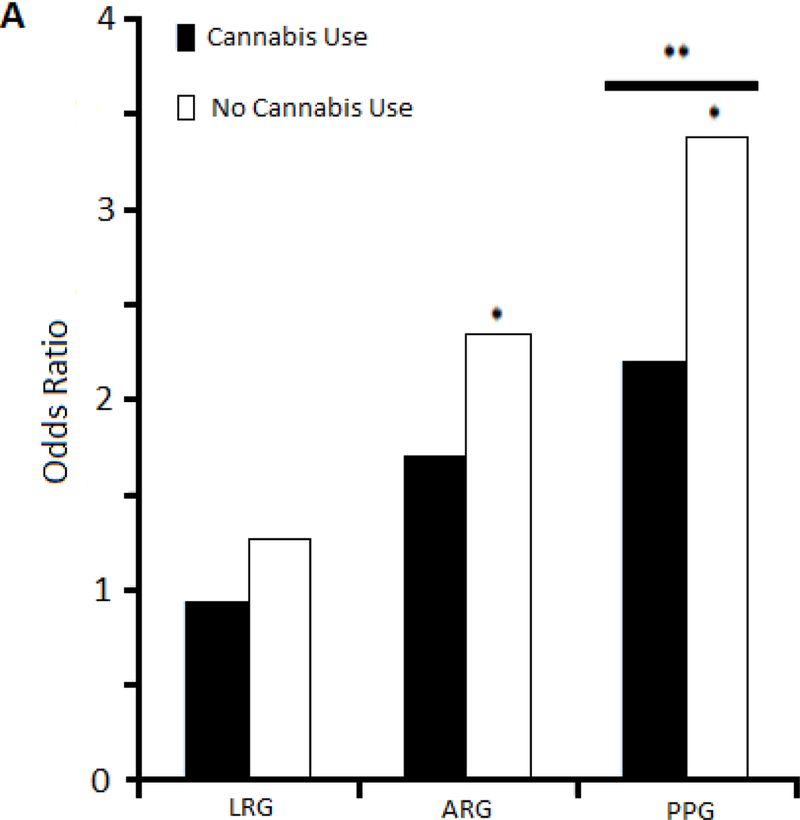
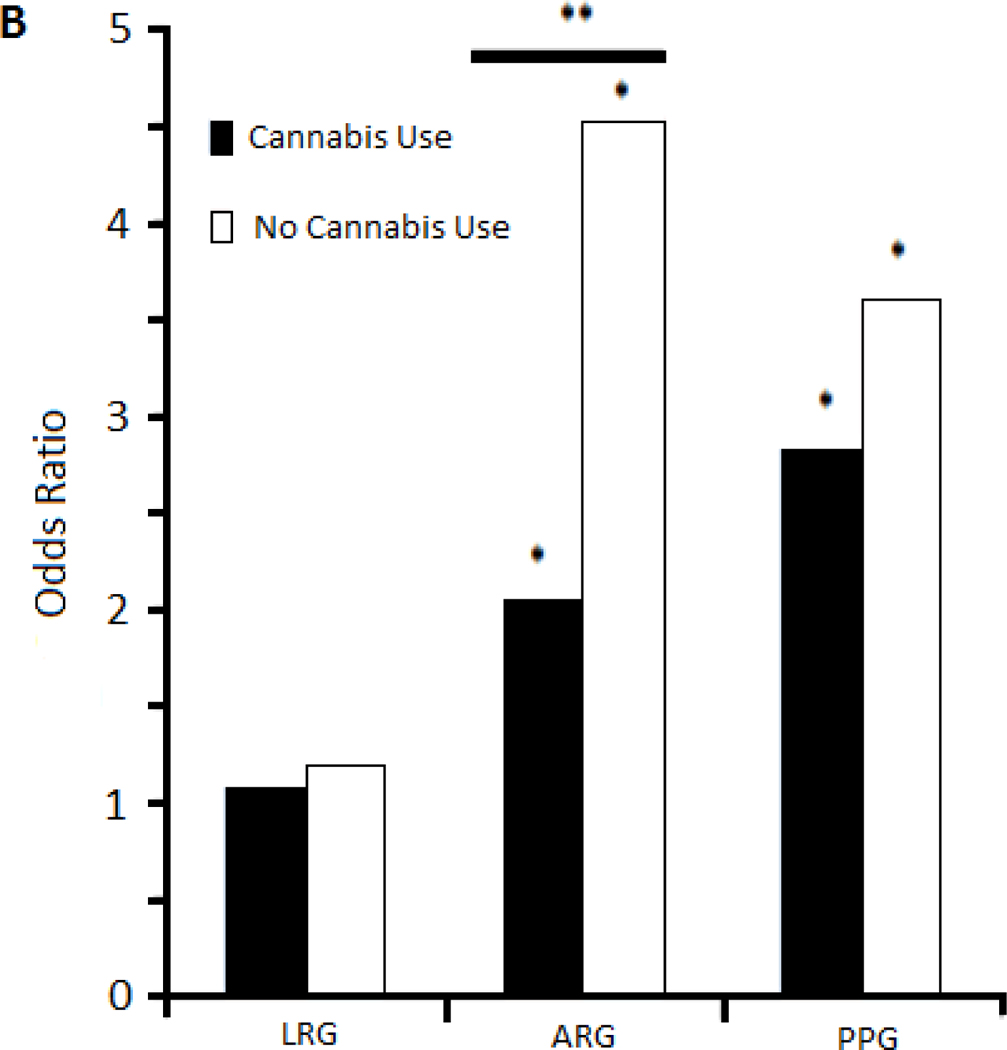
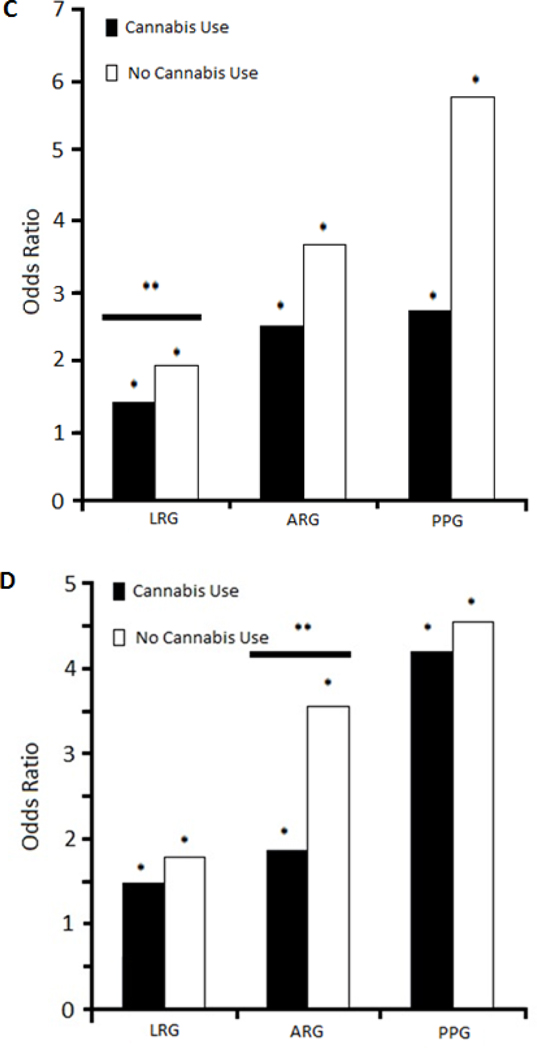
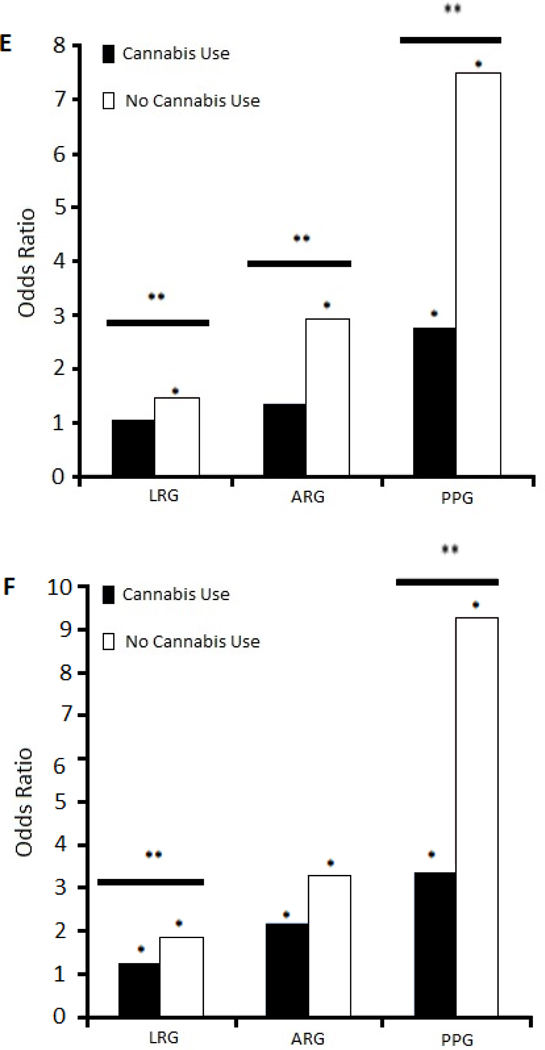
"Associations between problem-gambling severity and psychopathology
among lifetime-cannabis-using and never-using groups. Figures compare
odds ratios for specific disorders in association with low-risk
gambling (LRG), at-risk gambling (ARG), and problem/pathological
gambling (PPG), using of non-gambling/low frequency gambling as a
reference group. Specific disorders are those as follows: A.
Interactions with cannabis use in the associations between major
depression and problem-gambling severity. B. Interactions with
cannabis use in the associations between panic disorder and
problem-gambling severity. C. Interactions with cannabis use in the
associations between alcohol abuse/dependence and problem-gambling
severity. D. Interactions with cannabis use in the associations
between nicotine dependence and problem-gambling severity. E.
Interactions with cannabis use in the associations between cluster A
personality disorder and gambling severity. F. Interactions with
cannabis use in the associations between cluster B personality
disorders and problem-gambling severity. * Indicates statistically
significant odds ratios at p<0.05. ** Indicates statistically
significant interactions at p<0.05."
and
"Furthermore, cannabis-use status moderated the relationships
problem-gambling severity and specific psychiatric disorders including
major depression, panic disorder, alcohol-use disorders, nicotine
dependence, cluster A PDs (especially paranoid PD), and cluster B PDs
(especially antisocial PD)."
However Dr Hammond, who has
"...received support from the American Psychiatric Association Child
& Adolescent Fellowship, an unrestricted education grant supported
by Shire Pharmaceuticals and the American Academy of Child &
Adolescent Psychiatry Pilot Research Award for Junior Investigators
supported by Lilly USA, LLC. Dr. Marc Potenza has received financial
support or compensation for the following: Dr. Potenza has consulted
for and advised Shire, INSYS, RiverMend Health, Opiant/Lakelight
Therapeutics, and Jazz Pharmaceuticals; has received unrestricted
research support from Mohegan Sun Casino and grant support from the
National Center for Responsible Gaming"
...tries to highlight cannabis in problem gambling, his own Figure 1
tells the real story. Even under prohibition conditions, it was
another blow for NECUD/SPUK sufferers, who were worse at gambling and
at being crazy too.
I've used my incredible graphics skills to show how the anti-cannabis
woowoo is favoured by the layout of the histograms in Figure
1.
Please compare
...which charts interactions with cannabis use in the associations
between major depression and problem-gambling severity for low-risk
gambling (LRG), at-risk gambling (ARG), and problem/pathological
gambling (PPG groups), with
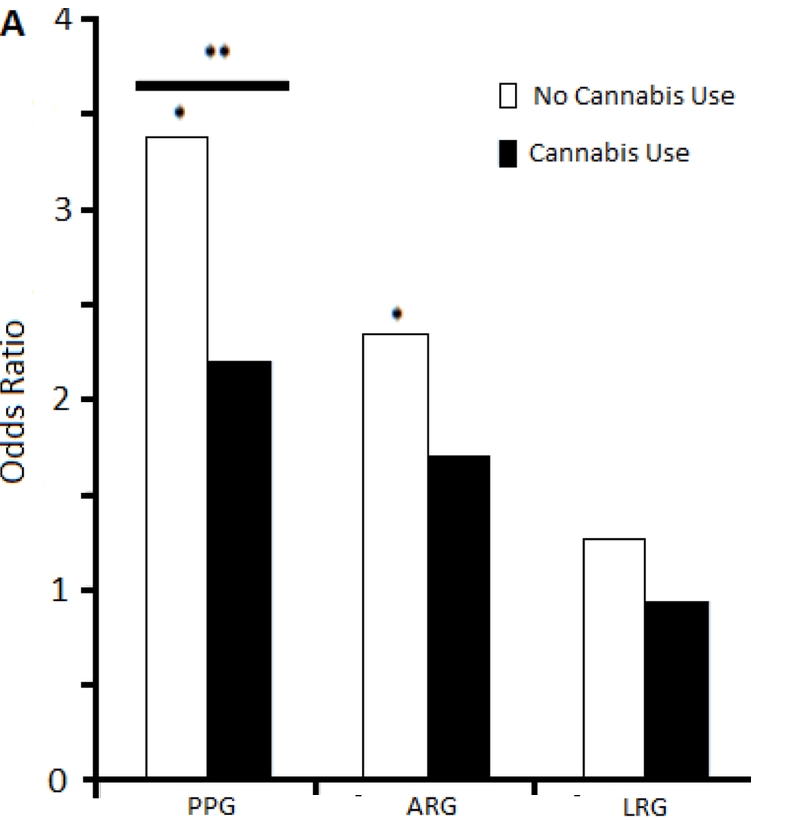
...a left to right mirror image of 1A. You can see cannabis looks
much better now, and we have begun with the most serious problem
gamblers and worked our way downwards. I have not done mirror images
for charts B-F, I'm sure the Court can imagine that for
itself.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6933114
[2711]
Another survey, published in JAMA Psychiatry by Grubbs and Kraus in
2024, found a relationship between problem drinking and problem
gambling:
"A total of 4363 respondents were included (51.4% men, 46.4% women,
and 2.2% nonbinary or other; mean [SD] age, 49.6 [16.2] years) (Table
1). The national census-matched survey consisted of 2806 participants
(mean [SD] age, 48.9 [17.2] years; 1365 [48.6%] men and 1441 [51.4%]
women; response rate, 2806 of 3203 [87.6%]). The oversample of sports
gamblers consisted of 1557 participants (mean [SD] age, 41.7 [15.3]
years; 1043 [67.0%] men and 514 [33.0%] women; response rate, 1557 of
1978 [78.7%]), of whom 1474 reported past year sports betting.
Additionally, in the national sample, 338 respondents (12.0%)
indicated they had gambled on sports in the past 12 months, resulting
in a total of 1812 sports gamblers (Table 1). Sports gamblers were
disproportionally likely to be men and younger. In these combined
samples, 3267 respondents (74.9%) reported past year alcohol use.
Sports wagerers were disproportionately more likely to report binge
drinking at monthly or greater frequency over the past 12 months and
were also disproportionately less likely to report no binge drinking
episodes in the past 12 months (Table 1). Multinomial logistic
regressions adjusted for age and race and ethnicity showed that sports
gamblers were substantially more likely to report higher levels of
binge drinking (Table 2), suggesting that elevated risky drinking
episodes among sports gamblers are not due to demographic
differences."
https://jamanetwork.com/journals/jamanetworkopen/articlepdf/2816784/grubbs_2024_ld_240031_1710953595.81812.pdf
[3483]
In view of the foregoing, we should not be surprised if "Expectancy
of impairment attenuates marijuana-induced risk taking"
(2017):
"Participants (N=136) were regular marijuana users. A balanced
placebo design (BPD) was used crossing marijuana administration (i.e.,
0% Tetrahydrocannabinol (THC) vs. 2.8% THC) with stimulus expectancy
(i.e., Told Placebo vs. Told THC). Marijuana outcome expectancies were
measured by self-report and dependent measures including a number of
behavioral impulsivity tasks and the balloon analogue risk task
(BART). ResultsAmong participants who received THC, higher
expectancies for cognitive-behavioral impairment (CBI) were related to
lower risk-taking on the BART. Among those who received placebo, there
was no association between CBI expectancies and BART performance. CBI
expectancies did not moderate drug effect on the BART and drug or
stimulus expectancy effects on impulsivity measures."
https://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC5796549&blobtype=pdf
[2712]
"Treating alcoholism by cannabis substitution creates a different
doctor-patient relationship," says Mikuriya.
"Patients seek out the physician to confer legitimacy on what they are
doing or are about to do. My most important service is to end their
criminal status, Aeschalapian protection from the criminal justice
system, which often brings an expression of relief. An alliance is
created that promotes candor and trust. The physician is permitted to
act as a coach or an enabler in a positive sense."
[3822]
Summarising the criteria for any substitution "treatment"...
"1. It should reduce alcohol use and related harms.
"2. It should ideally be free of harms, or at least less harmful than
alcohol.
"3. Misuse should be less than that of alcohol.
"4. It should be shown that it can substitute for alcohol and not be
used along with alcohol.
"5. It should be safer in overdose than alcohol.
"6. It should ideally not potentiate the effects of alcohol especially
if either drug is taken in overdose.
"7. It should offer significant health economic benefits."
...Chick and Nutt (2012) found six criteria wholly satisfied by
cannabis, while one (number 6) was partially satisfied, due to
disagreement on whether it potentiates alcohol. The answer to that is,
only if you drink alcohol. For details see Subbaraman's Table 1.
https://pmc.ncbi.nlm.nih.gov/articles/PMC3992908/
[3823]
Cannabis legalisation in Slovenia can be expected to reduce morbidity,
mortality and costs related to tobacco use. According to a survey of
9003 subjects by Pravosud et al (2024)
"In this longitudinal study, a web-based survey was administered to a
nationally representative, population-based panel of US adults in
2017, 2020, and 2021. We used weighted unadjusted binomial logistic
GEE models to assess changes in prevalence of cannabis,
tobacco/nicotine use and co-use and weighted, adjusted binary logistic
GEE models to assess associations of cannabis legalization with
cannabis, tobacco/nicotine use and co-use."
"Between 2017 and 2021 current cannabis use increased +3.3 % and was
higher in states with medical and recreational cannabis.
"Recreational cannabis legalization increased the odds of current
cannabis use by 1.13 times above the effect of medical
legalization.
"Current tobacco use declined −1.9 %, but this change was not
associated with legalization."
https://www.sciencedirect.com/science/article/pii/S0955395924003025?via%3Dihub
[4810]
----------------------------------------------------------------------------
The Englishman stands for the rights of everyone disadvantaged,
discriminated against, persecuted, and prosecuted on the false or
absent bases of prohibition, and also believes the victims of these
officially-sanctioned prejudices have been appallingly treated and
should be pardoned and compensated.
The Englishman requests the return of his
CaPs
and other rightful property, for whose distraint Slovenia has
proffered no credible excuse or cause.
The Benedictions represent both empirical entities as well as
beliefs. Beliefs which the Defence evidence shows may be reasonably
and earnestly held about the positive benefits of CaPs at the
population level, in which the good overwhelmingly outweighs the
bad. Below, the latest version of this dynamic list.
THE BENEDICTIONS
REFERENCES
TIMELINE OF DRUG LAW v. SCIENCE