PROHIBITION'S FRIENDS AND ENEMIES
Whose side are you on? - prejudice and quasilegality - racism - legal
amnesia - bullying - creativity - period pains - various pills and
potions - statins - cholesterophobia - spines good and bad - the
stress agenda - alcohol - psychiatrists - doctors - fat profits -
other prescription drugs - work accidents - driving - alcohol
substitution - donors - medical fraud - vix medicatrix naturae -
stigma - scientific neutrality - crime - lawyers
As a social construct, prohibition has social allies and social
antagonists. Its unpleasant effects create or at least exacerbate
prejudice. It does not deal in details nor in the big picture. Instead
tribes form around the poles of the social construct - police vs.
people, rich vs. poor, intellect vs. violence.
A neutral assessment of prohibition requires conditions unlikely to
pertain: equal resources, no fear of being honest, and not being a
member of one tribe or the other. History is littered with political
movements which did evil, but with good intentions. You could say
Hitler had good intentions. Lenin meant well. The best we can do is to
be professional and objective, and ask cui bono?
An approach to this is to examine who and what are the friends, and
enemies, of prohibition.
SUMMARY OF PROHIBITION'S FRIENDS: Racists, scapegoaters, plunderers,
religious nuts, painkiller sellers, insulin sellers, atypical
antipsychotic sellers, tummyache remedy sellers, big pharma,
medicofinancial bloat, "good vs. bad euphoria", overdoses and overdose
deaths, supporters of alcohol, poverty, pain, irrationality, obesity,
PTSD, cancer, stigma, witch-hunts as a mode of politicking, prejudice,
puritanism, the stress agenda, plastic rope, plastic clothing, and low
risk police hours.
SUMMARY OF THE ENEMIES OF PROHIBITION: vis medicatrix naturae,
ghrelin, enhanced consciousness, creativity, ineffable experiences,
many positive benefits and low risks, all of the Benedictions.
Prejudice: FRIEND
To find out what purposes ambiguous and erratically applied drug laws
serve we begin in Africa.
"This article explores the concept of quasilegality in relation to two
of Africas drug crops: khat and cannabis. It argues that the concept
is useful in understanding the two substances and their ambiguous
relation to the statute books: khat being of varied and ever-changing
legal status yet often treated with suspicion even where legal, while
cannabis is illegal everywhere in Africa yet often seems de facto
legal. The article argues that such quasilegality is socially
significant and productive, raising the value of such crops for
farmers and traders, but also allowing states to police or not police
these substances as their interests and instincts dictate. It also
argues that there is no clear link between the law on the statute book
and the actual harm potential of these substances. Finally, it
suggests that the concept has much wider use beyond these case-studies
of drugs in Africa in a world where global consensus on drug policy is
cracking, and where many other objects of trade and activities find
themselves in the blurred territory of the quasilegal."
and
"Quasilegality
"Quasilegal is a term with resonance in a number of fields, from the
study of law and the state to the study of drugs and other such goods.
The prefix quasi adds the idea of ambiguity to the term legal through
its meaning of as if, almost or seemingly. Quasilegal can refer to
procedures and rules within an organisation that are not supported
directly by state law, but resemble them in form, while also referring
to what might elsewhere be termed paralegal. Oren Perez links the
quasilegal to fuzzy law, soft law that lies between the poles of
lawlessness and complete legality. Such a definition is useful for our
purposes, linking the term as it does to spaces where state law is
often rivalled by semi-autonomous social fields in the words of Sally
Falk Moore, spaces that the substances we examine travel through while
often regulated by relationships of trust more than legal contract.
The term also hints at the vagueness of the law and its flexibility.
In this regard it links to debates in criminology regarding the
concept of discretion, where there is much leeway in the
interpretation and application of legal statutes. Again this leeway is
often influenced more by social relationships than by reference to the
law. The law is an imprecise tool, so in using discretion as to
whether to charge someone with an offence or whether to apply a more
or less lenient penalty, those who apply the law enter into an
ambiguous - quasilegal - realm. The law and its vagueness is also
capable of being corrupted by its protagonists, where discretion
becomes a tool for indiscretion and discrimination."
https://eprints.whiterose.ac.uk/121129/1/Quasilegality_author_accepted_version14_Augut_2017.pdf
[2150]
It is clear from this that the lesser rights are ascribed, to those to
whom the erratic laws have been applied, compared to the more
fortunate Homo sapiens who were left alone. This could be based on
economic, political, religious or racial groupings. Or language
groupings. It could be the person who complains about the Town Smell,
or has somewhere to live unencumbered by relatives or slack
bill-paying sharers. It could be people with red hair, or lights in
their windows. It could be people who don't give in to other types of
extortion or theft.
But what would we say about a society which thought it perfectly
acceptable to arrest, fine or imprison, or confiscate the property of
some people with an interest in vitamins, or insulin, or Scotch
whisky, while others were allowed to go freely about, openly producing
and consuming the same?
Would such a society and its legal edifices command the respect of its
population?
Racism: FRIEND
Black Americans are arrested for cannabis at four times the rate of
the whites. John Hudak, Deputy Director at the Center for Effective
Public Management and Senior Fellow in Governance Studies, has written
a book, reviewed on the website of the Brookings Institution, which
"traces its beginnings to 1916, when a group of leading reformers
founded the Institute for Government Research (IGR), the first private
organization devoted to analyzing public policy issues at the national
level." It was the first American "think tank".
Hudak's book
"explores the explicitly racist roots of cannabis policy in the United
States as well as the broader War on Drugs. It highlights how
politicians across the political divide spent much of the 20th century
using marijuana as a means of dividing America. By painting the drug
as a scourge from south of the border to a 'jazz drug' to the
corruptive intoxicant of choice for beatniks and hippies, marijuana as
a drug and the laws that sought to control it played on some of
Americas worst tendencies around race, ethnicity, civil disobedience,
and otherness."
https://www.brookings.edu/blog/how-we-rise/2020/06/23/marijuanas-racist-history-shows-the-need-for-comprehensive-drug-reform/
[1530]
A discussion can be found here:
https://www.brookings.edu/events/webinar-marijuana-a-substance-at-the-intersection-of-race-politics-and-culture/
[1531]
Legal amnesia: FRIEND
All your previous legal decisions, such as when weed was like heroin,
or when weed was no longer like heroin but still bad in unspecified
ways, or when weed was not a net benefit at the population level, are
disguised as a creeping technological advance, whereas the evidence
shows that it was really just ignorant bigotry from the get-go.
Any improvements in the law cannot be retrospective for the victims.
It is thought people would, if their previous convictions for sorcery
or heresy were reversed, might lose respect for the law. Nothing could
be further from the truth, as they would need lots of lawyers to fight
for their compensation.
Creeping improvements are no better. History will remember.
Bullying: FRIEND
Obese boys <15 were between 1.67 times more likely to be victims of
bullying. Obese boys BMI>30 and >=15 were 2.16 times more likely
to carry weapons.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2826832/
[1272]
Creativity: ENEMY
As reported by Gandy et al (2019) experiments on LSD and creativity
and meaning of life go back at least as far as 1966:
"A study on healthy people who had complained of a lack of purpose or
meaning in their lives found that a supervised LSD session resulted in
higher self-reported measures of self-actualization and creativity,
with participants reporting a greater sense of meaning and purpose in
their lives, oneness with humanity, decreased valuation of superficial
pursuits such as material gains and social status, and an increase in
confidence and assertiveness, with many of these changes still
apparent months later (Savage, Fadiman, & Mogar, 1966).
"Modern research has found that an LSD experience in a controlled
setting can result in elevated levels of optimism and trait openness 2
weeks post-experience (Carhart-Harris et al., 2016). The
administration of a single large (200 μg) dose of LSD in a
supportive setting to 16 healthy participants was found to lead to
increases in positive attitudes about life and/or self, positive mood
changes, altruistic/positive social effects, positive behavioral
changes, and well-being/life satisfaction at 1 and 12 months following
dosing, with no negative effects on attitudes or behavior attributed
to the LSD experience. After 12 months, 10 of 14 participants rated
their LSD experience as among the top 10 most meaningful experiences
of their lives, with five rating the experience as among the most
meaningful experiences of their lives (Schmid & Liechti,
2018)."
https://akjournals.com/view/journals/2054/3/3/article-p280.xml#B70
[6103]
"Participants [given 50 micrograms of LSD] were asked to come up with
alternative uses for items (such as a stone) or interpret drawings
(like waving lines).
"'When we looked at the responses, there was a distinct pattern to
those under the influence of LSD that was different from placebo,
which we have termed symbolic thinking. For example, when asked to
find creative uses for a knife, those who had gotten the placebo
answered that it could open a plastic bag or be used as a mirror,'
says Wiener. 'Those under the influence of LSD gave responses such as
cutting the important from the trivial in life. These responses moved
away from concrete, rational thinking towards more abstract or
symbolic thinking.'"
https://www.lucid.news/do-psychedelics-boost-creativity/
[1022]
Wiener et al (2022) found...
"In a randomized, double-blind, placebo-controlled, crossover study,
24 healthy volunteers received 50μg of LSD or inactive placebo.
Near drug peak, a creativity task battery was applied, including
pattern meaning task (PMT), alternate uses task (AUT), picture concept
task (PCT), creative metaphors task (MET) and figural creativity task
(FIG). Creativity was assessed by scoring creativity criteria
(novelty, utility, surprise), calculating divergent thinking (fluency,
originality, flexibility, elaboration) and convergent thinking,
computing semantic distances (semantic spread, semantic steps) and
searching for data-driven special features.
"Results: LSD, compared to placebo, changed several creativity
measurements pointing to three overall LSD-induced phenomena: (1)
pattern break, reflected by increased novelty, surprise, originality
and semantic distances; (2) decreased organization, reflected by
decreased utility, convergent thinking and, marginally, elaboration;
and (3) meaning, reflected by increased symbolic thinking and
ambiguity in the data-driven results.
"Conclusion: LSD changed creativity across modalities and measurement
approaches. Three phenomena of pattern break, disorganization and
meaning seemed to fundamentally influence creative cognition and
behaviour pointing to a shift of cognitive resources away from normal
and towards the new. LSD-induced symbolic thinking might provide a
tool to support treatment efficiency in psychedelic-assisted
therapy."
https://labs.psych.ucsb.edu/schooler/jonathan/sites/labs.psych.ucsb.edu.schooler.jonathan/files/pubs/wiessner_2022_lsd_creativity.pdf
[5572]
St Pierre et al (2025) confirm the worst fears of the
anti-creatives:
"Using multi-level modeling, we identified higher (p <.001)
ratings of Wellbeing (F(1,768) = 160.15), Productivity
(F(1,917) = 108.69), Creativity
(F(1,899) = 25.99), Connectedness
(F(1,859) = 253.4), Contemplation
(F(1,864) = 180.5), and Focus
(F(1,846) = 191.72) on microdosing days compared to
non-microdosing days. For the domain of Creativity, increased scores
were more pronounced among respondents with a history of using larger
doses of psychedelics (F(1,899) = 4.40,
p = .04)."
https://link.springer.com/article/10.1007/s00213-025-06913-9
[5613]
While Ptuj will be outraged at the finding of Prochazkova et al (2025)
that
"Microdosing psilocybin increased quality of original ideas."
https://www.sciencedirect.com/science/article/abs/pii/S002839082500440X
[5622]
"Ayahuasca-inspired DMT/harmine formulation alters creative thinking
dynamics during artistic creation" say Suay et al (2025):
https://journals.sagepub.com/doi/10.1177/02698811251353256
[5303]
Other papers relating to creativity are reviewed in [1022].
Some idea about the dangers awaiting those who are too afraid to try a
psychedelic can be discerned from "Leveraging psychedelic neuroscience
to boost human creativity using artificial intelligence" wherein Brian
M Ross of the Northern Ontario School of Medicine reveals the key
threats to Slovenia arising from their use:
"Psychedelics, such as LSD and psilocybin, disrupt entrenched
cognitive patterns by facilitating novel insights and new
associations."
"...reduced latent inhibition, increased divergent thinking, and
enhanced implicit learning..."
"...intensified meaning-making..."
"...enhancing communication between otherwise segregated brain
regions..."
"...Several studies suggest they facilitate novel associations by
relaxing cognitive constraints and encouraging a more fluid,
exploratory mindset. However, these effects are not uniform."
"...Although some artists use psychedelics regularly as a means of
enhancing creativity, this pattern of use typically does not become
problematic. Indeed, most classical psychedelics have low addictive
potential, even with repeated use, likely due to their intense and
often challenging psychological effects which naturally limit
excessive or compulsive use."
https://www.frontiersin.org/journals/artificial-intelligence/articles/10.3389/frai.2025.1589086/full
[5097]
Let's hope psychedelics fix up Slovenia's AI, such as Gastarbeiter -
for foreign workers in Slovenia - before it's too late:
"In 1966, researchers at the International Foundation for Advanced
Study in California gave mescaline to 27 men who were engineers,
physicists, mathematicians, architects, furniture designers, and
artists.
"While on the drug, one came up with a new conceptual model of a
photon particle; another envisioned a new approach to the design of a
vibratory microtome, a lab instrument that cuts material into small
slices; and an architect produced a design for a home that was later
approved by his client. The mescaline seemed to help 'facilitate
creative problem-solving, particularly in the "illumination phase",'
the researchers wrote."
But, as the Vice article discusses, revelations can vary in quality.
But that's true of people who don't take psychedelics too.


https://www.vice.com/en/article/5dgkkn/the-insights-psychedelics-give-you-arent-always-true
[1030]
Insulin sellers: FRIEND
"On January 23rd, 1923 Banting, Best, and Collip were awarded the
American patents for insulin. They sold the patent to the University
of Toronto for $1 each. Banting notably said: 'Insulin does not belong
to me, it belongs to the world.' His desire was for everyone who
needed access to it to have it.
"In order for the insulin to be mass produced and widely available,
the pharmaceutical company Eli Lilly and Co. were given the rights to
do so. While this incredible advancement was intended as a gift from
the discoverers, Eli Lilly and the two other major insulin producers,
Sanofi and Novo Nordisk, have turned insulin into profit machines,
assisting in bringing in billions of dollars in profit every year. By
1923, insulin was the highest-selling product in Eli Lillys history,
and profits from it accounted for over half of the companys revenue.
As we know, the prices have continued to skyrocket ever since."
https://www.t1international.com/100years/
[2359]
"Between 2012 and 2016, Lilly almost doubled the price of its insulin,
prompting letters from members of Congress about the sudden and huge
price increases."
https://skwawkbox.org/2024/10/17/the-trail-of-streetings-jabs4jobs-slimming-drug-company-is-littered-with-massive-lawsuits/
[3611]
The cost of insulin varies widely around the world. Rand has a report
and according to Figure 2.9 therein the price per standard unit in
2018 was $119.36 in the US, but only $8.19 on average in non-US OECD
countries.
Does it cost any more to make Americans' insulin? Is their
infrastructure so decrepit that distribution costs fourteen and a half
times more the other OECD countries? Profit over life is part of the
American dream.
https://www.rand.org/content/dam/rand/pubs/research_reports/RRA700/RRA788-1/RAND_RRA788-1.pdf
[954]
NECUD increases diabetes. Clark [707] mentions it 53 times. Besides insulin, the TZD PPAR agonist drugs
are also FRIENDS of prohibition.
Period pains FRIEND
Period pains and all the symptoms of the luteal phase which cannabis
shortens are friends of prohibition. So prohibition is FRIENDS with
mood swings, irritability, anxiety, fatigue, bloating, tender breasts,
headaches, breakouts or spots, changes in appetite, and changes in sex
drive, because it is friends with all the pharmaceutical treatments
for all of these.
https://www.clearblue.com/how-to-get-pregnant/luteal-phase
[960]
Prohibition is an American export, so here's a list of treatments from
the American dysmenorrhea pharmacopoeia.
https://www.drugs.com/condition/dysmenorrhea.html?page_all=1
[958]
Quite a few of these are based on ibuprofen, which is an
over-the-counter medication in the UK, but not Slovenia. And
"...if taken inappropriately and over long periods, ibuprofen can
cause gastro-intestinal, renal and cardiac complications, especially
among the 'at risk' patient groups."
https://onlinelibrary.wiley.com/doi/epdf/10.1111/1753-6405.12589
[959]
It also seems quite important to not do any serious research on using
cannabis for menstrual pain. Any research that is done is to examine
the problems of these cannabis abusers etc. etc. Accordingly RDTGH
authors Ferretti et al (2024) - insisting that feeling better must
have nothing to do with feeling good - claimed a first with their tiny
study, after finding only 33 subjects fitting the criteria:
"...who self-reported experiencing normal menstruation (occurring
every 2138 days and lasting between 4 and 8 days; Creinin et al.,
2004), willingness to track their menstrual cycles systematically, and
experiencing MRS."
The researchers had noticed that
"Some individuals attempt to alleviate menstrual-related symptoms
(MRS) by using cannabis and report having expectations that cannabis
can improve MRS; however, no study has examined the effect of
cannabinoids on MRS."
...and so women who had used cannabis in the last 30 days were
excluded.
In a two-dose analysis of the utility of CBD only, the authors used
the Menstrual-Related Symptom Questionnaire, the Brief Irritability
Test, the Depression, Anxiety, and Stress Scale21, Global impression
of change, and Subjective Severity.
2 4 mixed ANOVA analyses revealed lower MRSQ, stress, anxiety and
irritability scores, and a main effect of time for GIC and subjective
severity ratings of MRS, in all three months, but no effect on
depression.
"The present study findings are consistent with past research showing
the beneficial effects of CBD on various experiences associated with
MRS, including reductions in monthly ratings of MRS (using the MRSQ,
subjective severity, global impression of change), stress, and anxiety
(Zuardi et al., 2017). Data revealed reductions in both physiological
and psychological symptoms, which is consistent with past literature
documenting effects of CBD on both types of outcomes (Boyaji et al.,
2020; Shannon et al., 2019; Linares et al., 2019; Loflin et al.,
2017); however, various physiological symptoms that are assessed in
the MRSQ had not been examined in relation to CBD prior to the present
investigation (i.e., abdominal bloating, nausea, appetite-related
symptoms; Sexton et al., 2016; Slavin et al., 2017) and thus warrant
future research and replication.
"CBD has been associated with reducing pain related to inflammation
(Burstein, 2015). To the extent that some physiological MRS may be a
result of inflammation (Barcikowska et al., 2020; Gold et al., 2016),
CBD may reduce some pain-related physiological MRS; though this study
did not examine anti-inflammatory outcomes, future work may examine
the effects of CBD on biological markers of menstrual-related
inflammation."
https://psycnet.apa.org/fulltext/2024-61679-001.html
[3889]
The researchers do not seem to be in any great hurry under this
heading. Money is to be made curing symptoms - e.g. with NSAIDs -
while CBD is seen to prevent them. According to globenewswire.com on
26 March 2024:
"The PMS and menstrual health supplements market has grown strongly in
recent years. It will grow from $24.53 billion in 2023 to $26.23
billion in 2024 at a compound annual growth rate (CAGR) of 6.9%. The
growth observed in the historical period can be attributed to factors
such as the increasing awareness of women's health, changes in
lifestyles and dietary patterns, a growing recognition of PMS
symptoms, efforts in consumer education and health information
dissemination, and a shift in cultural attitudes towards women's
health.
"The market is expected to see strong growth in the next few years. It
will grow to $35.19 billion in 2028 at a compound annual growth rate
(CAGR) of 7.6%."
https://www.globenewswire.com/news-release/2024/03/26/2852663/28124/en/Global-PMS-and-Menstrual-Health-Supplements-Market-Analysis-2024-2028-2033-by-Product-Formulation-Consumer-Group-Sales-Channel-and-Region.html#:~:text=The%20PMS%20and%20menstrual%20health,(CAGR)%20of%206.9%25. [3890]
Covid- and pollution-induced anosmia and ageusia: FRIEND
On 12 Dec 2025 openpr.com predicted "Chronic Smell and Flavor Loss
Market Size to Reach USD 4.1 Billion by 2034"
"Pune, India, December 2025 - The global Chronic Smell and Flavor Loss
Market is projected to grow from USD 2.5 billion in 2024 to USD 4.1
billion by 2034, expanding at a CAGR of 5.2% during the forecast
period. Growing awareness of sensory disorders, improvements in
clinical diagnostics, and increasing research collaborations continue
to boost market expansion."
The worldwide fallout from Covid is the main driver:
"Chronic smell and flavor loss conditions-anosmia, hyposmia, ageusia,
and hypogeusia-are becoming increasingly recognized as significant
health burdens. The surge in sensory impairment cases following viral
infections (especially COVID-19), coupled with increasing elderly
populations and neurological disorders, is strengthening long-term
demand for diagnostic and therapeutic solutions."
https://www.openpr.com/news/4312514/chronic-smell-and-flavor-loss-market-size-to-reach-usd-4-1-billion
[5721]
Various pills and potions: FRIEND
Prescriptions for drugs used to treat pain, anxiety, high cholesterol,
nausea, psychoses, seizures, sleep disorders, depression, and
spasticity all fall with legalisation.
https://onlinelibrary.wiley.com/doi/epdf/10.1111/1753-6405.12589
[491]
Germany has a Cannabis Barometer:
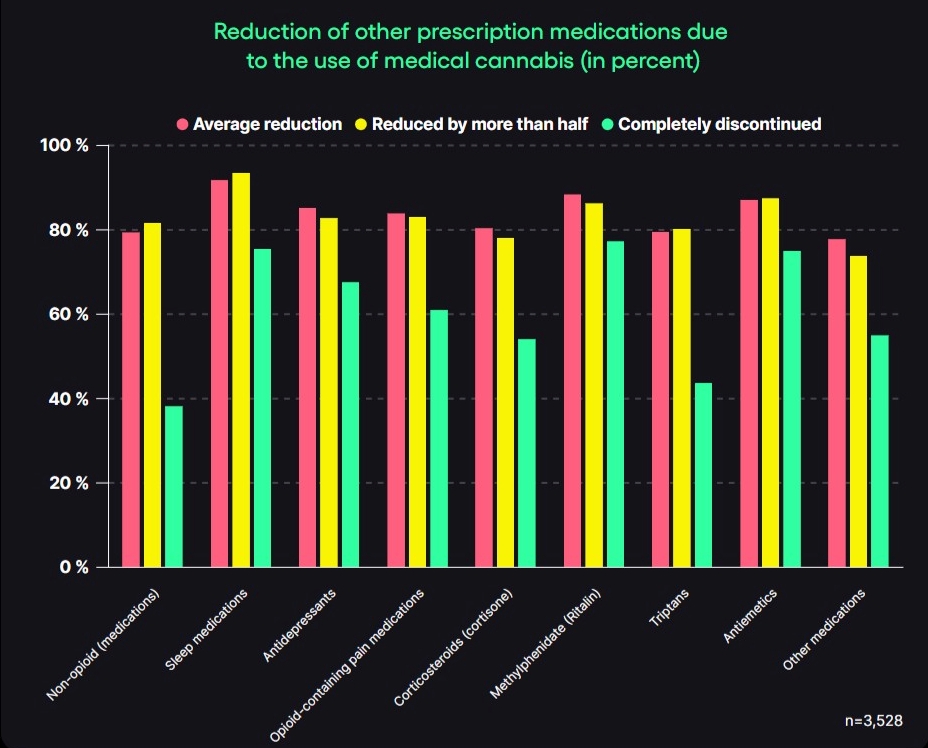
"Through the use of medical cannabis, patients were able to reduce the
use of other prescription medications by an average of 84.5% across
all categories. In more than half of the cases, medications could even
be stopped completely: the average rate of completely discontinued
prescription medications across the various categories is 58.9%. For
prescription sleeping pills, 93.6% were able to reduce the use by at
least half, and 75.5% were able to discontinue them completely.
Patients who took Methylphenidate (e.g., Ritalin) report an average
reduction of 88.4% through the use of medical cannabis. 77.3% were
able to discontinue it completely. Patients were able to reduce
opioids by an average of 83.9%. 61% of patients were able to
completely discontinue opioids through the use of medical
cannabis."
https://info.bloomwell.de/hubfs/Barometer/E%20The%20Cannabis%20Barometer%20Q1%202026.pdf
[6146]
Writing in the International Journal of Molecular Sciences, Thapa et
al (2023) point out the expanded notion of the endocannabinoidome:
"While ECS components including CB1 and CB2, and eCBs and their
enzymes have been shown to play a key role in the pharmacological
action of cannabis and cannabinoids, recent studies have revealed a
more complex picture involving other GPCRs and endocannabinoids-like
molecules. GPCRs are the most common human membrane receptor targeted
by currently available drugs. More than 34% of FDA-approved drugs
target GPCRs and account for annual international sales of over 180
billion USD."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10572150/pdf/ijms-24-14677.pdf
[4039]
In "The endocannabinoidomes: Pharmacological redundancy and
promiscuity, and multi-kingdom variety of sources and molecular
targets" Iannotti and Di Marzo (2025) spell out the growing scope of
the endocannabinoidome and by implication mechanisms in which the
Benedictions could exert their nutraceutical effects:
"This complex network now encompasses: (i) the 2 most established
eCBs, 2-AG and AEA; (ii) several dozens of eCB-like mediators,
including long-chain 2-MAGs, NAEs, N-acyl amino acids,
N-acyl-taurines, N-acyl-serotonins, N-acyl-dopamines, and primary
fatty acid amides; and (iii) redundant metabolic enzymes and molecular
targets for these molecules; and has been defined, due to its wide
biochemical diversity, as the 'endocannabinoidome' (Cristino et al,
2020) (Table 1).
"Concomitantly, it has been found that both eCBs and other eCB-like
molecules containing polyunsaturated fatty acids (PUFAs) in their
chemical structures, can be oxidized by the same enzymes that were
already known to transform such fatty acids, when in their free form,
into bioactive prostanoids, eicosanoids, and, more in general,
'oxylipins.' These enzymes include 12- and 15-lipoxygenases,
cyclooxygenase-2, and cytochrome p450-containing oxygenases and thus
engender a parallel 'oxyendocannabinoidome.' These oxidative
metabolites of eCBs and eCB-like mediators have receptors often, but
not necessarily, in common with those of the parent compounds (Simard
et al, 2022a) (Table 1)."
https://www.sciencedirect.com/science/article/abs/pii/S0031699725074782
[5108]
Morris et al (2025) believe CBD, but not THC, acts upon
anti-inflammatory lipid mediator synthesis via the LOX pathway - but
do not consider cannabinoid ratios, congeners, or entourage
effects:
"This present study aimed to investigate how CBD and THC effect plasma
levels of eicosanoids generated through LOX, COX, and cytochrome P450
(CYP450) pathways. Using plasma sample data from multiple clinical
studies, we tested the hypothesis that high-CBD cannabis use would
increase eicosanoid levels compared with high-THC cannabis. Results:
Following cannabis use, high-CBD cannabis led to a rise in plasma
eicosanoids, particularly lipoxins, while high-THC cannabis did not.
Conclusions: CBD promoted anti-inflammatory eicosanoid production via
the 15-LOX pathway, therefore supporting the potential role of CBD as
a therapeutic candidate for inflammatory diseases."
https://pubmed.ncbi.nlm.nih.gov/40552985/
[5112]
The problem is, cannabis just doesn't cause enough side-effects -
iatrogenic illnesses which, according to the western money model,
require more drugs.
Reporting in the journal Health Economics in April 2022, Raman and
Bradford examine the impact of recreational legalization in 10 states
plus Washington, D.C.:
"We find significant reductions in the volume of prescriptions within
the drug classes that align with the medical indications for pain,
depression, anxiety, sleep, psychosis, and seizures. Our results
suggest substitution away from prescription drugs and potential cost
savings for state Medicaid programs."
"Our findings show significant reductions in the Medicaid prescribing
rate relative to implementation of an RCL in six of our nine
condition-specific drug classes. We find that RCLs are associated with
the following condition-specific drug utilization reductions: 11.1%
(95% Confidence Interval [CI] = −18.2 to −4.1) for
depression, 12.2% (95% CI = −19.5 to −4.8) for anxiety, 8%
(95% CI = −15.4 to −0.6) for pain, 9.5% (95% CI =
−16.6 to −2.5) for seizures, 10.7% (95% CI = −17.8
to −3.6) for psychosis, and 10.8% (95% CI = −16.1 to
−5.4) for sleep. We do not see a measurable change in drugs used
to treat nausea, spasticity, or glaucoma following RCLs, in the
Medicaid population."
https://onlinelibrary.wiley.com/doi/10.1002/hec.4519
[1203]
"'Marijuana, in its natural form, is one of the safest therapeutically
active substances known to man.' DEA Administrative Law Judge Francis
Young Docket No. 86-22. 1988."
https://www.medicalcannabis.com/wp-content/uploads/young.pdf
[2159]
"Cholesterol Is A Nutrient, Not A Disease," says Dr Jocelyn Foran,
MD:
"Without Abundant Cholesterol Our Bodies Cannot Make:
Testosterone
Aldosterone
Cortisol
DHT Dihydrotestosterone
DHEA Dehydroepiandrosterone
Estradiol
Estriol
Estrone
Progesterone
Vitamin D
"The Most Important Fat In Our Body Is Cholesterol:
Protects against chemicals, toxins & heavy metals.
Prevents dementia & cognitive decline.
Protects against all cause mortality.
Production of all steroid hormones.
Bone density & Osteoporosis prevention.
Protective against stroke & heart disease.
Important for lungs & airways.
Building block of all cells & mitochondria.
Absorption of Vitamins A, D, E & K.
Critical for digestion & bile acids.
Immune system protection against infections.
Protection against bacteria, pathogens & viruses.
Lowers risk of cancer & death.
Lowers risk of depression & suicide.
Lowers stress, cortisol & anxiety.
Optimal brain is 60% fat & 25% cholesterol."
https://x.com/ValerieAnne1970/status/1929081019225014360
[5040]
The statin market is predicated on the dogma that cholesterol is bad.
By 2018 Pfizer's Lipitor beccame the most profitable drug in the
history of medicine. Statins in condiments at burger outlets, and in
the water supply, have been proposed. Skeptics like Dr Maryanne Demasi
say statins serve no purpose in lowering cholesterol. By simply
lowering the threshold of what we call high cholesterol, the "need"
for statins was increased in the customer base.
"Skepticism arose when it was discovered that 8 out of 9 of those
people deciding to lower that threshold actually had direct direct
financial ties to statin manufacturers."
"In 2013, American College of Cardiologists and the AHA moved away
from a single cholesterol number."
Her Youtube discusses the role of calculators in assessing CV risk.
Instead of a single number, they started including cholesterol, age,
blood pressure, weight, diabetes etc.
Different standards evolved for prescribing in the US vs the UK. In
the US a 7.5% risk of developing CV disease in the next ten years
triggers a statin recommendation. In the UK it is 20%.
"By simply changing from a single cholesterol number to this very low
percentage risk profile, it increased the number of Americans being
prescribed statins by 12.8 million."
"4 out of 5 'calculators' were over-estimating the risk, up to
115%."
This is referred to as the 'statinisation' of the population.
Yet the actual data on their alleged effectiveness is a secret
property of a tiny group.
https://youtu.be/BzTjPuikhQE
[3027]
Prior to 2013 statins were thought to be blockbuster. In 2019 the
question of statins was brought to the attention of 32 European
national regulators. Jefferson, Demasi and Doshi simply asked what you
might think was common knowledge already, namely:
"1. Are any of the seven statins authorised in [Country X]? (yes/no
for each statin)
"2. If yes, what year was each statin authorised?
"3. Was each statin first authorised on the basis of [Country X]'s
assessment of a marketing authorisation application (MAA)? (yes/no)
"4. If Q3 = yes. Does Country X still hold the clinical trial evidence
(including clinical study reports) in its archives? (yes/no)
"5. If Q3 = no. Which country evaluated the MAA and granted a license
that was recognized by [Country X] (for example, on the basis of the
mutual recognition or decentralised or national authorisation
procedures)?
"6. If [Country X] authorised the statin please refer us (via a
weblink or URL) to the healthcare professional prescribing information
for each statin, in English if possible."
https://www.bmj.com/content/354/bmj.i4992/rr-14
[3033]
Cholesterophobia is a relatively recent preoccupation, postdating the
SCND, while at the time of the Opium Conference essential fatty acids
and messenger lipids were unknown.
"[Ernst] Wynder in the 1970s became concerned with professional views
of what was the 'normal' blood cholesterol level. Most clinical
laboratory forms of the time used the cut-point of 300 mg/dl to flag
abnormal. Below that level, attention was rarely called to
cholesterol. Wynder decided to gather representatives of each major
medical discipline and charge them with defining 'optimal' blood
cholesterol levels, insisting on their independent deliberations. He
enlisted Barry Lewis of London to summarize clinical data, Bob
Wissler, the pathological data, and Henry Blackburn, the
epidemiological data. Each group of experts arrived at Wynders elegant
quarters at the Ford Foundation in Manhattan in the Fall of 1979 and
deliberated separately, presenting their conclusions in a final
plenary session.
"It turned out that experts from each discipline had arrived at
virtually identical conclusions on what were ideal levels of blood
total cholesterol for a population, and what levels they thought were
feasible to achieve in Western industrialized populations. At the
time, data on lipoprotein subfractions from representative populations
were not available. The ideal mean value of 160 mg/dl was illustrated
in a curtotic distribution with few population values above 200. It
was thought feasible in a decade or so to arrive at a mean of 190,
with a standard deviation of +/-30, compared to the existing mean of
210 with a standard deviation of 35. Wynder went on to develop similar
recommendations for ideal blood lipid values for youth.
"Following the success of the LRC Primary Prevention Trial in 1984, a
consensus conference of the NHLBI formalized recommendations for a
National Cholesterol Education Project (NCEN) in the medical and
public health community, where 200 mg/dl was the upper limit of
'normal' for the individual and 130 as the upper limit for LDL. The
NCEN have since modified these recommended values as a result of
extensive subsequent trial data indicating the lower LDL and the
higher HDL the better."
http://www.epi.umn.edu/cvdepi/essay/optimal-blood-lipid-levels-an-international-report/#:~:text=Wynder%20in%20the%201970s%20became,was%20rarely%20called%20to%20cholesterol. [3028]
"Total cholesterol and all-cause mortality by sex and age: a
prospective cohort study among 12.8 million adults" by Yi et al (2018)
found the lowest mortality in the 210-250 TC range:
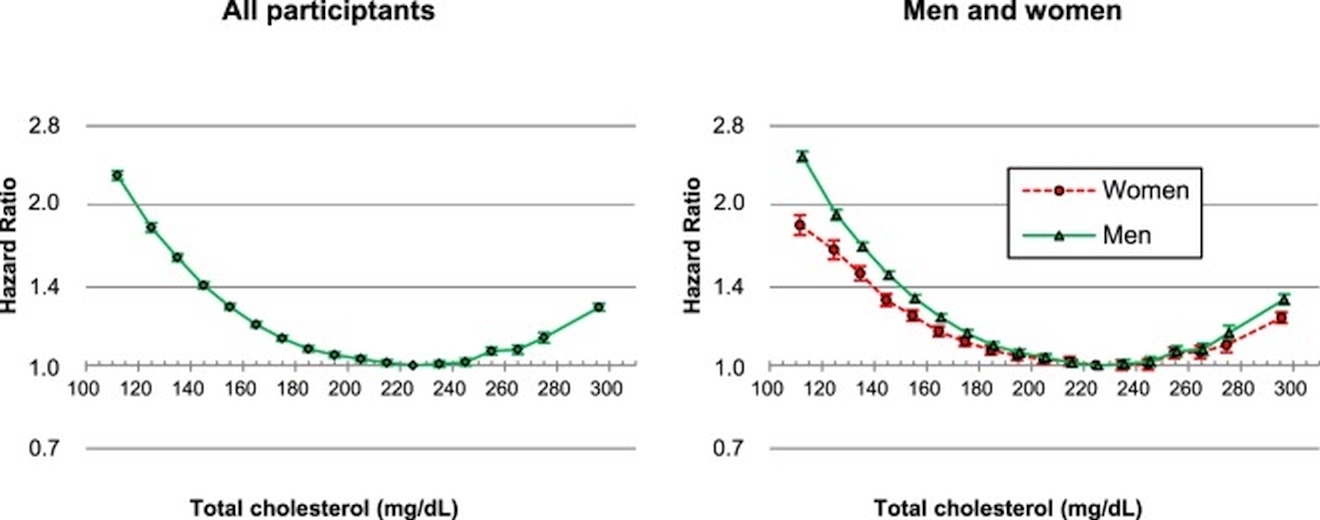
https://www.nature.com/articles/s41598-018-38461-y.pdf
[3806]
"In the UK, two medical experts have earned a major win in the High
Court in a case described by the Judge as 'the most significant piece
of defamation litigation' he has seen in a very long time.
"The case shines a light on how journalists cover scientific issues
and how the media seeks to discredit those who challenge official
narratives.
"For decades, Malcolm Kendrick, general practitioner and Zoe Harcombe,
PhD in nutritional science, have publicly challenged the role of
saturated fat and cholesterol in heart disease, as well as the
widespread use of statin medications."
The experts accused the Daily Mail of bias, and a hatchet job.
"Justice Matthew Nicklin issued a 255-page judgement and dismissed a
'public interest defence' because the articles in question had
'seriously misled readers.'"
and
"The Professors included Rory Collins, Peter Sever, and Colin Baigent
who co-authored a 2016 review in The Lancet which promoted the wider
use of statins, even for people at low risk of heart disease a view
that Kendrick and Harcombe had publicly challenged.
"Their advocacy of statins to lower cholesterol is well-known.
"Collins told Calman that anyone who thinks LDL-cholesterol does not
'cause' heart disease is akin to 'flat earthism' and 'in the same
realm as claiming that smoking does not cause lung cancer.'"
So...
"Calman put out a call for people to come forward and tell their
stories, but he was apparently 'inundated by stories of people who
have stopped taking statins and felt far healthier.'
"He also received 'two quite dramatic stories' of patients who were
taken off their statins by their doctors after they developed serious
liver problems and died from complications. 'The families themselves
both naturally question whether statins caused the problems,' noted
Calman.
"All these case studies contradicted the narrative that stopping
statins was dangerous, so Calman wrote to the Professors. 'What we
havent had is a single story which backs your thesis, and obviously Im
concerned,' he explained. 'I think it makes us look rather weak.'"
https://brokenscience.org/doctors-sue-british-tabloid-for-libel-and-win-first-battle-round/
[3409]
Other evidence links statin use to reduced impairment of coenzyme Q10
production, mitochondrial dysfunction, disruption of intracellular
calcium metabolism, muscle fibre damage,
declines in muscle function, grip strength, appendicular lean mass
(ALM),
and increased insulin resistance.
https://onlinelibrary.wiley.com/doi/pdfdirect/10.1002/jcsm.70132
[5720]
Supporting the idea that the LDL-C hypothesis is broken, while
"acceptable" levels have been lowered to trigger statin prescribing,
Ravnskov et al (2020) in a systematic review of cohort studies report
as follows:
"We identified 19 follow-up studies including 20 cohorts of more than
six million patients or healthy people. Total mortality was recorded
in 18 of the cohorts. In eight of them, those with the highest LDL-C
lived as long as those with normal LDL-C; in nine of them, they lived
longer, whether they were on statin treatment or not. CVD mortality
was measured in nine cohorts. In two of them, it was inversely
associated with LDL-C; in five of them, it was not with normal BMI
associated. In the study without information about total mortality,
CVD mortality was not associated with LDL-C. In two cohorts, low LDL-C
was significantly associated with total mortality. In two other
cohorts, the association between LDL-C and total mortality was
U-shaped. However, in the largest of them (n>5 million people below
the age of 40), the mortality difference between those with the
highest LDL-C and those with normal LDL-C was only 0.04%.
"Conclusions: Our updated review of studies published since 2016
confirms that, overall, high levels of LDL-C are not associated with
reduced lifespan. These findings are inconsistent with the consensus
that high lifetime LDL levels promotes premature mortality. The
widespread promotion of LDL-C reduction is not only unjustified, it
may even worsen the health of the elderly because LDL-C contributes to
immune functioning, including the elimination of harmful pathogens.
https://meddocsonline.org/annals-of-epidemiology-and-public-health/the-LDL-paradox-higher-LDL-cholesterol-is-associated-with-greater-longevity.pdf
[3805]
While some have suggested cannabis can increase LDL-C to HDL-C ratios,
the studies on cholesterol have been very small and do not prove
anything either way. For instance Cusihuaman et al managed to find 20
heavy cannabis users in Cusco, Peru (2022). Although HDL-C was raised
after smoking, the irony of the condition of the original cohort seems
to have been lost on the authors, who report matter-of-factly that
before the experiment began, out of these twenty heavy users with
normal BMI
"...12 (60%), 10 (50%), and 11 (55%) had desirable total cholesterol,
fairly good HDL-C (4060 mg/dL) and fairly good LDL-C (100129 mg/dL)
values, respectively."
...while how many candidates for this research were rejected because
they were too fat is not recorded.
https://www.mdpi.com/2227-9717/10/8/1597
[3029]
A true understanding of the risks vs. benefits at the biochemical
level is bedevilled by the significant number of variables, including
all the cannabinoids and terpenes, genetic predispositions, diet and
other environmental factors, as well as prohibition itself (the
cannabis cohort may be in hiding). The epidemiology, as the evidence
shows, tells a different story.
https://www.healthline.com/health/can-weed-raise-your-cholesterol
[3030]
For instance, in a comparison of cannabis use with the odds ratio of
hypertriglyceridemic waist (HTGW+/+) phenotype in U.S. adults:
"Of the 47,364 adults included, 48.5% were women. The prevalence of
HTGW+/+ phenotype was 11.7%. Current, but not former, users were less
likely to show HTGW+/+ phenotype. Current cannabis users with greater
or equal to four uses per week showed a significant lower likelihood
for HTGW+/+ than those who never used cannabis (AOR 0.46 [95% CI,
0.220.97]). HTGW+/+ phenotype was associated with neither two to three
uses per week (AOR 1.12 [95% CI, 0.403.12]) nor less than two uses per
week (AOR 0.56 [95% CI, 0.181.73])."
The analysis shows that ex-users (<2 uses per week in the past)
suffering from NECUD/SPUK for 1-10 years fared the worst, with a 60%
higher chance of HTGW. They were followed by ex-users (>=4 uses per
week in in the past) with 28% higher, compared to never-users.
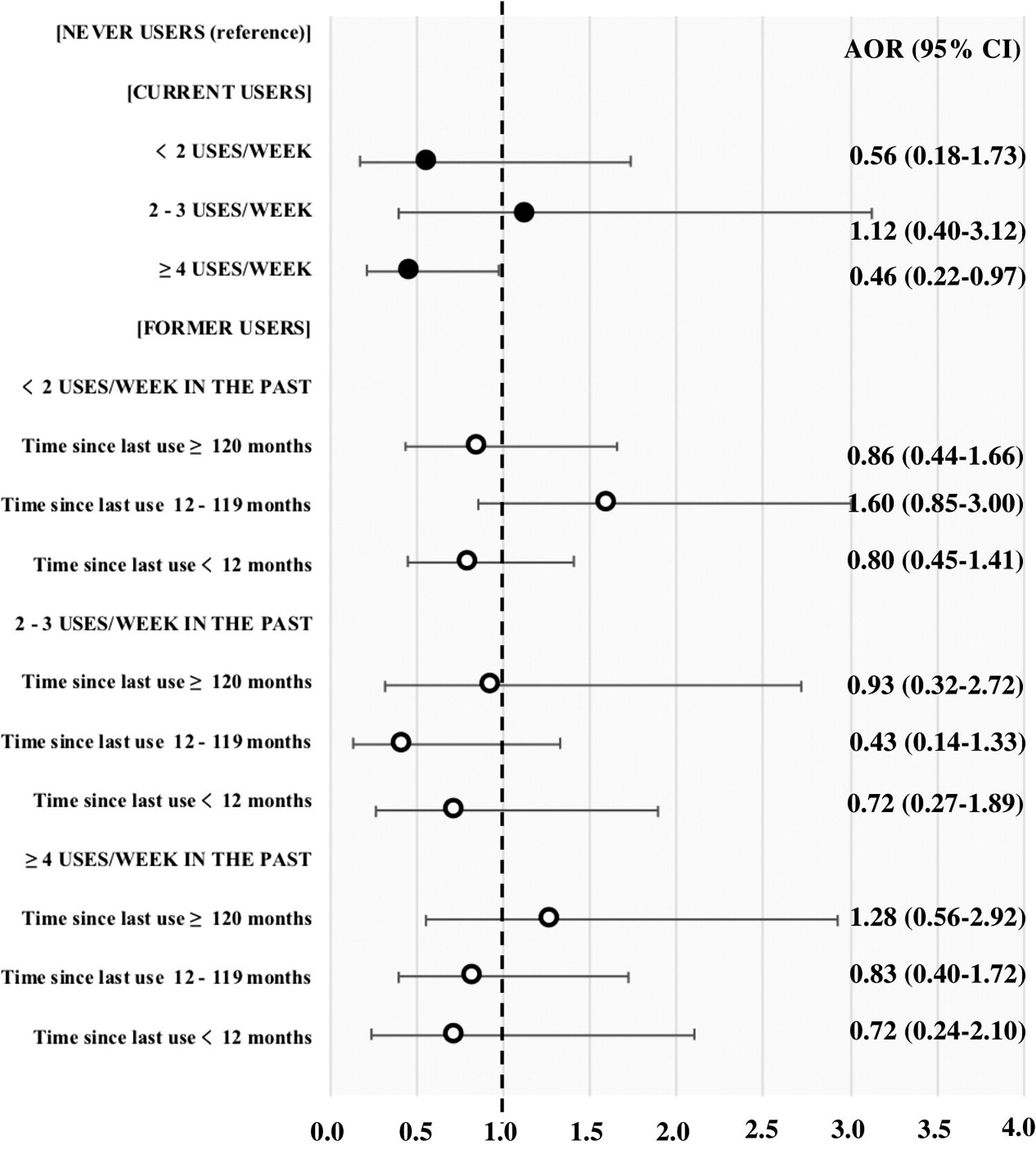
https://www.liebertpub.com/doi/10.1089/can.2019.0048
[3031]
And here's an illustration from the Lancet's 2019 position statement
on visceral and ectopic fat, atherosclerosis, and cardiometabolic
disease, outlining the outcomes.
https://www.thelancet.com/journals/landia/article/PIIS2213-8587%2819%2930084-1/fulltext
[3032]
Indeed the most interesting thing about more reliable large-scale
studies of cannabis and cholesterol is the lack of them.
In a two-way fixed-effects regressions and leverage variation from
eleven U.S. states that adopted a recreational cannabis law (RCL)
between 2010 and 2019, Raman et al found a 26% reduction in
pharmacy-based distribution of codeine and as much as a 37% reduction
after recreational cannabis laws have been in effect for four
years.
https://onlinelibrary.wiley.com/doi/10.1002/hec.4652
[2686]
Cannabis and classical psychedelics are a direct rival of atypical
antipsychotics. If you want to know when elongating your dendritic
spines is dangerous, that's when cannabis and psychedelics are
responsible. The advantage of atypical antipsychotics such as
clozapine over conventional antipsychotics such as haloperiodol is:
"...that in rat dissociated hippocampal neurons 1.0 μM clozapine
administration increased DS-enriched protein spinophilin by 70%,
increased post-synaptic protein shank1a puncta density by 26% and
increased overall primary dendrite DS density by 59%. Filopodia and
mushroom DS were particularly affected by clozapine. Conversely, 0.1
μM haloperidol decreased spinophilin protein by 40%, caused a 25%
decrease in shank1a puncta and reduced the numbers of filopodia. In
contrast, neither haloperidol nor clozapine induced any change in the
levels of the pre-synaptic protein synapsin. This indicates that
clozapine and haloperidol differentially regulate DS and post-synaptic
plasticity. These findings may provide a molecular and cellular
correlate to the superior therapeutic profile of clozapine when
compared with haloperidol."
https://www.sciencedirect.com/science/article/abs/pii/S1044743106001047?via%3Dihub
[2969]
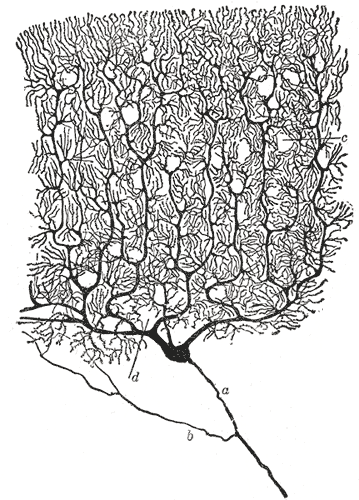
https://en.wikipedia.org/wiki/Golgi%27s_method
[2975]
Please note that the public's dendritic spines belonged to them even
before their description and naming in 1888 by Santiago Ramn y Cajal.
Much of his insight into their purpose and function proved to be
correct, while opponents who argued spines were an artifact of the
Golgi staining process were eventually proved wrong, but not until
after his death in 1934 and the application of electron microscopy.
"De Robertis and Palay performed the first ultrastructural analysis of
synapses (DeRobertis and Bennett, 1955; Palay, 1956) and shortly
afterwards, synapses were demonstrated on spines (Gray, 1959a,b).
Cajal was proven correct and spines became a bona-fide topic of
interest for neurobiological studies."
https://www.frontiersin.org/articles/10.3389/fnana.2015.00018/full
[2968]
So in respect of our treatment of our dendritic spines and its
relevance to this hearing, if some evidence in support of the legal
status quo claims there is no need for these drugs to promote DS
growth, or that spine growing is dangerous, remember how great the
atypical antipsychotics are supposed to be, and why.
Remember that dendritic spine length is considered a valuable measure
of the utility of both legal and illegal drugs.
Can the same effect be useful for legal drugs and not useful for the
illegal ones? That doesn't make sense. No law can change the utility
of elongated DS which, let us remind ourselves constantly, belong to
their owners and not to Pfizer or Krka; nor to Gibanje Svoboda or the
SDS; not to the judiciary, nor to the Archbishop of Ljubljana; finally
our dendritic spines do not belong to the Republic of Slovenia, its
Courts, or to the staff of UNODC.
Suffice to say, they were not a topic of concern at the 1925 Opium
Convention, as Cajal's work was still in the wilderness, and much
still remains to be elucidated even today. Had the relevant
discoveries about recreational drugs and dendritic spines predated the
anti-drug treaties, if would have been rather hard to argue for
prohibition.
The devastating effects of cannabis upon rival drugs may be
extrapolated from the results of a 2023 survey of over 200 prescribees
in New Zealand:
"Of the participants who took cannabis for other reasons, such as
autism, attention deficit hyperactivity disorder, post-traumatic
stress disorder and difficulty eating, 98% found taking cannabis
helped.
"Study co-author Dr Geoff Noller, of the Dunedin School of Medicines
Centre for Bioethics, says as with several other studies undertaken in
Aotearoa New Zealand, there was consistent reporting of positive
effects on pain relief, sleeplessness and anxiety.
"'An important finding of the study was that participants either
decreased or stopped their use of prescribed medicines, many of which
were opioid based,' Dr Noller said in a press release."
What proportion of the population experiences anxiety? This Defence
says 100%.
https://cannabishealthnews.co.uk/2023/06/05/new-zealand-new-findings-prompt-calls-for-wider-access-to-medicinal-cannabis/
[2685]
The stress agenda: FRIEND
Psychedelics enthusiasts have long managed without technical
explanations of the biological mechanisms of fear. Fear of breaking a
law lacking rational explanation is no different to any other kind of
fear.
But since the user is expected, unlike the prohibitionists, to provide
a rationale for their actions, the Defence is obliged to Chung et al
(2025) who explain "Psychedelic control of neuroimmune interactions
governing fear":
"Neuroimmune interactionssignals transmitted between immune and brain
cellsregulate many aspects of tissue physiology1, including responses
to psychological stress, which can predispose individuals to develop
neuropsychiatric diseases. Still, the interactions between
haematopoietic and brain-resident cells that influence complex
behaviours are poorly understood. Here, we use a combination of
genomic and behavioural screens to show that astrocytes in the
amygdala limit stress-induced fear behaviour through epidermal growth
factor receptor (EGFR). Mechanistically, EGFR expression in amygdala
astrocytes inhibits a stress-induced, pro-inflammatory
signal-transduction cascade that facilitates neuronglial crosstalk and
stress-induced fear behaviour through the orphan nuclear receptor
NR2F2 in amygdala neurons. In turn, decreased EGFR signalling and fear
behaviour are associated with the recruitment of meningeal monocytes
during chronic stress. This set of neuroimmune interactions is
therapeutically targetable through the administration of psychedelic
compounds, which reversed the accumulation of monocytes in the brain
meninges along with fear behaviour. Together with validation in
clinical samples, these data suggest that psychedelics can be used to
target neuroimmune interactions relevant to neuropsychiatric disorders
and potentially other inflammatory diseases."
https://www.nature.com/articles/s41586-025-08880-9
[5120]
Chung et al "specifically included that astrocytes are direct targets
of corticosterone signaling for chronic stress, linking these
inflammatory signals with fear behaviour through glucocorticoid
receptor activation and epidermal growth factor receptor upregulation.
This specific receptor expression in the amygdala inhibits
stress-induced, pro-inflammatory signal transduction cascades, while
enabling neuronal-glial crosstalk. These findings support the
mechanism of psilocybin for the use of neuroimmune modulation and
support for neuropsychiatric disorders." [5119]
The Defendant's infographics explain where this psychiatric paradigm
fits in with typical naturalistic use.
Accordingly this mechanism is included among the Benedictions.
Psychedelics are fundamentally inimical to governments' attempts to
reduce political inclusivity and public participation, using the fear
cycle.
By reducing fear extinction, THC, LSD, DMT, DOI, TCB-2, 𝑅-MDMA, and
4-OH-DiPT ameliorate the effects of today's stress agenda. Those who
profit from the stress agenda - basically by piling it on - have
nothing to gain from people with a cool, calm and collected view of
problems and solution-oriented behaviour.
Alcohol: FRIEND
"A recent study [3144] found that more Americans now consume cannabis every day than drink
alcohol on a daily basis. Since 1992, it found, the per capita rate of
daily cannabis consumption in the country has increased nearly 15
times over.
"A multinational investment bank said in a report late last year that
marijuana has become a 'formidable competitor' to alcohol, projecting
that nearly 20 million more people will regularly consume cannabis
over the next five years as booze loses a couple million drinkers. It
also says marijuana sales are estimated to reach $37 billion in 2027
in the U.S. as more state markets come online."
https://www.marijuanamoment.net/peoples-use-of-alcohol-or-opioids-causes-greater-secondhand-harms-than-marijuana-consumption-does-study-finds/
[3145]
According to Casswell et al (2016) in "How the alcohol industry relies
on harmful use of alcohol and works to protect its profits":
"The alcohol industry have attempted to position themselves as
collaborators in alcohol policy making....The goal of their public
relations organisations is to promote responsible drinking. However,
analysis of data collected in the International Alcohol Control study
and used to estimate how much heavier drinking occasions contribute to
the alcohol market in five different countries shows the alcohol
industry's reliance on the harmful use of alcohol. In higher income
countries heavier drinking occasions make up approximately 50% of
sales and in middle income countries it is closer to two-thirds. It is
this reliance on the harmful use of alcohol which underpins the
conflicting interests between the transnational alcohol corporations
and public health and which militates against their involvement in the
alcohol policy arena. [Caswell S, Callinan S, Chaiyasong S, Cuong PV,
Kazantseva E, Bayandorj T, Huckle T, Parker K, Railton R, Wall M. How
the alcohol industry relies on harmful use of alcohol and works to
protect its profits. Drug Alcohol Rev 2016;35:661664]"
https://onlinelibrary.wiley.com/doi/abs/10.1111/dar.12460
[3960]
Taxation politicking: FRIEND. Governments sometimes try to equate high
taxation with an attempt to control unhealthy behaviour. Sin taxes do
not prevent or proportionately ameliorate out-of-control substance
use.
"In 1993 Leung and Phelps performed a literature review of 15 studies
that analyzed either statewide or nationwide data on alcohol
consumption but used differing methods and criteria for subject
selection and data analysis. Summarizing the broad range of reported
results, the reviewers estimated that a 1-percent increase in price
led to a 0.3-percent decrease in demand for beer, a 1-percent decrease
in demand for wine, and a 1.5-percent decrease in demand for
spirits.
"More recent research has continued to study the effects of price
changes on alcohol consumption. In one study, based on a random
nationwide survey of 18,000 adults, Manning and colleagues found that
higher beverage prices were significantly related to lower alcohol
consumption rates among the overall population. However, no
significant responsiveness to price was found among the heaviest
drinkers, specifically the 5 percent of the population responsible for
36 percent of the Nation's total alcohol consumption."
Abe Lincoln's quote.
A Forbes' article refers to the National Institute on Alcohol Abuse
and Alcoholism:
https://pubs.niaaa.nih.gov/publications/aa51.htm
[950]
on this topic, which in turn refers to
https://www.jstor.org/stable/20111841
[948]
https://linkinghub.elsevier.com/retrieve/pii/0167629694000423
[949]
And according to Forbes:
"Such claims are politically useful because the average adult who
consumes alcohol may be reluctant to voluntarily impose alcohol taxes
on themselves if they realized who really bore the costs.
"In order to substantiate the claim that abusive drinkers pay most of
the costs, proponents rely on an unrealistic definition of an abusive
drinker."
https://www.forbes.com/sites/econostats/2016/10/25/taxing-choice-and-the-road-to-prohibition/?sh=5b7121f27285
[947]
The woo woo of good vs bad euphoria: FRIEND
Big Pharma and Big Alcohol are compelled to look both ways. Euphoria
from cannabinoids and psychedelics is viewed in a therapeutic context
is as "bad euphoria", because it will limit sales of drugs through
channels where messages against those are reinforced to sell other
drugs. At the same time, alcohol creates so much health devastation it
is profitable for the drugs companies. Some effort has even been put
into promoting alcohol as a health benefit, but this does not hold up
in the largest studies. The friends of prohibition are motivated to
despise "bad euphoria" but not criticise the "good euphoria" that is
causing much of the liver disease and cancer in the first place.
As in all religions in which not all persons necessarily believe, the
"bad euphoria" thesis can be theologized, reified, and schismatized,
for the benefit of a generation too old and fixed in its ways to
change. One of the subcategories of bad euphoria in bad textbooks is
"overly elated mood".
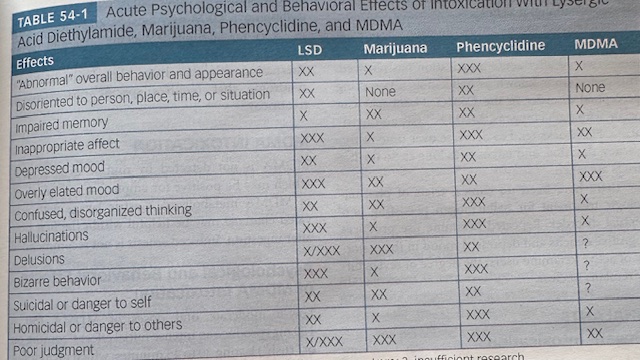
https://x.com/Peter_Grinspoon/status/1867593872831873392
[3783]
Psychiatrists on the pharma payroll: FRIEND
"Over half of active psychiatrists (55.7%) received some form of
payments from pharmaceutical manufacturers. Of these, top the 2.8% of
psychiatrists received 82.6% of the payments. Pharmaceutical
manufacturers provided 812,877 payments worth $110,512,607.18 to
26,422 psychiatrists in the US. Compensation for services (e.g.,
speakers bureaus) and consulting fees altogether constituted 71.4% of
the total payment, with a median value of $1,725.00 and $700,
respectively. Among all psychiatrists who received payments,
manufacturers that paid the most included Otsuka Pharmaceuticals,
Alkermes, and Sunovion Pharmaceuticals."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7260092/
[4500]
The gravitational pull of anti-euphoria is strong. Even when the
benefits of just a single puff per day must be admitted, science must
strive to make sure we don't enjoy cannabis. Thus, Psychology Today is
able to tell us that:
"Ordinarily, we do not view marijuana as being good for our brain and
certainly not for making memories. How could a drug that clearly
impairs memory while people are under its sway protect their brains
from the consequences of aging? The answer likely has everything to do
with the way that young and old brains function and a series of
age-related changes in brain chemistry. When we are young, stimulating
the brains marijuana receptors interferes with making memories.
However, later in life, the brain gradually displays increasing
evidence of inflammation and a dramatic decline in the production of
new neurons, called neurogenesis, that are important for making new
memories (Duncan et al., 2024).
"Research has demonstrated that stimulating the brains marijuana
receptors may offer protection by reducing brain inflammation and by
restoring neurogenesis. Thus, later in life, marijuana might actually
help your brain, rather than harm it. Cannabis products may offer
benefits for a variety of central nervous system diseases and
dysfunctions such as forms of epilepsy, multiple sclerosis,
Parkinson's disease, and some neuropsychiatric disorders. It may
require very little daily cannabis consumption to produce benefits in
the older brain; it appears as though only a single puff each day is
necessary to produce significant benefit."
Gary Wenk Ph. D concludes with the inexplicable statement that:
"The challenge for pharmacologists in the future will be to isolate
the beneficial effects of the marijuana plant from its psychoactive
effects."
https://www.psychologytoday.com/us/blog/your-brain-on-food/202404/preventing-memory-loss-with-marijuana
[4612]
Or as he might have said, "The challenge for pharmacologists in the
future will be to create a patentable product, make sure it's no fun,
doesn't work, and creates a need for more patentable drugs."
The global schizophrenia drugs market will be worth $8.02 Billion in
2021, reported Yahoo Finance in April 2022, and is expected to reach
$10.15 Billion in 2027.
How do they know?
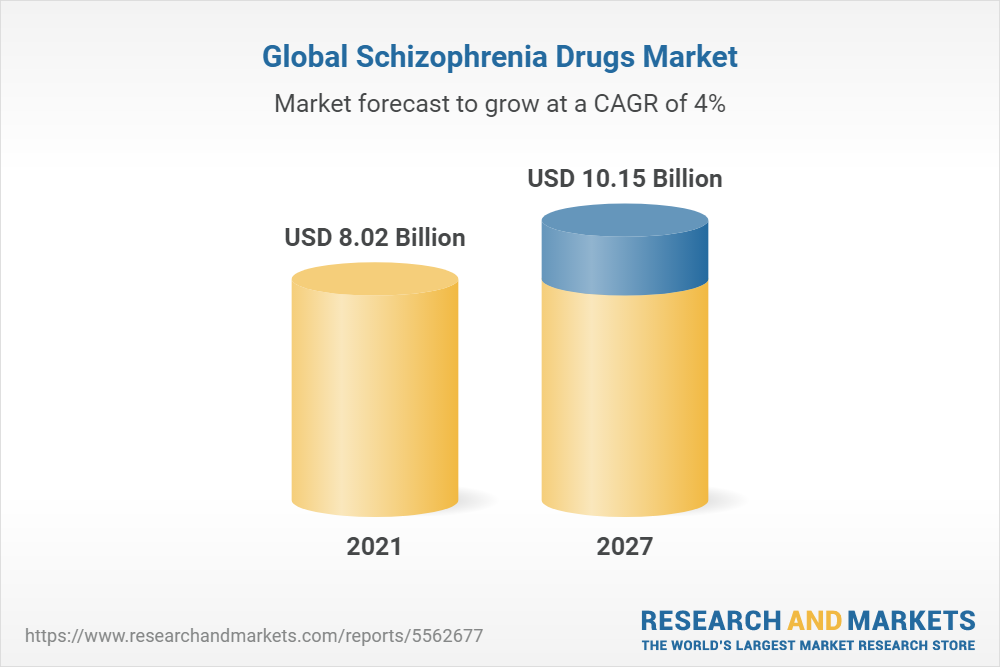
https://finance.yahoo.com/news/global-schizophrenia-drugs-market-research-080300440.html?guccounter=1
[2528]
Doctors on the the pharma payroll: FRIEND
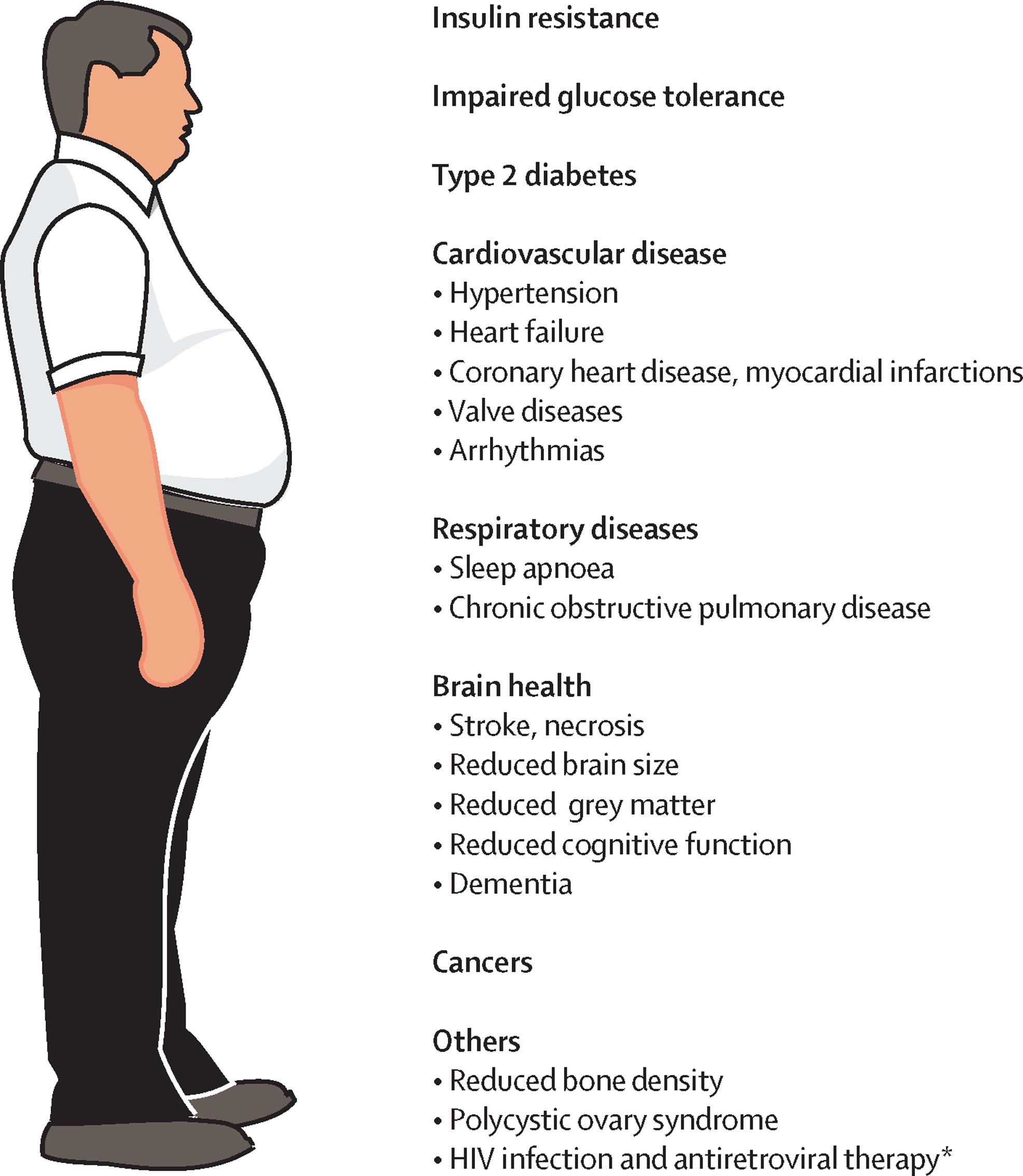
Obesity is a reliable source of income for pharmaceuticals. Besides
the downstream negative health effects of obesity, obesity per se is a
target of drugs which companies are keen to keep prescribing doctors
and pharmacists up to date about. In the use of anti-obesity drugs,
motives of health and vanity overlap.
According to the Irish Times:
"A Danish pharmaceutical company behind popular new weight-loss drugs
has made payments totalling 345,000 to Irish health professionals and
organisations over the past three years.
"Novo Nordisk, the company behind the much-touted Ozempic and Wegovy
treatments for obesity and diabetes, describes the payments in support
of medical education as a cornerstone of its support for healthcare
professionals treating patients with serious chronic conditions.
"In the UK, the pharmaceutical industry association has suspended Novo
for two years over its marketing of another weight-loss drug, Saxenda,
saying it breached the industrys code of conduct. The company was
accused of failing to make clear its involvement in training on
weight-loss drugs offered to pharmacists on LinkedIn, according to the
Association of the British Pharmaceutical Industry.
"In response to the suspension, the Royal College of Physicians cut
links with the firm and returned outstanding grants."
and
"Novo Nordisk has become one of the biggest companies in Europe thanks
to soaring demand for Wegovy, used for chronic weight management.
"Wegovy has been hailed as a blockbuster new obesity treatment
worldwide though it is unlikely to be available in Ireland until next
year. Administered long term by weekly injection, it contains the
appetite suppressant semaglutide and is said to help patients lose up
to 15 per cent of their body weight. Ozempic, a diabetes drug with a
slightly lower dose of semaglutide, has become the darling of
celebrity dieters.
"Earlier this month [March 2023], the Observer newspaper in the UK
reported the company had paid 21.7 million to health organisations and
professionals in three years as part of a campaign to boost its
influence in the UK. It said those with links to the company went on
to promote Wegovy in media interviews and regulatory submissions
without always making their connections to the company clear.
and
"Critics of pharmaceutical sector transparency claim payments by drug
companies to doctors and other health professionals influence
prescribing habits. Research suggests the receipt of payments from the
pharma industry is associated with higher prescribing rates and costs
and lower prescribing quality, according to Dr James Larkin, a
researcher at the Royal College of Surgeons in Ireland.
"Dr Larkin said the transfers of value system for disclosing payments
'vastly underestimates' the actual amount of support provided by
industry, because some payments are not required to be disclosed and
areas such as generic drugs and medical devices are not covered."
https://www.irishtimes.com/health/2023/03/27/obesity-drug-firm-paid-health-staff-345000-over-three-years/
[2331]
"Novo Nordisk is paying the salaries of staff on NHS obesity teams and
financing the launch and redesign of services, including giving
206,000 to a health partnership to transform its treatment of obesity.
The Danish firm also has financial links to the co-chair of an NHS
England weight management advisory group, and paid her almost 50,000
in lecture, consulting and other fees in just two years."
and
"In some cases, recipients of the funding went on to praise Wegovy or
support its approval for use on the NHS without always making their
links to Novo clear. This weekend, the National Institute for Health
and Care Excellence (Nice) said an internal inquiry had found that
some of those who advised it on the use of Wegovy in the NHS had not
properly declared their interests.
"Now further documents reveal how Novo Nordisk has been granted a
potential role in shaping obesity treatment through partnerships with
NHS trusts, pharmacies and GPs to provide training and funding.
"In one case, the company is paying 206,000 to an integrated care
system to help it 'transform' its specialist obesity services and
'reduce unnecessary barriers' to treatment.
"Novos money is paying for two 'dedicated' staff members and
'independent facilitation support' for a partnership with Mid and
South Essex NHS trust and local councils, which aims to provide a
blueprint for transforming other weight loss services across the
country.
"In another partnership, Novo Nordisk has agreed to fund a weight
management nurse specialist to work at the Somerset NHS foundation
trust, which it has also partnered with to design an online weight
management course for patients.
"A separate initiative with the National Pharmacy Association aims to
'upskill pharmacists' in obesity medicine and help them launch new
weight management services. Novo is providing support with 'financial
tracking and ensuring delivery of outcomes' and funding to develop
resources for the two-year project.
"Novo Nordisk also has close links to the co-chair of an NHS England
advisory group on specialist weight management services. Prof Rachel
Batterham was appointed to the unpaid NHS role in 2021 despite a
longstanding relationship with the company. Disclosure UK records
which detail payments to healthcare professionals such as consulting,
lecture and conference fees show she was paid 16,306 in 'service fees'
by Novo in 2020 and 33,560 in 2021. She was also an investigator on a
Novo Nordisk-sponsored trial of its Wegovy (semaglutide) injections
and subsequently described the treatment as a 'gamechanger'."
https://www.theguardian.com/business/2023/apr/02/revealed-maker-of-wegovy-skinny-jab-is-funding-nhs-weight-loss-services
[2347]
And in June 2023 the Guardian reported:
"Payments to UK health professionals and organisations, including
donations, sponsorship, consultancy fees and expenses, reached a
record 200m in 2022, excluding R&D with companies seeking to
promote lucrative drugs for obesity, diabetes and heart conditions
among the biggest spenders."
Among the winners:
"Eli Lilly makes drugs for diabetes and is seeking approval for its
obesity drug Mounjaro, a rival to the recently approved Wegovy
injections. Records show it spent 3.5m on payments to NHS
organisations in 2022, up from 147,000 in 2018."
However
"The Association of the British Pharmaceutical Industry, a trade body
which publishes the Disclosure UK database of drugs industry spending,
said companies were required to be transparent about payments and were
banned from making payments that constituted an inducement to
prescribe or promote a medicine."
https://www.theguardian.com/business/2023/jul/08/revealed-pharma-giants-pour-millions-of-pounds-into-nhs-to-boost-drug-sales?utm_term=Autofeed&CMP=twt_gu&utm_medium&utm_source=Twitter#Echobox=1688857674
[2770]
Across the pond, "Over 100 members of Congress, who took money from
Danish giant Novo Nordisk, are pushing to make Medicare fund Ozempic
at $1,500/month." According to Robert F Kennedy, half of this would be
enough for three organic meals a day and gym membership, for every
obese American.
https://x.com/newstart_2024/status/1973431677239144675
[5453]
Meanwhile the side-effects are rolling in. The EMA is investigating
reports of suicidal ideation. You could be losing weight because you
are suffering from gastroparesis, and throwing up three times a day,
even a year after stopping the drug...
"...which works by mimicking a hormone called glucagon-like peptide 1
(GLP-1), regulating blood sugar levels and slowing down the rate at
which food leaves the stomach to create the feeling of fullness."
"'Gastrointestinal (GI) events are well-known side effects of the
GLP-1 class, the company [Novo Nordisk] told CNN. 'For semaglutide,
the majority of GI side effects are mild to moderate in severity and
of short duration. GLP-1s are known to cause a delay in gastric
emptying, as noted in the label of each of our GLP-1 RA medications.
Symptoms of delayed gastric emptying, nausea and vomiting are listed
as side effects.'"
But it's not the drug manufacturers who will be committing suicide:
"Brenda Allen, from Texas, has since been managing her nausea and
vomiting with a medication called Zofran and prescription
probiotics."
https://www.independent.co.uk/life-style/health-and-families/ozempic-stomach-paralysis-side-effects-b2381825.html?utm_medium=Social&utm_source=Twitter#Echobox=1690330909
[2853]
The FDA, MRHA, and the European Medicines Agency are all tracking
adverse reaction reports. In mixed messages...
"The ability of GLP-1s to lower blood sugar is a key reason drugs such
as Rybelsus (semaglutide) received FDA approval in 2019 for diabetes
treatment. According to Fiona Rutherford at Bloomberg, clinical trial
data in the US do 'not support warnings for suicidal thoughts or
behavior for the GLP-1s approved for diabetes indications.' 'In the
US,' she adds, 'the labels for Wegovy and Saxenda already include
warnings for suicidal behavior and thoughts, and recommend that
patients using these drugs are monitored for worsening symptoms.'"
Having historically had a policy of opposition to medication-induced
weight loss, the company Weightwatchers has made a u-turn:
"...since going all-in on GLP-1 agonists, WeightWatchers now has no
choice but to address the negative publicity tied to the drugs adverse
effects. Those hoping merely for reduced weight via GLP-1s may have to
contend instead with a rise in suicidal thinking, as well as severe
gastroparesis and cyclic vomiting syndrome that could derail their
lives completely."
https://www.madinamerica.com/2023/09/obesity-drugs-suicidal/
[2944]
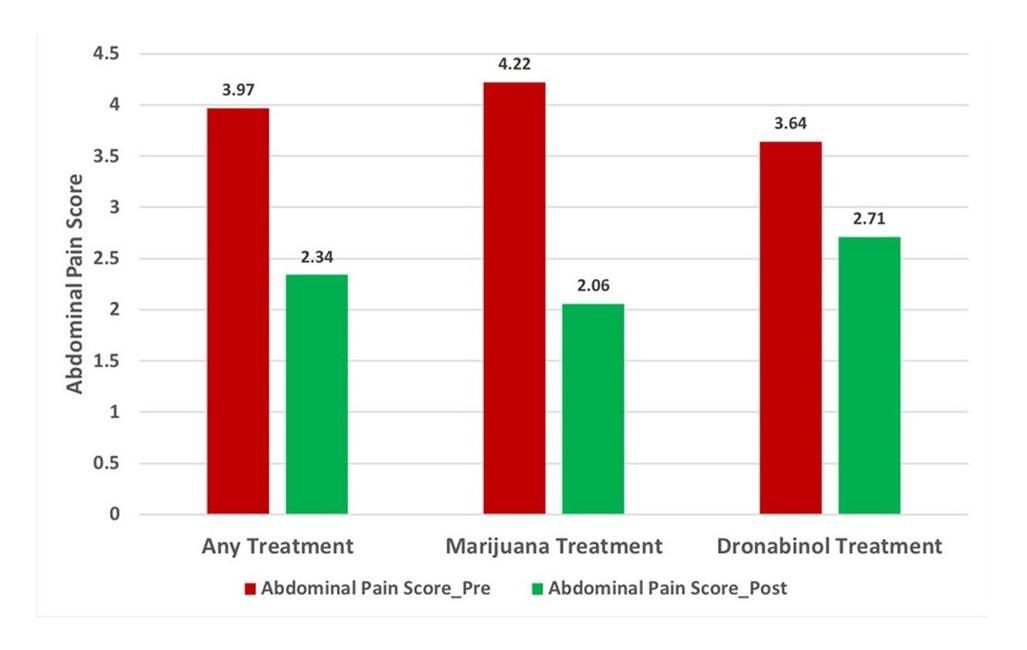
Fortunately, besides being an antidote to suicide, there is a
treatment for gastroparesis, according to Barbash et al (2018).
"Six patients were prescribed Dronabinol, ten were prescribed
marijuana and eight were prescribed Dronabinol followed by marijuana.
Paired sample Ttests were performed and statistically significant
improvement in abdominal pain score was seen in patients who received
either cannabinoid treatment. When analyzed individually, both
marijuana and Dronabinol showed statistically significant improvement
in abdominal pain scores as well.
"Conclusion: Our study shows that cannabinoids may play an important
role in the management of gastroparesisrelated abdominal pain. There
are currently no treatments shown to be effective for gastroparetic
pain in clinical trials, and cannabinoids may serve a niche for this
undertreated symptom."
https://journals.lww.com/ajg/fulltext/2018/10001/cannabinoids_lead_to_significant_improvement_in.1204.aspx
[3384]
Compared with similar people who didnt take GLP-1 medications, those
who did had about a 50% higher risk of being diagnosed with the
condition, at least three studies have shown.
https://edition.cnn.com/2024/05/20/health/glp-1-drugs-stomach-paralysis/index.html
[4664]
Hollywood restaurants have emptied in an "Ozempidemic", with various
celebs struggling as valiantly with addiction to weight loss and
looking like a meth-head with a hollowed-out "Ozempic face" as once
battled with obesity.
https://www.youtube.com/watch?v=YBbOidZffZs
[3107]
The side-effects keep on coming: "Semaglutide Reduces Cardiomyocyte
Size and Cardiac Mass in Lean and Obese Mice" say Martens et al
(2024).
https://www.sciencedirect.com/science/article/pii/S2452302X24002869?via%3Dihub
[3798]
And, says the American Academy of Ophthalmology and North American
Neuro-Ophthalmology Society, these safe and effective miracle drugs
may worsen your eyesight or make you go blind:
"A new study suggests patients taking semaglutide the active
ingredient in Ozempic and Wegovy may be at higher risk of developing
an eye condition that can cause blindness. Non-arteritic anterior
ischemic optic neuropathy or NAION, happens when blood flow to the
optic nerve is blocked, causing sudden, painless loss of vision in one
eye."
https://www.aao.org/newsroom/news-releases/detail/weight-loss-drug-and-eye-health
[3850]
"Thirty optic neuropathy lawsuits are pending in federal court, and
more than 40 in state court, according to court records cited by
Reuters."
https://childrenshealthdefense.org/defender/federal-court-consolidates-70-lawsuits-alleging-ozempic-wegovy-caused-vision-loss/?utm_source=x&utm_medium=social&utm_campaign=defender&utm_id=20251217
[5751]
Measured in column inches, such problems will receive much less
attention in the media compared to CaPs. "Cannabidiol represses
miR-143 to promote cardiomyocyte proliferation and heart regeneration
after myocardial infarction" say Ren et al (2024):
"Our results demonstrate that systemic administration (10 mg/kg) of
CBD markedly increased cardiac regenerative ability, reduced infarct
size, and restored cardiac function in MI mice. Consistently, in vitro
study also showed that CBD was able to promote the proliferation of
neonatal cardiomyocytes. Mechanistically, the expression of miR-1433p
related to cardiomyocyte proliferation was significantly
down-regulated in CBD-treated cardiomyocytes, while the overexpression
of miR-1433p inhibited cardiomyocyte mitosis and eliminated
CBD-induced cardiomyocyte proliferation. Moreover, CBD enhanced the
expression of Yap and Ctnnd1, which were demonstrated as the target
genes of miR-1433p. Silencing of Yap and Ctnnd1 hindered the
proliferative effects of CBD. We further revealed that inhibition of
the cannabinoid receptor 2 impeded the regulatory effect of CBD on
miR-1433p and its downstream target Yap/Ctnnd1, which ultimately
eliminated the pro-proliferative effect of CBD on neonatal and adult
cardiomyocytes. Taken together, CBD promotes cardiomyocyte
proliferation and heart regeneration after MI via miR-1433p/Yap/Ctnnd1
signaling pathway, which provides a new strategy for cardiac repair in
adult myocardium."
https://www.sciencedirect.com/science/article/abs/pii/S0014299923007598
[3799]
See also [1679].
According to a 21 March 2024 report by USA Today:
"More than five dozen lawsuits accuse Novo Nordisk or Eli Lilly of
failing to notify patients about the side effects of their popular
diabetes or weight loss drugs. Those drugs include Novo Nordisk's
Ozempic, Wegovy and Rybelsus, and Eli Lilly's Trulicity and Mounjaro.
These personal injury cases have been centralized under a federal
judge in Philadelphia because they share common elements involving the
same class of drugs.
"Among the more than five dozen lawsuits thus far, Novo Nordisk, maker
of Ozempic and Wegovy, faces the most suits. However, the attorneys
expect the case will eventually include thousands of others who say
they were harmed.
"In a statement, representatives of Novo Nordisk said the cases are
without merit and the company intends to 'vigorously defend against
these claims.'"
https://eu.usatoday.com/story/news/health/2024/03/21/lawsuits-ozempic-wegovy-weight-loss-drugs-diabetes-harmful/72947158007
[3111]
Mounjaro manufacturer Eli Lilly is defending a growing number of
claims. According to mass tort specialists King Law:
"The number of lawsuits targeting GLP-1 drug manufacturers, including
Eli Lilly, the maker of Trulicity, saw a 20% increase between August
and September. As of October 1, 2024, there were 1,090 cases pending
in MDL 3092 [believed to be a misprint for MDL 3094]. Increasing
reports of severe side effects from users of GLP-1 agonist drugs, like
Trulicity, have likely driven this rise in cases. With more Americans
taking these medications, legal experts predict tens of thousands of
additional lawsuits to be filed in the coming months."
https://www.robertkinglawfirm.com/personal-injury/trulicity-lawsuit/
[3612]
https://fingfx.thomsonreuters.com/gfx/legaldocs/znpnkkonzvl/fc191587-7a6d-4ef8-bbf6-6bf154db6aae.pdf
[3613]
The Defence asserts that no reasonably educated person would risk
taking big pharma's latest anti-obesity products when these companies
have such a dismal record and basically must be costing in the
litigation while keeping governments under control. Why would obese
people reject the proven, but unpatentable and prohibited alternative,
cannabis? Who would contine to worship this pharmaceutical mirage? Who
wouldn't know what's going on?
According to finance.si 6 July 2024:
"Farmacevtska industrija spet z rekordnimi plačili zdravnikom
Okoli 15 milijonov evrov je lani farmacija v Sloveniji plačala
organizacijam in zdravnikom za strokovne dogodke in udelebo, za
svetovanja, izobraevanja in preizkuanja zdravil."
https://www.finance.si/farmacevtska-industrija-spet-z-rekordnimi-placili-zdravnikom/a/9025921
[3347]
In more pain for the pharmaceutical industry, as alternatives to both
antidepressant and to oral anticoagulant drugs, CaPs reduce the risk
of gastrointestinal bleeding which are more likely in concomitant use,
as according to Rahman et al (2024):
"This study suggests that among patients with atrial fibrillation,
concomitant use of SSRIs and OACs was associated with an increased
risk of major bleeding compared with OAC use alone, requiring close
monitoring and management of risk factors for bleeding, particularly
in the first few months of use."
https://jamanetwork.com/journals/jamanetworkopen/articlepdf/2816687/rahman_2024_oi_240142_1710523887.19892.pdf
[4727]
Prescription drugs and accidents: FRIEND
Almost four fifths of 2183 pain and mental health patients reduced
opioid use after switching to cannabis.
"93.36% of these reported a change in pain medication after medical
cannabis. The majority of participants (79%) reported either cessation
or reduction in pain medication use following initiation of medical
cannabis and 11.47% described improved functioning."
and
"Most (90.59%) reported that medical cannabis was very or extremely
helpful when dealing with their medical condition; less than 2%
reported it as slightly or not helpful at all. Over 85% reported
medical cannabis products were very or extremely important to their
quality of life (88.67%)."
https://www.tandfonline.com/doi/full/10.1080/10826084.2022.2107673
[1690]
The National Bureau of Economic Research found reductions in Workers'
Compensation claims in RML states. They found declines in such filings
both in terms of the propensity to receive benefits and benefit amount
in states that have enacted the policy change.
Further, they identified complementary declines in non-traumatic
workplace injury rates and the incidence of work-limiting disabilities
in legal states.
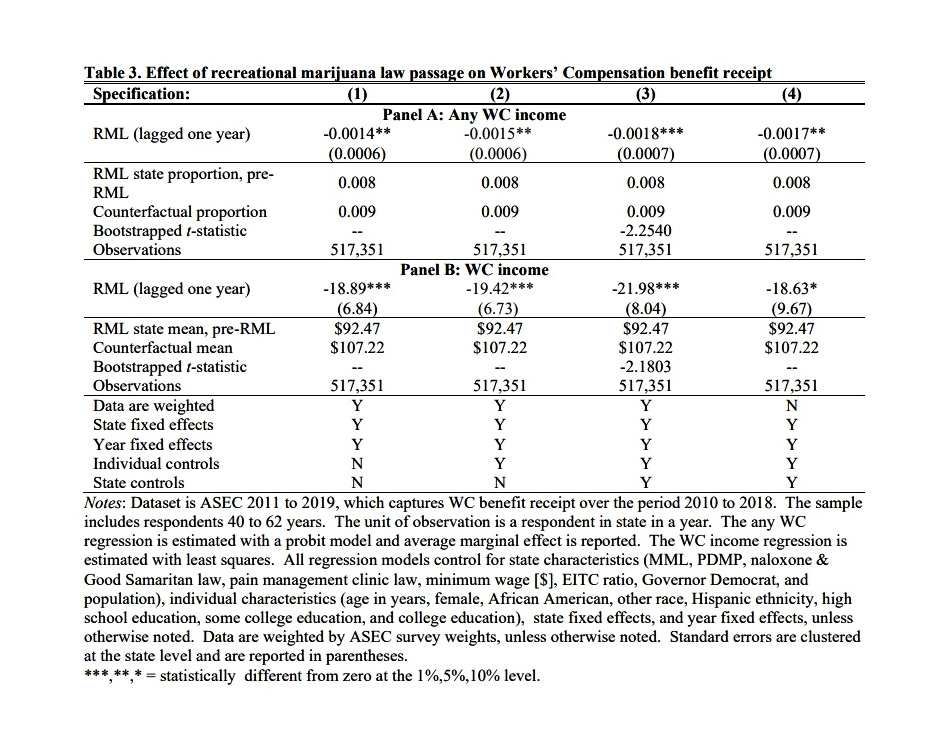
"There are many pathways through which RMLs could reduce WC benefit
receipt. We conjecture that improvements in the management of chronic
pain and other health condition symptoms play a key role in the
observed findings."
https://www.nber.org/system/files/working_papers/w28471/w28471.pdf
[1995]
In a similar vein, after just 23 years, workplace fatalities were
reduced by a third in states with medical marijuana laws. According to
Anderson et al at the University of Montana:
"Participants: All 50 states and the District of Columbia for the
period 1992-2015.
"Measurements: Workplace fatalities by state and year were obtained
from the Bureau of Labor Statistics. Regression models were adjusted
for state demographics, the unemployment rate, state fixed effects,
and year fixed effects.
"Findings: Legalizing medical marijuana was associated with a 19.5%
reduction in the expected number of workplace fatalities among workers
aged 25-44 (incident rate ratio [IRR], .805; 95% CI, .662-.979). The
association between legalizing medical marijuana and workplace
fatalities among workers aged 16-24, although negative, was not
statistically significant at conventional levels. The association
between legalizing medical marijuana and workplace fatalities among
workers aged 25-44 grew stronger over time. Five years after coming
into effect, MMLs were associated with a 41.1% reduction in the
expected number of workplace fatalities (IRR, .663; 95% CI,
.482-.912). MMLs that listed pain as a qualifying condition or allowed
collective cultivation were associated with larger reductions in
fatalities among workers aged 25-44 than those that did not.
"Conclusions: The results provide evidence that legalizing medical
marijuana improved workplace safety for workers aged 25-44. Further
investigation is required to determine whether this result is
attributable to reductions in the consumption of alcohol and other
substances that impair cognitive function, memory, and motor
skills."
https://scholarworks.montana.edu/xmlui/bitstream/1/15294/1/Anderson_MML_and_Workplace_Fatalities_06_13_18_v5.pdf
[2019]
If workplace fatalities would be associated with a reduction of one
third without the ZPPPD, the ZPPPD would be associated with a 50%
increase in workplace fatalities.
That would be five or six deaths - there were 17 in Slovenia in 2020,
according to Eurostat, and 16872 non-fatal accidents at work besides.
Europe-wide we see 3355 deaths at work in 2020. The U of Montana
findings were that the improvement grew over time, a period when the
stigma of cannabis use would have presumably diminished. The authors
adjusted for recreational legalization, meaning that even better
results could have been obtained had they not. The authors also find a
greater reduction in states where pain was included as a qualifying
condition. The Montana authors also manage to find a milquetoast way
of dealing with an awful possibility, when they say "the effects of
legalizing recreational marijuana and decriminalizing marijuana could
be similar to the effects of legalizing medical marijuana". Well why
would they be worse? Does the marijuana know whether it is medical or
recreational? It does not. Worse yet, there is no reason to suppose
legally smoked cannabis is any more effective in this regard that
illegally smoked cannabis.
Therefore the ZPPPD is a dangerous piece of legislation, not only
because it encourages people like Mr Teodorović and the Police to
manipulate each other for their own imagined gain, but for the very
simple straightforward reason of this association with workplace
fatalities, among the many other damages attributable to its
restraining effect on marijuana as a choice.
All the ZPPPD has going for it is, it is a law, and has a big sack of
woo woo on its side from people whose interest in occupational injury
is probably limited to their compensation claims.
Why can't they sue the government for increasing this risk? Sunk cost
error, along with an emotional and economic attachment to the woo woo
have killed 1379 EU workers in one year.
Measuring after five years of (at least) MMLs, they found a 41.1%
reduction in fatalities. It is fairly simple to transpose the
nationwide Montana findings [2019] to the Eurostat figures and
multiplying 3355 by 0.441 suggests that had the combined anti-cannabis
laws of the Member States been abandoned in 2015 the number of deaths
in 2020 would have been 1379 lower, at 1976. Therefore I propose the
ZPPPD is an extermination. Just another government extermination
dressed up as a health measure.
https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Accidents_at_work_statistics#Number_of_accidents
[2024]
In Ptuj sized units, in the smarter-five-years-ago scenario,
Slovenia's seven avoidable 2020 workplace fatalities is 2.33 Dreveneks
per year. Europe-wide it's 459.67 Dreveneks per year.
In past-year cannabis users, Toronto researchers Zhang et al found a
19% lower incidence of workplace injury during the same period.
"We performed a cross-sectional analysis of the Canadian Community
Health Survey (201316) of working individuals. We used multiple
logistic regression modelling to calculate the odds of experiencing a
work-related injury (defined as non-repetitive strain injury) among
workers who reported using cannabis more than once during the prior 12
months as compared to non-users. We repeated the analysis among
participants working in high injury risk occupational groups only.
"Among the 136 536 working participants, 2577 (2%) had a work-related
injury in the last 12 months. Of these 2577 who had a work-related
injury, 4% also reported being a cannabis user in the same period. We
found no association between past-year cannabis use and work-related
injury (odds ratio for work injury among users 0.81, 95% confidence
interval 0.660.99). The association was unchanged in the subgroup
analysis limited to high injury risk occupational groups.
and concluded
"We found no evidence that cannabis users experienced higher rates of
work-related injuries. While awaiting prospective studies,
occupational medicine practitioners should take a risk-based approach
to drafting workplace cannabis policies."
This was the largest study sample I could find on work-related
injuries, but cannabis use may be underreported as the survey preceded
legalisation in Canada. Previous work is mentioned, viz.:
"Our finding was consistent with, but expanded upon, a number of
smaller studies published previously. In a study of 5466 job
applicants with the US postal service, Normand et al. found that
testing positive for illicit drugs (including cannabis) during
pre-employment screening did not increase the risk of injury or
accidents occurrence. Similarly, an analysis of over 12 000 young
people in the USA showed that the life-time use of cannabis did not
increase the incidence of occupational injuries. In contrast, a
cross-sectional New Zealand study of 15 687 employed individuals in
various sectors found that cannabis use in the last 12 months did
slightly increase the risk of work injuries, but the authors did not
adjust for other potential confounding variables in the model.
Wadsworth et al. conducted a community based survey of 7979
individuals in the UK and found that cannabis use in the past year was
not associated with increased odds of work incidents, but increased
the odds of overall incidents (e.g. accidents, road traffic accidents,
minor injuries, cognitive failures). This is similar to the result of
another cross-sectional analysis of 27 934 survey subjects in Spain
which showed that cannabis use in the last 12 months was not
associated with injuries at work but seemed to increase the frequency
of overall non-traffic injuries."
In contrast to cannabis,
"Factors associated with increased odds of injury included male sex
(OR 1.55, 95% CI 1.411.71), non-white ethnicity (OR 1.34, 95% CI
1.171.53), history of back problems (OR 1.75, 95% CI 1.611.93),
migraine headaches (OR 1.24, 95% CI 1.101.41), mood disorder (OR 1.46,
95% CI 1.2711.67), smoking (OR 1.31, 95% CI 1.201.43) and workplace
stress (OR 1.76, 95% CI 1.611.93). Participants working in industry
(OR 3.16, 95% CI 2.753.62), trades (OR 2.98, 95% CI 2.653.36) or sales
and services (OR 1.99, 95% CI 1.772.23) occupational groups were
significantly more likely to report work-related injuries."
Besides its size, the most remarkable thing about this paper is the
downplaying of the result. Nowhere do terms like "inverse association"
or "negative relationship" appear!
Having failed to produce a result assistive of the drug war, do the
authors discuss the possibility that cannabis users are safer, perhaps
more careful, less reckless people?
Far from it - the authors redefine this alarmingly positive outcome as
merely "no evidence of higher rates". One out of five accidents are
somehow absent in the cannabis cohort, yet this cannot be applauded,
obviously.
Maybe they have fewer accidents because they are smoking weed in the
factory yard instead of working. The researchers are not thinking or
behaving very scientifically at all.
https://academic.oup.com/occmed/article/70/8/570/5941608
[2091]
According to Cannatech today:
"Historically, in every single jurisdiction on earth where
legalization was pursued and achieved, without exception, there were
cannabis opponents spreading anti-cannabis myths and half-truths to
try to deter voters or lawmakers from supporting reform.
"One of the most popular areas of focus for cannabis opponents was,
and presumably always will be, impaired driving. The talking point can
come about in a variety of forms, however, the main premise of the
talking point regardless of how it manifests itself is this that if
cannabis laws are reformed there will be terror on the roadways in the
form of increased vehicle crashes.
"Unfortunately for cannabis opponents, and fortunately for
rational-thinking people worldwide, the data does not support
opponents claims."
https://cannatechtoday.com/how-is-canadian-legalization-impacting-traffic-crashes/
[2612]
In a Canadian sample of 2745 workers:
"Overall, 11.3 per cent of workers in the sample experienced a
workplace injury, but the risk of injury was different for those who
used cannabis at work and those who did not. When compared to those
who did not use cannabis in the past year, the risk of workplace
injury for those who reported workplace use over the past year
(specifically including use during a shift or up to two hours before)
was two-fold higher (a risk ratio of 1.97). In contrast, for workers
who used cannabis in the past year but not before or at work, the
injury risk was not statistically different from that of workers who
did not use cannabis in the past year.
"These results underscore the importance of distinguishing cannabis
use at work and off work when examining the link with injury risk.
Rather than considering any cannabis use as an occupational safety
risk, this finding suggests that workplaces need to reframe their
focus on use that is likely to lead to impairment at work."
https://iwh.on.ca/sites/iwh/files/iwh/reports/iwh_issue_briefing_cannabis_use_by_workers_2024.pdf
[3894]
In Ohio:
"...voters approved marijuana legalization in November 2023, with use
and possession becoming legal the following month. Adult-use cannabis
sales, meanwhile, began last August."
Fatal accidents fell 30%, according to data from the Ohio State
Highway Patrol.
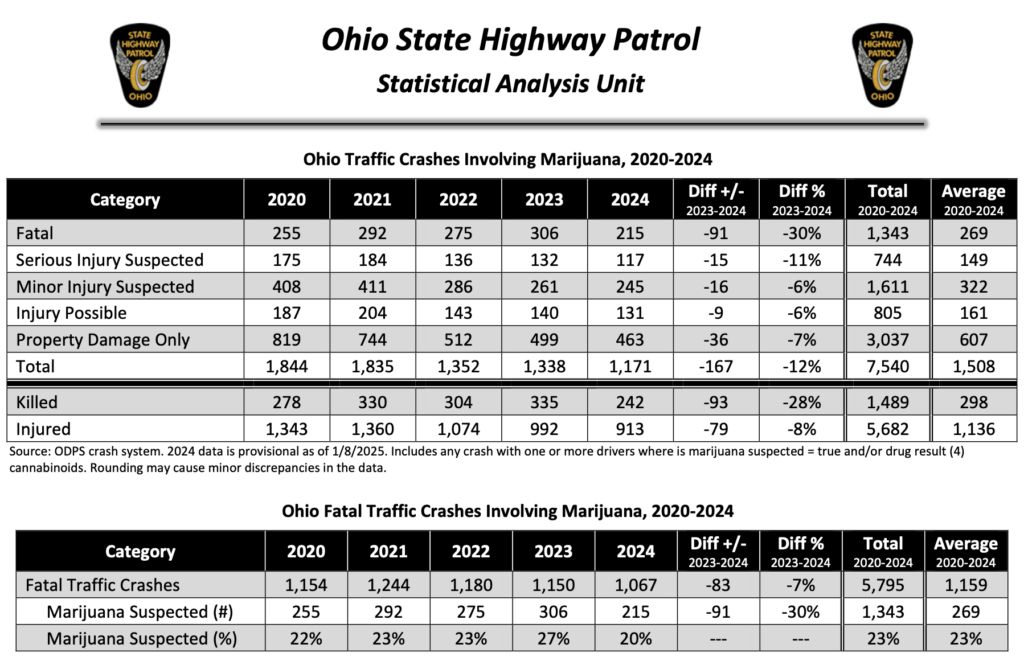
"All told, there were 1,067 fatal traffic crashes in Ohio during
2024the lowest number in at least five years, and down 7 percent from
the 1,150 fatal crashes in 2023.
Of those, about 20 percent (215 crashes) were linked to cannabis last
yearalso the lowest number in years, and down from 27 percent (306
crashes) in 2023."
https://www.marijuanamoment.net/fatal-traffic-crashes-linked-to-marijuana-fell-by-30-in-ohio-last-year-as-legalization-took-effect-contrary-to-opponents-fears/
[3893]
In "Marijuana laws and pedestrian fatalities in the United States"
(2022) Dewey and Vadlamani at Department of the Data Science &
Business Analytics, Florida Polytechnic University, Lakeland found a
highly statistically significant fall in daytime pedestrian deaths and
a fall in night-time deaths.
They included cyclists and skateboarders, and "other personal
conveyances" so scooters in this study of the whole USA for 35 years
from 1985 through 2019.
"MMLs are followed by a statistically significant reduction in overall
fatalities and in daytime fatalities involving alcohol. Nighttime
fatalities involving alcohol decline as well, but the decline is not
statistically significant. Following RMLs, there is a statistically
significant decline in alcohol related daytime fatalities and a
decline in nighttime alcohol related fatalities that is not
statistically significant. There is no apparent change in daytime or
nighttime nonalcohol related fatalities related to either MMLs or
RMLs. Taken together, our results mirror findings regarding the
effects of MMLs on total traffic fatalities, and the pattern of
changes in alcohol related fatalities suggests the alcohol
substitution hypothesis is at work. States bordering RML states see an
apparent decline in nighttime alcohol related fatalities and increase
in nighttime non-alcohol related fatalities, but these are
insignificant statistically. Moreover, they start prior to the RMLs
effective date, and thus appear not directly related to liberalization
in neighboring states.
"One might at first expect the effects of RMLs to be larger than the
continued effects associated with MMLs. However, the analysis of
marijuana laws in Dewey et al. suggests most variation in marijuana
laws is associated with a single underlying dimension of state
permissiveness toward marijuana use, and that permissiveness is well
captured by the presence of an MML. Therefore, in practice, the
difference between a state with an old MML but no RML and with an old
MML and a RML may be less than it at first seems."
And their data leads them to conclude:
"Liberalization, and RMLs in particular, may eventually be shown to
lead to more pedestrian fatalities under some sets of circumstances.
However, as of 2019, we find liberalization has been associated with
lower pedestrian fatalities, not higher. Further, the pattern is
consistent with the alcohol substitution hypothesis. Specifically, the
induced decline in alcohol related fatalities following liberalization
is large enough to more than compensate for any additional fatalities
due to marijuana consumption. While there has been an increase in
pedestrian fatalities concurrent with liberalization of marijuana use
laws, and particularly RMLs, there is no evidence to suggest it is due
to that liberalization. To the contrary, if anything liberalization
appears to have reduced the size of the increase."
https://www.sciencedirect.com/science/article/pii/S0386111223000067
[2263]
Up in Canada, M J Armstrong from the Department of Finance, Operations
& Information Systems at Brock University was researching exactly
that alcohol substitution hypothesis...
"Specifically, he discovered that for every dollar of legal marijuana
sold, there was a tie to declines in alcohol sales between 74 to 84
Canadian cents. Prof. Armstrong says the findings are not causative
though it does suggest that alcohol is being replaced by cannabis.
Additionally, he found that sales of alcohol from 2017 to 2018 were
around 1.8% less than they would have been, had Canada not regulated
medical cannabis.
"'The negative association was robust to several alternative modeling
choices,' he writes.
"'From an academic perspective, this study found evidence that
cannabis on average was a substitute, not a complement, for alcohol in
Canada. This suggests cannabis might also have a substitution effect
in other countries that legalize it, though that remains to be seen,'
says Professor Armstrong in the paper.
"'From a public health perspective, the results likewise imply that
reductions in alcohol-related health impacts might partly offset the
increased cannabis-related health impacts that legalization might
bring,' he continues. 'Furthermore, medical cannabis presumably
improves the health of at least some patients by treating symptoms
that alcohol had merely masked,' Armstrong says."
https://cannabis.net/blog/news/the-cannabis-correlation-every-1-spent-on-cannabis-leads-to-a-drop-in-alcohol-sales-of-0.75-to
[2613]
https://dr.library.brocku.ca/bitstream/handle/10464/17045/ArmstrongMJ_MedicalCannabisAlcohol_Appendix.pdf;jsessionid=6E7863AD5A0CCC4A65F8F23585AF8CE3?sequence=2
[2614]
Kam Insight's 2024 report "The Future of Socialising" tells us that
58% of UK psychotropic-curious consumers say their consumption of
alcohol declined when taking Cannabis or Psychedelics.
https://kaminsight.com/wp-content/uploads/sites/2044/2024/07/KAM-X-High-Dry-The-Future-of-Socialising-2024.pdf
[3249]
In Toronto:
"Regardless of the outcome, neither the CCA nor the NCS [number of
cannabis stores, per capita] is associated with concomitant changes in
the outcomes. In hybrid DID [difference-in-difference] models, the CCA
is associated with non-significant decreases of 9% (incidence rate
ratio 0.91, 95% confidence interval 0.74,1.11) in traffic crashes and
in the hybrid-fuzzy DID models, the NCS are associated with
nonsignificant decreases of 3% (95% confidence interval - 9%, 4%) in
the same outcome."
https://onlinelibrary.wiley.com/doi/pdf/10.1111/dar.13678
[2609]
It was a similar story in Ontario generally, and in Alberta:
"There was no evidence of significant changes associated with cannabis
legalization on post-legalization weekly counts of drivers
traffic-injury ED visits in: (1) Alberta, all drivers (n = 52,752
traffic-injury presentations), an increase of 9.17 visits (95 % CI
-18.85; 37.20; p = 0.52); (2) Alberta, youth drivers (n = 3265
presentations), a decrease of 0.66 visits (95 % CI -2.26; 0.94; p =
0.42); (3) Ontario, all drivers (n = 186,921 presentations), an
increase of 28.93 visits (95 % CI -26.32; 84.19; p = 0.30); and (4)
Ontario, youth drivers (n = 4565), an increase of 0.09 visits (95 % CI
-6.25; 6.42; p = 0.98)."
https://www.sciencedirect.com/science/article/abs/pii/S0376871621005032
[2610]
Another Canadian study examined
"ED visits in Ontario and Alberta and hospitalizations in Ontario,
Alberta, British Columbia, the Prairies (Manitoba and Saskatchewan)
and the Maritimes (Nova Scotia, New Brunswick, Newfoundland and Prince
Edward Island)."
for
"motor vehicle injury or pedestrian/cyclist injury"
and Walker et al say
"There were no statistically significant changes in rates of ED visits
and hospitalizations for motor vehicle or pedestrian/cyclist injury
after RCL after accounting for multiple testing. After COVID-19, there
was an immediate decrease in the rate of ED visits for motor vehicle
injury that was statistically significant only in Ontario (level
change β = −16.07 in Ontario, 95% CI = −20.55 to
−11.60, P = 0.000; β = −10.34 in Alberta, 95% CI =
−17.80 to −2.89, P = 0.008; α of 0.004) and no
changes in rates of hospitalizations.
"Conclusions: Canadas recreational cannabis legalization did not
notably impact motor vehicle and pedestrian/cyclist injury. The rate
of emergency department visits for motor vehicle injury decreased
immediately after COVID-19 lockdowns, resulting in rates below
post-recreational cannabis legalization levels in the year after
COVID-19."
https://onlinelibrary.wiley.com/doi/pdf/10.1111/add.16188
[2610]
In good news for the auto insurance industry...
"In California, Maine, Massachusetts, and Nevada four states that
fully legalized marijuana in 2016 traffic fatalities declined or
remained the same in the three years that followed, compared to a
slight increase in states where it remained illegal.
"A comprehensive study of traffic data in the U.S. and Canada failed
to find a statistically significant change in accidents and fatalities
after legalization.
"Alcohol, which remains fully legal in all 50 states and D.C., is a
factor in nearly a third of all automotive fatalities."
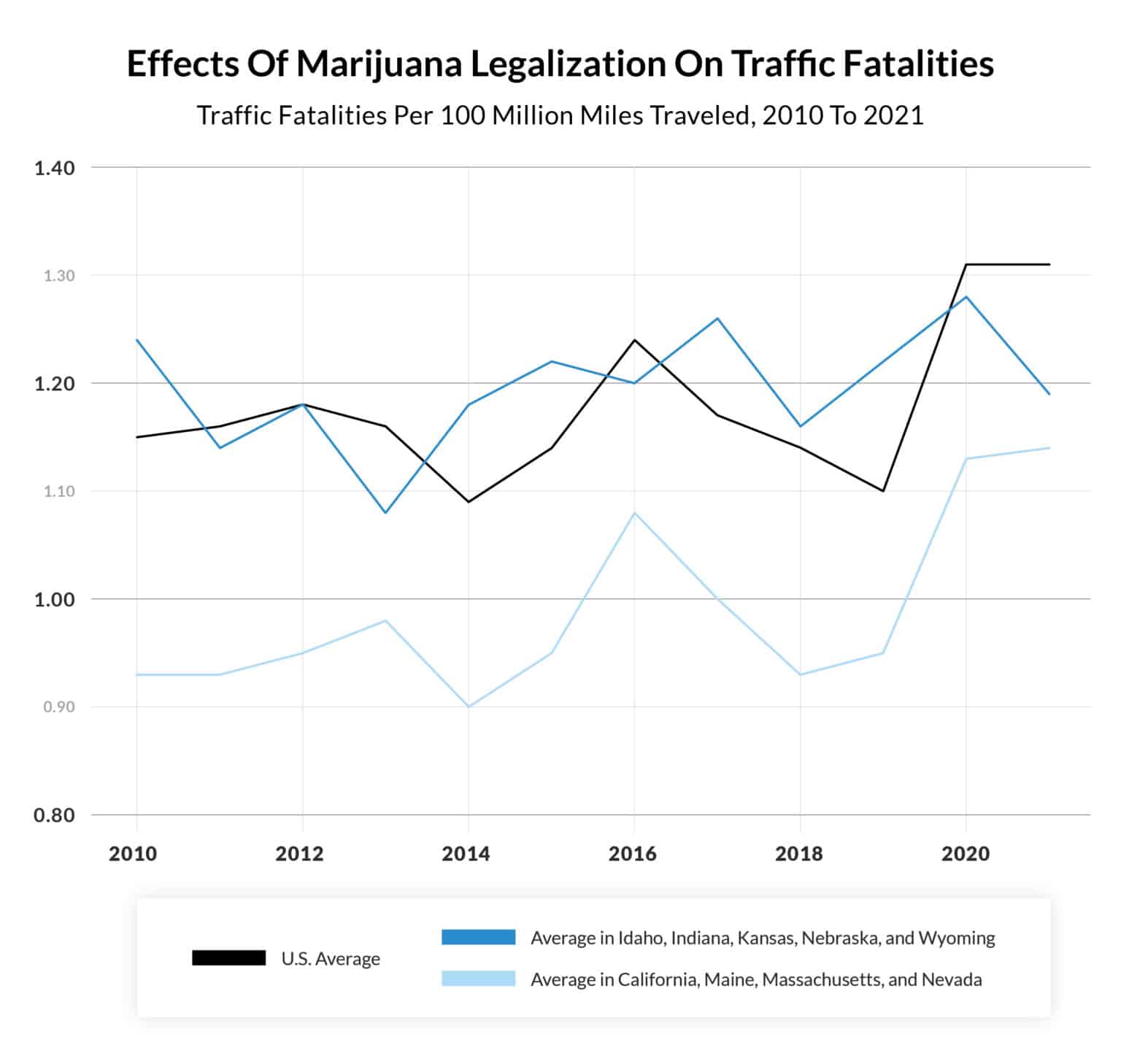
https://qz.com/advisor/auto-insurance/has-marijuana-legalization-made-roads-less-safe/
[4271]
Had an accident? Conversion of a hospital visit into a hospital
admission was more likely in alcohol positive RTA/MVA victims:
"10 322 injured drivers visited a participating trauma centre
between 2018 and 2023. 1649 (16.0%), 1716 (16.6%) and 463 (4.5%)
drivers had detectable levels of alcohol, THC or both, respectively.
Compared with sober drivers (BAC=0), drivers with 0%<BAC<0.08%
had increased odds of admission (aOR=1.69, 95% CI=1.31 to
2.19), as did drivers with BAC≥0.08% (aOR=1.36, 95% CI=1.16
to 1.60). THC did not modify the relationship between alcohol and
admission. Neither alcohol nor THC predicted were associated with
length of stay following admission."
https://injuryprevention.bmj.com/content/early/2025/07/16/ip-2025-045642
[5250]
Police car chases are a great American, if not Slovenian, tradition
and on Youtube a large proportion of fleeing vehicles seem to contain
marijuana. Not infrequently this is the only reason for flight.
There are no official statistics on how many die in vehicular flight
because they have CaPs on board, but in one year according to the San
Francisco Chronicle:
"We found that at least 551 people, or more than 25% of those killed,
were bystanders. In addition, the vast majority of these pursuits were
initiated over traffic violations and nonviolent crimes such as
shoplifting, not serious felonies."
...
"From 2017 through 2022, at least 3,336 people died in police
chases."
https://www.sfchronicle.com/projects/2024/police-chases-database/
[5393]
https://www.sfchronicle.com/projects/2024/police-chases/
[5394]
The Defence hopes that it can be easily understood that no one needs
to flee from the Police because of CaPs if they are legal, and
therefore a reduction in this effect is included in the Benedictions
on commonsense grounds, although this benefit, like many others,
relies on legal status and is not an effect of the substances
themselves.
Given the association between cannabis and lower impulsivity [3923] it would make sense for users to flee less, independent of
legality. Interestingly the highest death rates were found in the
non-RM states of Alabama and Georgia.
Policing styles and rules authorising vehicular pursuits vary by
state, making comparisons with marijuana laws useless. However early
legalisation adopters such as California, Colorado and Alaska were
below the average deaths per 100k, according to a 2017 report. The
Defence predicts less rather than more car chase fatalities from the
destigmatization process as a logical effect, but cannot say how much
less. As, rather like CaPs interdiction in general...
"The DOJ does not report the justifications for each pursuit."
https://finance.yahoo.com/news/states-deadliest-police-chases-144217749.html?guccounter=1
[5395]
Commenting on the fifth anniversary of legalisation in Canada
"Zac Walsh, professor of psychology at the University of British
Columbia, says he thinks during this time, the industry has lost some
of the stigmas that were previously attached to it and has become more
normalized in society."
and he thinks that
We have our own cannabis system, the endocannabinoid system, and plant
cannabis binds with those same receptors. So our body is actually more
geared to accept cannabis as opposed to sort of the blanket effects of
alcohol.
"Cannabis has always been a controversial substance, but since
legalization, Walsh says, most Canadians recognize that if they are a
cannabis user, it has made a big difference in their life. And if
theyre not, it probably hasnt.
"'People have been using cannabis for thousands of years and it seems
like just a basic liberty issue that people should be able to grow a
plant and use it as they see fit if its not hurting anyone else,' he
added."
https://globalnews.ca/news/10030910/cannabis-in-canada-from-stigma-to-normalcy-the-5-year-journey-since-legalization/
[4007]
But some people don't want fewer workplace fatalities and illness.
Raman and Bradford note that:
"In August [2016], the pharmaceutical company Insys Therapeutics also
cited concerns for child safety when, with a $500,000 contribution, it
became the largest donor to Arizonas anti-legalization drive. But
their stated concerns have raised a few eyebrows across the state.
Insys manufactures Subsys, a prescription painkiller derived from
fentanyl, the synthetic opioid that is up to 100 times more powerful
than morphine."
and
"Besides Insys, the Arizona Wine and Spirits Wholesale Association
gave one of the largest donations to the states anti-legalization
campaign when it paid $10,000 to Arizonans for Responsible Drug
Policy. And the Beer Distributors PAC recently donated $25,000 to the
Campaign for a Safe and Healthy Massachusetts, making it the states
third-largest backer of the opposition to recreational cannabis.
"Purdue Pharma and Abbott Laboratories, makers of the painkiller
OxyContin and Vicodin, respectively, are among the largest
contributors to the Anti-Drug Coalition of America, according to a
report in the Nation. And the Pharmaceutical Research and
Manufacturers of America, considered one of marijuanas biggest
opponents, spent nearly $19m on lobbying in 2015."
https://www.theguardian.com/sustainable-business/2016/oct/22/recreational-marijuana-legalization-big-business?CMP=share_btn_tw
[1677]
The pharmaceutical industry takes a serious economic hit after states
legalize marijuanawith an average market loss of nearly $10 billion
for drugmakers per each legalization eventaccording to a
first-of-its-kind study.
The peer-reviewed research article, published in the journal PLOS ONE,
looked at stock return and prescription drug sales data for 556
pharmaceutical companies over 25 years of state cannabis legalisation,
analyzing market trends before and after the enactment of medical and
adult-use cannabis legalization laws at the state level.
The stock returns were 1.5-2 percent lower at 10 days after
legalization, the study authors found. Returns decreased in response
to both medical and recreational legalization, for both generic and
brand drugmakers. Investors anticipate a single legalization event to
reduce drugmaker annual sales by $3 billion on average.
The California Polytechnic State University and University of New
Mexico researchers said:
By expanding access and, thus use, legalization could permit cannabis
to compete with conventional pharmaceuticals. Largely unpatentable,
cannabis may act like a new generic entrant following medical
legalization, leading some individuals to substitute away from other
drugs toward cannabis. However, unlike a conventional new generic
drug, cannabis use is not restricted to a single or limited set of
conditions. This means that cannabis acts as a new entrant across many
different drug markets simultaneously.
We find the average change in a firms market value per legalization
event is $63 million with a total impact on market value across firms
per event of $9.8 billion, the study says.
The study also factored in shifts in pharmaceutical drug sales
post-legalization.
Using the historical price-to-sales ratio of drugmakers for the year
associated with each legalization event, this implies a change in
annual sales across all drugmakers of $3 billion per event, it
says.
Taking these findings a step further, the researchers also estimated
that predicted annual prescription drug spending would have been $1
billion lower in 2014 if all 30 states without legal medical cannabis
in 2014 had legalized medical cannabis.
In addition to capturing a larger number of drugs, a larger number of
conditions, and all payers, our estimate may be larger also because,
unlike [researchers on a previous study], who take drug prices as
given, our estimate captures the competitive pressure on prices that
cannabis puts on both brand and generic drugmakers for both
prescription and over-the-counter drugs, it says.
The authors note there are some caveats:
The economic significance of an estimated $9.8 billion loss in market
value across firms per cannabis legalization event is extremely large,
however our results should be interpreted cautiously. A key limitation
is that we model investors as rational, which may overstate the
economic significance of our results. Second, we are limited to
publicly traded firms and past legalization events. Third, we note
that estimates may be sensitive to our choice of using 150 to 50 days
before the legalization event. Finally, we expect there to be
measurement error due to heterogeneity in the legalization and
subsequent regulatory processes.
For private and public drugmakers, we expect the response to
legalization to include investment and marketing, the study concludes,
citing the fact that Pfizer spent billions to acquire a biotech
company that focuses on cannabinoid-type therapies."
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0272492
[1518]
For comparison, according to thebusinessresearchcompany.com...
"The antidepressants market size has grown steadily in recent years.
It will grow from $16.6 billion in 2023 to $17.32 billion in 2024 at a
compound annual growth rate (CAGR) of 4.3%."
https://www.thebusinessresearchcompany.com/report/antidepressant-global-market-report
[3503]
ceskenoviny.cz reported 9 July 2024 that Czech National Drug
Coordinator Jindřich Vobořil had resigned, citing pressure from "some
major industries":
"Because of his approach, he got into a dispute with politicians, for
example in promoting a regulated cannabis market or taxing silent
wine, but also after his commentary on finding cocaine in the
House."
https://www.ceskenoviny.cz/zpravy/protidrogovy-koordinator-voboril-se-rozhodl-odstoupit/2541571
[3234]
Towards the end of 2024 Mravčk et al considered "New legislative
framework for control of psychoactive substances in Czechia" in the
International Journal of Drug Policy, pointing out the failure of the
international treaties and the creation of the worst possible outcome
in the cases of both licit and illicit drugs.
"Acknowledging the potential benefits of such psychoactive substances
and balancing them with potential harms, it suggests stringent rules
for marketing, safety, and preventing sales to minors. This approach
aims to quell illicit markets, safeguard vulnerable populations, and
encourage controlled use."
https://www.sciencedirect.com/science/article/abs/pii/S0955395924002871
[3585]
It is difficult to see why allopathic medicine is trusted at all any
more. A partial history of settlements against pharmaceutical
companies:
https://en.wikipedia.org/wiki/List_of_largest_pharmaceutical_settlements
[3391]
The egregious behaviour of Johnson & Johnson is recounted in in
Gardiner Harriss "No More Tears: The Dark Secrets of Johnson &
Johnson" reviewed here:
https://newrepublic.com/article/194726/johnson-and-johnson-investigation-crimes-health-care-system
[5026]
Off-label promotion settlements:
https://en.wikipedia.org/wiki/List_of_off-label_promotion_pharmaceutical_settlements
[3392]
Actions by the European Commission and national competition
authorities in Europe:
"Between 2018 and 2022, the EC and the NCAs adopted an average of five
pharma-related antitrust decisions per year compared to only three
decisions per year between 2009 and 2017.
"The total amount of fines imposed was around 1.1 billion across a
nine-year period from 2009 to 2017, and about 773 million across the
five-year period from 2018 to 2022, and the average fine per
infringement decision remained around the same level (about 46
million).
"The UK Competition and Markets Authority (CMA) (five decisions) led
the enforcement efforts prior to the end of the transition period,
followed by the Romanian Competition Council (RCC) (four decisions)
and the Belgian Competition Authority (BCA) and Italian Competition
Authority (ICA) (three decisions each). Within the same period, the EC
adopted two decisions (Aspen and Teva-Cephalon).
"The EC and the NCAs have pursued several novel theories of harm in
recent years (eg, excessive pricing and vexatious litigation) and have
not shied away from broadening the scope of existing theories (eg,
disparagement)."

https://globalcompetitionreview.com/review/the-european-middle-east-and-african-antitrust-review/2025/article/european-union-pharmaceutical-sector-investigations-signal-increased-focus-broadened-theories-of-harm
[3393]
Vix medicatrix naturae: ENEMY
Self-rebalancing in illness is not helpful to sales of medical props.
Discoveries about the microbiome, the endocannabinoid system and
homeostatic lipid messengers
"Relation to homeostasis
Walter Cannon's notion of homeostasis also has its origins in vis
medicatrix naturae. 'All that I have done thus far in reviewing the
various protective and stabilizing devices of the body is to present a
modern interpretation of the natural vis medicatrix.' In this, Cannon
stands in contrast to Claude Bernard (the father of modern
physiology), and his earlier idea of milieu interieur that he proposed
to replace vitalistic ideas about the body. However, both the notions
of homeostasis and milieu interieur are ones concerned with how the
body's physiology regulates itself through multiple mechanical
equilibrium adjustment feedbacks rather than nonmechanistic life
forces.
"Relation to evolutionary medicine
More recently, evolutionary medicine has identified many medical
symptoms such as fever, inflammation, sickness behavior, and morning
sickness as evolved adaptations that function as darwinian medicatrix
naturae due to their selection as means to protect, heal, or restore
the injured, infected or physiologically disrupted body.
https://en.wikipedia.org/wiki/Vis_medicatrix_naturae
[2738]
Medicofinancial bloat: FRIEND
For example:
"Objectives: Patients with treatment-resistant depression (TRD)
experience high relapse rates and a relentless cycle of ineffective
treatments, significantly impairing their quality of life and
burdening healthcare resources. Psilocybin has emerged as a promising
alternative, offering rapid and sustained symptom relief. However, its
cost-effectiveness remains unexplored. This study conducted a
pioneering cost-effectiveness analysis of psilocybin-assisted therapy
(PAT) versus standard care (SoC) for individuals with TRD using a
Markov model from a U.S. healthcare perspective. Methods: The model,
parameterized by randomized trial efficacy data and a micro-costing
approach, simulated patient transitions every six-week cycle,
consistent with American Psychiatric Association guidelines. Outcomes
focused on response/remission rates and incremental cost-effectiveness
ratios (ICERs), expressed in 2023 U.S. dollars per quality-adjusted
life years (QALYs). Extensive deterministic and probabilistic
sensitivity analyses (PSA) explored uncertainties. Dosing and price
point variations were also examined in scenario analysis to identify
optimal strategies. Results: Psilocybin consistently dominated SoC,
providing cost savings (ΔCosts = -$7,037) and superior clinical
benefits (ΔQALY = 0.10). PAT increased remission by 3.20% and
response by 7.75%, gaining between 0.15 and 0.25 QALYs. The PSA
demonstrated an 81.98% likelihood of PAT being optimal at a
$50,000/QALY threshold, with 65.89% of iterations showing greater
effectiveness at lower costs. Notably, the Incremental Net Monetary
Benefit (INMB) analysis indicated a value of $12,765 at this
threshold, reinforcing PAT's cost-effectiveness. No scenario
identified SoC as more cost-effective. PAT retained its superiority
across all willingness-to-pay (WTP) values (from $50,000 to $200,000)
and remained the optimal strategy across all price levels evaluated
(from $500 to $10,000). Scenario analysis revealed that administering
two doses three weeks apart was the most cost-effective regimen.
Conclusions: Psilocybin offers a groundbreaking, cost-effective
alternative to SoC for TRD. These findings support its integration
into treatment protocols, warrant further research into its long-term
benefits, and position PAT as a promising strategy for future clinical
guidelines"
https://scholar.stjohns.edu/theses_dissertations/896/
[6014]
Stigma: FRIEND
Who can we stigmatise first? Women!
"This study found that motivations for cannabis consumption by people
with endometriosis internationally are comparable to those previously
reported in Australia and New Zealand (Armour et al. 2019b , Sinclair
et al. 2021b , 2023a ). In addition, significant associations were
observed for the non-legal therapeutic cohort relating to the negative
impact of cannabis-associated stigma, breaking the law, and
potentially losing employment or driving licences due to prevailing
laws or workplace drug policies, which mirror concerns from previous
research in Australia and New Zealand (Sinclair et al. 2023a )." [5082]
"The most common description of stigma comes from sociologist Erving
Goffman, who defined it as, 'an attribute that is deeply discrediting
that causes one's identity to be 'spoiled' compared to the dominant
group.' He divided stigma into three types: those linked to
'abomination of the body' (e.g., physical disability); those that
incite 'tribal' responses (e.g., race, religion); and those derived
from 'character traits' (e.g., drug use, mental illness, HIV status).
Published in 1963, Goffman's theory is dated but remains influential.
For instance, the Government of Canada defines stigma as 'negative
attitudes, beliefs or behaviours about or towards a group of people
because of their situation in life.' This is a limited depiction of
how and why stigma emerges, who benefits from enacting it, and the
different ways it is sustained.
"Specifically, stigma is not stable. Whether a certain characteristic
is stigmatized is constantly negotiated and re-negotiated, and this
changes over time. Consider that homosexuality was once criminalized,
and it later appeared as a mental disorder in psychiatric texts.
Although queerness is still 'non-normal' in some contexts, general
responses to it have shifted dramatically alongside legislation,
policy, and evolving trends in medicine. Drug use is no different.
Before anti-drug laws were implemented, and long before 'substance use
disorders' existed as official diagnoses, drug use was deemed neutral.
It became stigmatized as the 'war on drugs' escalated and, with it, so
too did racial, ethnical, religious, and class-based inequalities.
Important to remember is that in both the cases of sexuality and drug
use, alterations in public perception have been due to grassroots
activism and civil disobedience.
"Next, stigma is not just interpersonal. It is more trenchant than
individual attitudes and behaviours, and stigma becomes
institutionalized and systemic when official policies (in housing,
employment, education, the child welfare system, and so on) prohibit
entrance based on identification with a particular class. For example,
compulsory attendance at 12-step meetings as a condition of not being
re-incarcerated reflects this latter type of stigma. So too do
requirements placed on healthcare professionals who have been to
addiction treatment who must complete regular drug tests to remain
employed.
"Finally, stigma becomes internalized. Research on this phenomena
repeatedly concludes that viewing oneself as 'bad,' 'Mad,' and/or
'diseased,' which is an outcome of institutionalized and systemic
stigma, leads to negative outcomes. People who are stigmatized begin
to anticipate rejection, they may alter behaviour based on these
expectations, and their material conditions deteriorate. This is
especially true of people who are stigmatized on multiple axes, which
highlights that drug use alone is not a sufficient condition for being
stigmatized. Those who use drugs but are otherwise stably housed,
employed, and part of dominant racial and cultural groups can consume
with near-impunity. Anti-stigma campaigns, then, which address drug
use and drug use alone, may not be effective because this is just one
facet of one's identity."
https://www.drugpolicy.ca/critical-terminology-guide/
[1007]
Stigma comes from the top:
"Cannabis is commonly characterized as the most normalized illicit
drug. However, it remains a prohibited substance in most parts of the
world, including Europe, and users can still be subject to
stigmatization. The objective of this study is to assess to what
extent and how cannabis users in different countries with different
cannabis policies perceive, experience and respond to stigmatization.
We conducted a survey in the Dutch coffeeshops among 1225 last year
cannabis users from seven European countries, with national cannabis
policies ranging from relatively liberal to punitive. Three dimensions
of cannabis-related stigma were investigated (discrimination,
perceived devaluation and alienation) and a sum score was used to
reflect the general level of stigmatization. Perceived devaluation was
the highest-scoring dimension of stigma and discrimination the
lowest-scoring. The general level of stigmatization was lowest in the
Netherlands and highest in Greece. This indicates that punitive
cannabis policy is associated with stigma and liberal cannabis policy
is associated with de-stigmatization. Besides country, daily cannabis
use was also found to be a significant predictor of stigma, but
gender, age, household type and employment status were not."
https://www.researchgate.net/publication/347939939_Cannabis_users_and_stigma_A_comparison_of_users_from_European_countries_with_different_cannabis_policies/link/601a735845851589397ab034/download
[2026]
In "'I'm Treated Way Differently': The Intersectional Risk Environment
of Maternal Cannabis Use" Gould et al (2025) describe how superstition
makes its way through the institutions, even in California:
"Participants who used cannabis during pregnancy described: 1) how
their race/ethnicity, gender, and socioeconomic status impacted their
care experiences together with their cannabis use, 2) their experience
of poor perinatal care due to their insurance coverage and location of
care, 3) worsening of care after disclosing cannabis use (e.g., being
judged, ignored), and 4) removal from perinatal care after disclosing
cannabis use."
https://www.tandfonline.com/doi/full/10.1080/10826084.2025.2568153?src=exp-la
[5464]
As soon as we recognize a stigma - which might be masquerading as a
health concern, a public safety concern, a concern about
"appropriateness", or a concern about immigrants...however it is
dressed up - we should look to the laws against that stigma, however
it is portrayed. It is up to the stigmatisers to prove their empirical
bases.
"A woman from the Bronx has been awarded a $75,000 settlement after
city officials wrongfully attempted to take her baby away due to her
cannabis use during pregnancy. The case highlights the ongoing debate
and stigma surrounding cannabis use, especially among expectant
mothers. "
https://cannadelics.com/2023/09/14/cannabis-use-during-pregnancy-bronx-woman-wins-75k-settlement/
[2990]
This represents the first grinding of the rocks, where an individual
is obliged to confront the system in the courts. Subsequently, when it
is obvious both that the discrimination is egregious, and that such
cases cannot and should not be repeated ad nauseam, a practical
solution is miraculously found. Thus cannabisculture.com reported in
December 2023 that:
"California employees will soon officially have protections from
discrimination based on their use of cannabis or marijuana while off
the clock and away from the workplace.
"The new protections come from an amendment to Californias Fair
Employment and Housing Act (AB 2188) which was approved by Governor
Gavin Newsom on Sept. 18, 2022, and goes into effect on Jan. 1, 2024.
The bill makes it unlawful for an employer to not hire, penalize, or
terminate a person based on their use of cannabis products outside of
work.
"Although California was the first state to legalize medical marijuana
in 1996 and became one of the first to legalize the recreational use
of marijuana in 2016, AB 2188 is the first law in the Golden State to
specifically provide workplace protections for employees who use it
for either reason."
https://www.cannabisculture.com/content/2023/12/16/new-cannabis-laws-in-california-to-protect-employees-take-effect-in-2024/
[4286]
A hitherto invisible aspect of recreational or nootropic drug research
is the situation of the researchers themselves. This was recently
confronted in "'Hes used drugs - hes biased! Hes not a drug user -
what would he know!': A Cross-sectional, Online Study of Drug
Researchers Experiential Knowledge of Drug Use and Disclosure" (2024),
wherein Ompad et al found:
"86 % of drug researchers reported drug use.
"59 % of drug researchers disclosed use at their institutions
or organizations and 11% in their research/scholarship.
"Drug use experiences can positively inform research- but stigma is a
barrier.
"Researchers believe drug use could strengthen research questions.
"If disclosing use, there are concerns that research would not be seen
as objective."
...although no one seems to raise such concerns about research by
non-users.
"Of the sample (n=669, 43 countries), 52 % were cisgender
women, 89 % had post-graduate education, and 79 % worked
in academia. Most (86 %) reported lifetime drug use and
47 % past 3-month use. Among 557 researchers who used drugs,
59 % disclosed their use to institutional colleagues,
59 % to colleagues outside their institution, 25 % to
research participants, and 11 % in their research/scholarship.
Themes included frequency; context; meaning of drug use disclosure
personally, professionally, and socially; and how drug use experience
and disclosure informs research. Respondents connected their concerns
about disclosure in research with issues of social identity,
professional risk, and the role of stigma related to lived experience.
Some respondents felt that such concerns reinforce a vacuum, noting
that the inability to disclose drug use limits research questions and
the knowledge base overall."
https://www.sciencedirect.com/science/article/pii/S2772724624000404
Scientific neutrality: ENEMY
In Ireland:
"Civil society expressed concern that dissent is not well-tolerated
within the current system directing drugs policy.
"One representative said that a decision maker in a Government
organisation told the board of their civil society group that they
'have no right to criticise government policy' as they were in receipt
of State funds.
"Another individual agreed that this happens, and that there is 'an
underlying understanding that if you are too critical, you could lose
your funding sometimes it is explicit, sometimes it is implicit'."
https://crainn.com/2024/06/25/government-used-pre-selected-figures-to-influence-drug-policy/
[3171]
Establishment Religion: FRIEND.
"Gisela Kreglinger, in her book The Spirituality of Wine", notes that
the rise of drugs has accompanied the decline of religious belief and
practices." [265]
Democracy is prohibition's ENEMY. Cannabis and psychedelics have never
been prohibited by public plebiscite. No society en masse has ever
called for them to be outlawed. Any agitation has been of a
conservative, top-down nature.
One state Governor determined to prevent the Benedictions is Kristi
Noem of South Dakota. In 2019, Noem even vetoed a bill to legalize
industrial hemp because she viewed it as a possible first step toward
recreational legalization.
In 2022, the state Senate passed two different legalization bills, as
well as measure to expunge prior cannabis convictions and create a tax
structure for legal sales. Noem won't rule our vetoing these because
she is personally anti-marijuana. Her hatred of fun is apparently
pathological.
"Voters [had] already approved adult-use legalization at the ballot in
2020, but it was invalidated by the state Supreme Court following a
single-subject legal challenge funded by the Noem administration."
https://www.marijuanamoment.net/south-dakota-governor-wont-rule-out-vetoing-marijuana-legalization-bill-that-passed-the-senate/
[1011]
Prohibitionists might see political profit in cannabis referendums.
Interestingly no other food consumption behaviours or medical
interventions are chosen democratically on a population basis.
Crime: FRIEND
Prohibition creates crime.
Crime is created which would be impossible without prohibition.
Overdoses and overdose deaths: FRIEND
Ray et al (2023) examined the effects of drug interdiction on local
overdoses in Marion County, Indiana, which includes Indianapolis and a
population of one million, and found
"Within 7, 14, and 21 days, opioid-related law enforcement drug
seizures were significantly associated with increased spatiotemporal
clustering of overdoses within radii of 100, 250, and 500 meters. For
example, the observed number of fatal overdoses was two-fold higher
than expected under the null distribution within 7 days and 500 meters
following opioid-related seizures. To a lesser extent,
stimulant-related drug seizures were associated with increased
spatiotemporal clustering overdose.
"Conclusions. Supply-side enforcement interventions and drug policies
should be further explored to determine whether they exacerbate an
ongoing overdose epidemic and negatively affect the nations life
expectancy.
Figure 4 shows the fold change observed vs. expected
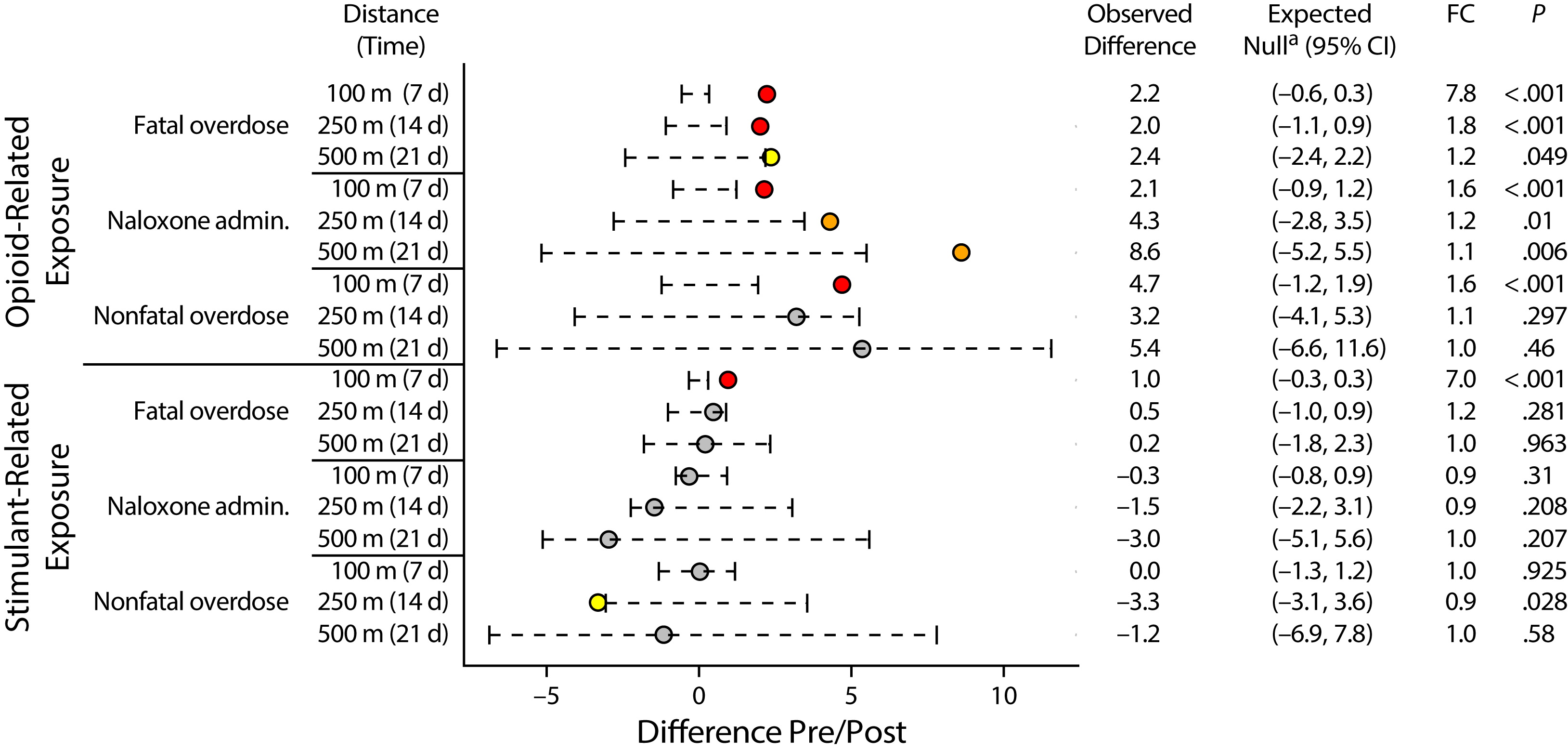
https://ajph.aphapublications.org/doi/full/10.2105/AJPH.2023.307291?role=tab
[2690]
Recreational marijuana had been legal in Oregon for six years
when...
"Ballot Measure 110 was approved by Oregon voters in the November 2020
election. BM 110 reduced the penalties for most Possession of a
Controlled Substance (PCS) offenses from a felony or misdemeanor to a
new Class E violation, punishable with a $100 maximum fine."
https://www.oregon.gov/das/oea/pages/ballot-measure-110-savings.aspx#:~:text=Ballot%20Measure%20110%20was%20approved,effect%20on%20February%201%2C%202021. [3048]
Recreational marijuana had been legal for eight years in Washington
state when...
"Because the Washington State Supreme Court declared the statute
unconstitutional, Washington courts will apply State v. Blake to
anyone convicted under the RCW 69.50.4013 statute. This means
convictions may be vacated, dismissed, etc., by an order from the
court."
https://kingcounty.gov/en/legacy/initiatives/felony-drug-possession-blake-decision#:~:text=In%20February%202021%2C%20the%20Washington,of%20the%20Courts%20(AOC). [3049]
In "One-Year Association of Drug Possession Law Change With Fatal Drug
Overdose in Oregon and Washington" Joshi et al (2023) asked:
"Question Were laws that fully or partially decriminalize drug
possession in Oregon and Washington associated with fatal drug
overdose rates 1 year post implementation?
"Findings In this cohort study using synthetic control analysis, laws
decriminalizing drug possession in Oregon and Washington were not
associated with changes in fatal drug overdose rates in either state.
The average rate difference in Oregon post change was 0.268 fatal drug
overdoses per 100 000 state population, while the average rate
difference in Washington post change was 0.112 fatal drug overdoses
per 100 000 state population.
"Meaning The findings of this study suggest that legal changes to
remove or decrease criminal penalties for drug possession are not
associated with the fatal drug overdose rate 1-year post
implementation.
"Importance Two states modified laws to remove or substantially reduce
criminal penalties for any drug possession. The hypothesis was that
removing criminal penalties for drug possession may reduce fatal drug
overdoses due to reduced incarceration and increased calls for help at
the scene of an overdose.
"Objective To evaluate whether decriminalization of drug possession in
Oregon and Washington was associated with changes in either direction
in fatal drug overdose rates.
"Design, Setting, and Participants This cohort study used a synthetic
control method approach to examine whether there were changes in drug
possession laws and fatal drug overdose rates in Oregon and Washington
in the postpolicy period (February 1, 2021, to March 31, 2022, in
Oregon and March 1, 2021, to March 31, 2022, in Washington). A
counterfactual comparison group (synthetic controls) was created for
Oregon and Washington, using 48 states and the District of Columbia,
that did not implement similar policies during the study period
(January 1, 2018, to March 31, 2022). For 2018-2021, final multiple
cause-of-death data from the National Vital Statistics System (NVSS)
were used. For 2022, provisional NVSS data were used. Drug overdose
deaths were identified using International Statistical Classification
of Diseases and Related Health Problems, 10th Revision underlying
cause-of-death codes X40-X44, X60-X64, X85, and Y10-Y14.
"Exposures In Oregon, Measure 110 went into effect on February 1,
2021. In Washington, the Washington Supreme Court decision in State v
Blake occurred on February 25, 2021.
"Main Outcome Monthly fatal drug overdose rates."
https://jamanetwork.com/journals/jamapsychiatry/article-abstract/2809867?utm_source=twitter&utm_campaign=content-shareicons&utm_content=article_engagement&utm_medium=social&utm_term=092723
[3047]
Lawyers: FRIENDS
Lawyers and legal staff benefit from prohibition as NECUD ensures more
accidents. Lawyers also profit by perpetuating the prosecution of FOBs
and ROBs. All of the crime and domestic violence which would have been
prevented by substitution of alcohol by cannabis and psychedelics is a
gain for the legal profession. Litigation for pharmaceutical drug
harms is reduced by provision of alternatives.
----------------------------------------------------------------------------
The Englishman stands for the rights of everyone disadvantaged,
discriminated against, persecuted, and prosecuted on the false or
absent bases of prohibition, and also believes the victims of these
officially-sanctioned prejudices have been appallingly treated and
should be pardoned and compensated.
The Englishman requests the return of his
CaPs and other
rightful property, for whose distraint Slovenia has proffered no
credible excuse or cause.
The Benedictions represent both empirical entities as well as beliefs.
Beliefs which the Defence evidence shows may be reasonably and
earnestly held about the positive benefits of CaPs at the population
level, in which the good overwhelmingly outweighs the bad. Below, the
latest version of this dynamic list.
THE BENEDICTIONS
REFERENCES
TIMELINE OF DRUG LAW v. SCIENCE