BRAIN VOLUMES
As with other areas of anti-cannabis legislation the literature on
attention deficit hyperactivity disorder is strewn with the debris of
officialdom not knowing what it did not know.
Pim Ittiphakorn, Simon Erridge, and Mikael Sodergren of Imperial
College London, James Rucker of Kings College London, and Carl Holvey
and Ross Coomber of Sapphire Medical Clinics, explain what we now
believe about cannabis and ADHD - "now" meaning 6 December 2023:
"Attention-deficit/hyperactivity disorder (ADHD) is one of the most
common psychiatric disorders, with an estimated global prevalence of
5% in children and 2.5% in adults. The estimated incidence of ADHD
diagnosis has increased by approximately 42% in children between 2003
and 2011, and 123% in adults between 2007 and 2016 in the United
States. ADHD is characterized by symptoms of inattentiveness,
hyperactivity, and impulsiveness causing functional impairment in two
or more settings (e.g., work and home). ADHD is often associated with
psychosocial difficulties, such as relationship problems,
unemployment, educational underachievement, and criminality. Moreover,
ADHD is also associated with a higher incidence of sleep disturbance
and psychiatric co-morbidities, including anxiety, substance misuse,
and depression. As a result, these issues can significantly reduce the
quality of life for individuals with ADHD.
"Current treatment for ADHD consists of a combination of
psychological therapies and both stimulant and non-stimulant
medications. Stimulants are the most commonly prescribed medications
for ADHD and target executive and attentional function. They are
considered relatively safe and effective treatments, however, they are
commonly associated with decreased appetite, insomnia, emotional
dysregulation, irritability, and an increased risk of adverse
cardiovascular events. Non-stimulant medications have been shown to
reduce ADHD-related functional impairments and co-occurring mood
disorders. Despite their effectiveness, medication adherence rates are
relatively low due to the adverse events that are commonly
experienced. This highlights the need for novel therapeutics for
ADHD.
"The endocannabinoid system (ECS) plays a vital role in cognitive
function, motor coordination, and emotional homeostasis, in addition
to the regulation of dopaminergic pathways in the brain. The ECS is a
signaling network consisting of endocannabinoids, enzymes, and
cannabinoid receptors, including cannabinoid type 1 (CB1) receptors
and cannabinoid type 2 (CB2) receptors. Dysregulation in the ECS has
been implicated in the pathophysiology of ADHD. CB1 receptors are
widely distributed throughout the central nervous system, with high
levels found in regions associated with cognitive functioning and
processing, such as the basal ganglia, cerebellum, neocortex, and
hippocampus."
https://onlinelibrary.wiley.com/doi/10.1002/npr2.1240
[4264]
Although ADHD's roots as a concept can be traced back to 1798, people
didn't really believe in physiological bases for behavioural disorders
until a lot later.
In 2010 Klaus W Lange worked at the Department of Biological and
Abnormal Psychology, University of Regensburg. According to Lange et
al's "The history of attention deficit hyperactivity disorder"
printed, appropriately enough, in Attention Deficit Hyperactivity
Disorder, it was in 1902 that "defective moral control" gained a
semblance of scientific definition, focussing on
"(1) passionateness; (2) spitefulness cruelty; (3) jealousy; (4)
lawlessness; (5) dishonesty; (6) wanton mischievousness
destructiveness; (7) shamelessness immodesty; (8) sexual immorality;
and (9) viciousness. The keynote of these qualities is
self-gratification, the immediate gratification of self without regard
either to the good of others or to the larger and more remote good of
self."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3000907/
[1888]
George F Still attempts to wrestle with the evidence using the tools
available at the time, which basically amount to listening to stories,
a physical examination, and measuring the circumference of the
troubled kids' above-average sized heads:
"Another boy was brought to me at the age of five years with a
history that for two months he had been very excitable and had at the
same time become extremely spiteful, throwing things at people
apparently in wanton spitefulness and attacking strange children in
the street without any provocation ; he had expressed a wish one day
to 'chop his mothers head off with a chopper,' and was caught one day
in the act of putting the cat into the fire, and on a subsequent
occasion- he attempted to put it into a copper of boiling water. I saw
this boy 18 months later when he was said still to be very excitable
and extremely passionate, kicking or striking anyone who offended him.
Nine months previously he had hit his mother on the head with a big
toy gun because he could not have some trifling thing that he wanted;
he was also said to be spiteful to other children. He was untruthful,
but his lying was of the purely romantic type, so much so that it was
difficult to imagine that the boy intended to deceive. His head was
unusually large, measuring 21⅜ inches in maximum circumference at the
age of six and a half years. He is a heavylooking but well-grown boy
and he is fully up to the average in school attainments. His maternal
grandfather had diabetes, one maternal uncle attempted suicide twice,
and two other maternal uncles have become confirmed drunkards. The
boys parents are respectable middle-class people and seemed to give
the child excellent care."
Dr Still noticed some things we would today ascribe to other
syndromes: the pronounced epicanthic folds perhaps of fetal alcohol
syndrome, or the repetitive actions of obsessive compulsive disorder.
He looks for suspected causes in the medical histories of family
members. By today's statistical standards, Still's collection of case
histories is nothing more than anecdotal. But it's from here the idea
of a hyperkinetic disorder begins to take shape, culminating in the
new name attention deficit disorder (ADD) in 1980.
https://ia800708.us.archive.org/view_archive.php?archive=/22/items/crossref-pre-1909-scholarly-works/10.1016%252Fs0140-6736%252801%252970006-2.zip&file=10.1016%252Fs0140-6736%252801%252970022-0.pdf
[1889]
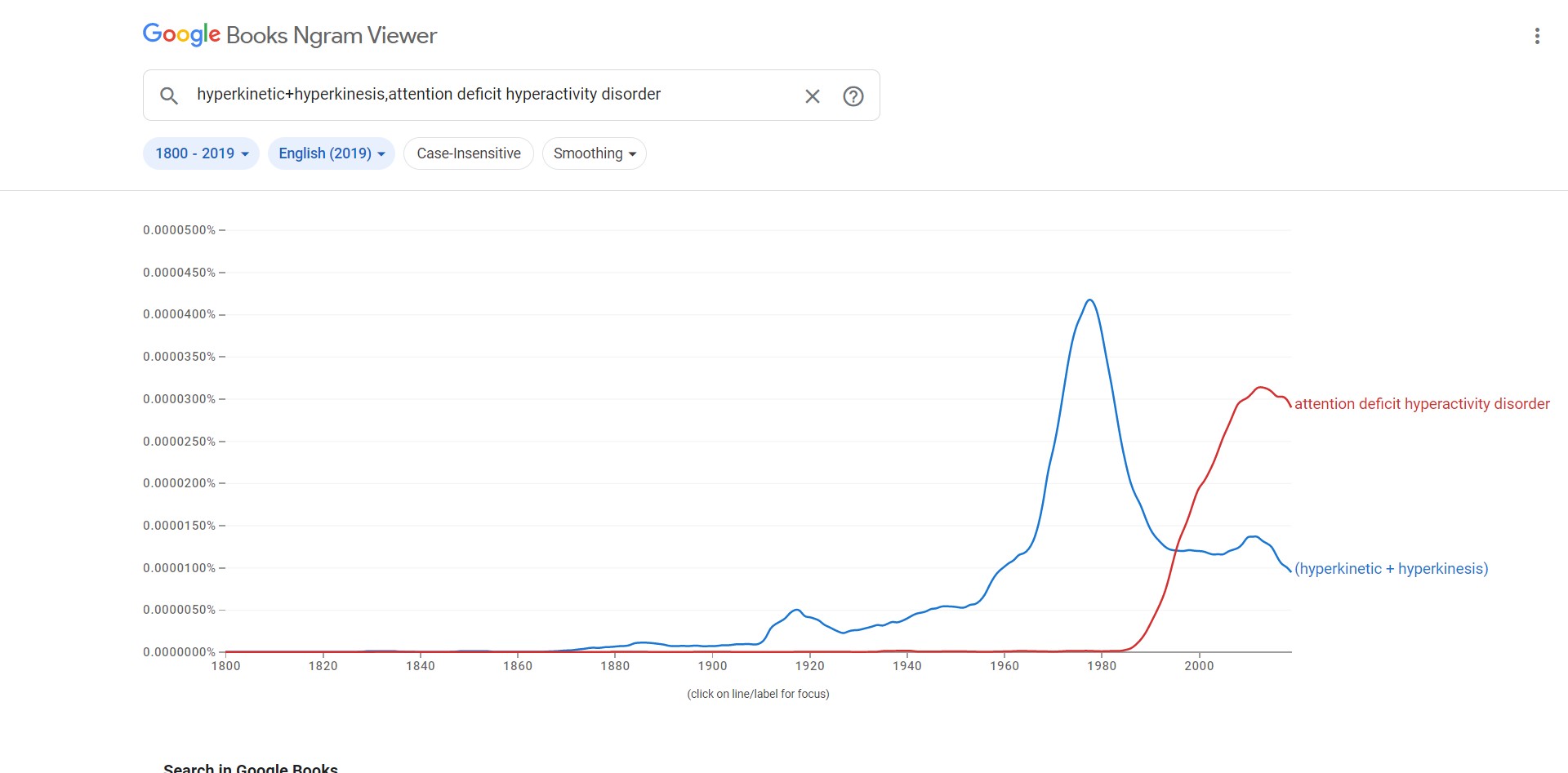
Here's how the nomenclature looks in the English corpus
Here's a diagram to help explain the neurobiology of ADHD, as it was
understood in 2011.
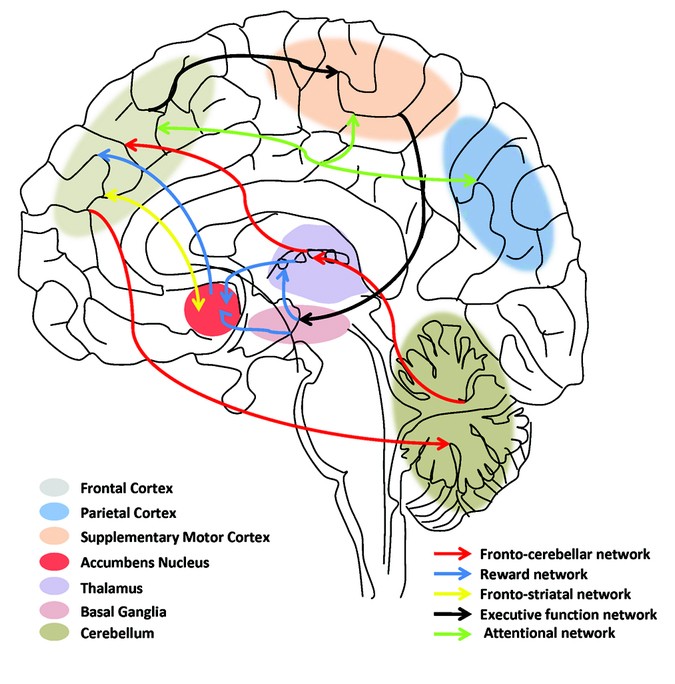
According to these French authors,
"A study of pregnant mothers related or unrelated to their child as a
result of in vitro fertilization showed that prenatal stress was
linked to ADHD only when mothers were related to their child,
suggesting that the association may be accounted for by inherited
factors. A recent twin study focused on ADHD-related conditions
(antisocial behavior and substance use disorders in young adults), has
provided an important insight into mechanisms of gene-environment
influence on externalizing disorders by showing that genetic factors
contribute more to the development of behavioral symptoms in a context
of high environmental adversity, in accordance with a diathesis-stress
model. These examples illustrate the importance of genetically
informed study designs to further disentangle environmental and
genetic contributions to ADHD."
https://www.nature.com/articles/pr9201196
[2008]
From New York to Australia, Isik et al (2023) have been looking at
"Neurodevelopmental outcomes in children after prenatal marijuana
exposure"
"This study evaluated the association between PME and
neuropsychological test scores in late childhood and early adulthood,
accounting for a wide range of parental characteristics.
"Methods: This study evaluated participants from the Raine Study, a
cohort of 2868 children born between 1989 and 1992 [formerly known as
the West Australian Pregnancy Cohort Study]. Children whose mothers
provided information on marijuana use during pregnancy were included.
The primary outcome was the Clinical Evaluation of Language
Fundamentals (CELF) at age 10. Secondary outcomes included the Peabody
Picture Vocabulary Test (PPVT), Child Behaviour Checklist (CBCL),
McCarron Assessment of Neuromuscular Development (MAND), Coloured
Progressive Matrices (CPM), Symbol Digit Modality Test (SDMT) and
Autism Spectrum Quotient (AQ) scores. Exposed and unexposed children
were matched by propensity score using optimal full matching. Missing
covariate data were imputed using multiple imputation. Inverse
probability of censoring weighting (IPCW) was used to adjust for
missing outcome data. Linear regression within matched sets, adjusted
by IPCW, evaluated score differences between exposed and unexposed
children. As a secondary analysis, modified Poisson regression,
adjusted by match weights and IPCW, evaluated the risk of clinical
deficit in each outcome following PME.
"Results: Of the 2804 children in this cohort, 285 (10.2%) had PME.
After optimal full matching and IPCW, exposed children scored
similarly on CELF Total (-0.33 points, 95% confidence interval [CI]
-4.71, 4.05), Receptive (+0.65 points, 95% CI -4.08, 5.38) or
Expressive (-0.53 points, 95% CI -5.07, 4.02). PME was not associated
with secondary outcomes or risks of clinical deficit in any
neuropsychological assessments.
"Conclusions: After adjusting for sociodemographic and clinical
covariates, PME was not associated with worse neuropsychological test
scores at age 10 or autistic traits at 19-20."
https://pubmed.ncbi.nlm.nih.gov/37283466/
[2713]
NIJZ (2017) had some information about ADHD, but about ADHD in
Slovenia not so much.
"Various epidemiological studies have found that for the primary
school population, the prevalence ranges from 2.4% to 19.8%. A recent
meta-study on 175 different prevalence studies carried out over the
last 36 years estimated the prevalence of hyperkinetic disorder at
7.2%. The disorder is more common in boys, with a sex ratio of 3-4:1.
It should be pointed out that the impact of sex is not yet fully
understood and that the sex ratio almost evens out in adulthood.
"In Slovenia, there are no data on prevalence and incidence, but
there are data on visits to GPs or specialist outpatient clinics for
hyperkinetic disorder, where an increase in the number of visits can
be observed in recent years."
The causes:
"The cause of the disorder is not yet fully understood and is likely
to be a combination of environmental and genetic risk factors, the
latter of which play a primary role:
"Genetic factors (family history of the disorder).
Neurophysiological factors (differences in the frontal regions of the
brain - reduced volume of the prefrontal cortex and reduced thickness
of the anterior cingulate cortex, as well as cortical thinning in both
upper frontal regions of the brain).
"Neurochemical factors (neurochemical peculiarities - in particular
in the action of neurotransmitters that affect executive functions and
cause excessive activity, distractibility or impulsivity - excessive
noradrenaline activity, dopamine deficiency).
"Psychosocial factors (stressful psychiatric events,
anxiety-provoking factors, the child's temperament, emotional
deprivation and society's demands that behaviour be adapted to the
environment)."
https://web.archive.org/web/20220519122733/https://www.nijz.si/sl/bi-prepoznali-hiperkineticno-motnjo
[1883]
Dopamine was first identified in 1910 as an intermediary in the
synthesis of adrenaline and noradrenaline.
https://physoc.onlinelibrary.wiley.com/doi/epdf/10.1113/jphysiol.1910.sp001392
[2200]
It was not until 1957 that it was found in the brains of several
species including humans, and in the following years:
"...studies on the mechanisms of the first-generation of
antipsychiatric drugs, pioneered by Arvid Carlsson, identified
dopamine as a neurotransmitter playing a role in motor and mental
functions. In parallel, Oleh Hornykiewicz and others found that
dopamine plays a critical role in movement regulation in Parkinson
disease. Finally, while studying the mechanisms of slow
neurotransmission, Paul Greengard and others revealed how dopamine
acts on dopamine receptors, activates downstream signalling pathways,
and modulates neuronal activity and synaptic plasticity." [2199]
So here, for instance, we see work on the effects of drugs on
adrenalin and noradrenaline steaming ahead in 1954, with not a mention
of dopamine, which had been so named in 1952. It is there, though,
lurking in the "total amines", for example in Table 15.
More than a quarter of a century after the Opium Conference,
dopamine's roles in motor control, modulation of behavior and
cognition, motivation and reward, inhibition of prolactin production,
sleep, dreaming, mood, attention, working memory, and learning was as
yet unknown. [2205]
But in Table 9 we can see that cats on caffeine had hypothalamic
noradrenaline 109% of the control's. In cats on insulin it was 66.6%
of the normal value, while morphine hydrochloride produced 56.6% of
the control or lower.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1366219/pdf/jphysiol01416-0041.pdf
[2202]
In 1957 came the recognition of dopamine as a neurotransmitter:
https://www.nature.com/articles/1801200a0.pdf
[2201].
As of 2022, dopamine unknowns included the
"...precise mechanisms and locations along the axons and dendrites
that dopamine is released, the structure and organization of dopamine
receptors, dopaminergic neuron subpopulations, their projections and
regulations, the role of glial cells in shaping dopamine functions,
the patterns of dopamine release at a single synapse, and across large
brain areas, and the time scale of dopamine modulation on intrinsic
neuronal excitability and synaptic plasticity."
https://www.frontiersin.org/research-topics/27370/brain-dopaminergic-mechanisms
[2199]
Dopamine theory remains restless. In a 2023 paper in Nature
Neuroscience, as explained in Wired's article "Everyone Was Wrong
About Antipsychotics":
"[Northwestern University neuroscientist Jones] Parker shows that an
assumption about antipsychotics thats almost as old as the drugs
themselves is . well, wrong.
"Neuroscientists have long thought that antipsychotics dampen extreme
dopamine transmission by sticking to receptors in a type of cell
called spiny projection neurons, or SPNs. The drugs basically box out
the dopamine at receptor proteins called D1 or D2 (where 'D' stands
for dopamine). Each of the spiny neurons sport either D1 or D2theyre
genetically distinct. Experiments on calf brain extracts in the 1970s
showed that the most powerful antipsychotics are the ones that cling
strongly to the D2 SPNs in particular, so decades worth of
antipsychotics were designed and refined with D2 in mind.
"But when Parkers team probed how four antipsychotics affect D1, D2,
and mouse behavior, they found that the most drug interaction is
actually happening at D1 neurons."
By using 2g microscopes to peer into living mouse brains via a tiny
endoscope, Parker was able to study a model of amphetamine psychosis
and the effect of haloperidol, olanzapine, clozapine and a failed drug
candidate MP-10.
"The notion that D1 receptors may be a more important target upends
decades of research in a $15 billion market for drugs that are
famously erratic. Antipsychotics dont work for about 30 percent of
people who try them. Theyre plagued by side effects, from extreme
lethargy to unwanted facial movements, and rarely address the
cognitive symptoms of psychosis, like social withdrawal and poor
working memory."
Parker's next plan is to see what happens with D1 partial
agonists.
"The drugs compensate for high dopamine and low dopamine. Its a
different approach than just blocking dopamine altogether, and Parker
hopes his new results bode well for D1 partial agonists in particular.
Thats because despite having more dopamine in their striatum, people
with schizophrenia actually have lower dopamine levels in their
cortex, a feature that neuroscientists think contributes to social
withdrawal and forgetfulness. 'Such a drug could be both antipsychotic
and cognition-promoting,' Parker says. His lab has begun testing
candidates."
https://www.wired.com/story/everyone-was-wrong-about-antipsychotics/?utm_medium=social&utm_source=twitter&utm_brand=wired-science&mbid=social_tw_sci&utm_social-type=owned
[2875]
https://www.nature.com/articles/s41593-023-01390-9
[2876]
Were it not for those pesky patents, Parker would not need to look
very far, as describing their work which "mark[ed] the first
demonstration of partial agonist/antagonist effects of THC in vivo" in
2012, Paronis et al, over at Northeastern University in Boston, Mass.,
explain:
"The designation of a drug as a full or a partial agonist is always
related to the effects of other drugs in that pharmacological class on
the variable being measured. Thus, although we find that THC is a
partial agonist in producing hypothermia in mice, it must still be
considered a full agonist under conditions in which it produces the
maximum possible effect, including antinociception, decreased
locomotor activity, and THC discrimination (Compton et al., 1992; Fan
et al., 1994; McMahon and Koek, 2007; Ginsburg et al., 2012). Some
studies have used the strategy of decreasing the number of available
receptors to rank the relative efficacy of opioid drugs that have full
agonist effects in vivo (Adams et al., 1990; Paronis and Holtzman,
1992). A similar approach has been used to define THC as a partial
agonist indirectly, insofar as it shows greater tolerance than other
cannabinoid agonists in vivo (Hruba et al., 2012). Our results extend
these findings by indicating that acute administration of THC has
partial agonist and antagonist effects in otherwise drug-naive
animals. Insofar as the apparent partial or full agonist effects of
drugs reflect their intrinsic properties, it seems likely that THC in
vivo has lower efficacy than AM2389 and, as has been shown in vitro,
other cannabinoid agonists."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3697741/
[2877]
In 2023 an international collaboration
"...compared the shared genetic risk and biological foundations of
neurological and mental illnesses using roughly one million cases from
genome-wide association studies (GWAS)."
"Psychiatric disorders were more polygenic than neurological
disorders, with pediatric-onset disorders having the highest single
nucleotide polymorphism (SNP) heritability. The finding supported the
hypothesis that multiple causal pathways may converge on the same
mental illness while fewer causal pathways may underlie neurological
disorders.
"The estimated polygenicity for psychiatric diseases and COG [general
cognitive ability] was greater than that for neurological diseases,
somatic disorders, cortical imaging evaluations, and height. Most
polygenic phenotypes had low discoverability, indicative of a higher
proportion of trait-affecting variants with smaller effect
sizes.
"The study found that 40 of 45 genetic correlations among psychiatric
disorders and 12 of 45 correlations among neurological disorders
reached significance."
https://www.news-medical.net/news/20230801/Research-reveals-surprising-genetic-overlap-between-neurological-and-psychiatric-disorders.aspx
[2878]
https://www.medrxiv.org/content/medrxiv/early/2023/07/23/2023.07.21.23292993.full.pdf
[2879]
A 2020 review of ADHD studies points to a strong genetic link.
"The formal heritability of ADHD is about 80%."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7046577/
[1890]
Do you think ADHD [known as HKM in Slovene] is associated with
criminal behaviour?
PsychCentral.com has some ideas about why people with ADHD might
lie:
"Impulsivity often plays a role in why people with ADHD lie.
"Sam Goldstein, PhD, a licensed psychologist in Utah, explains people
with ADHD have a tendency to act without thinking first while under
stress (impulsive behavior).
'This alone [may] lead to an increased probability that an impulsive
person may lie to avoid responsibility or manipulate others to achieve
a goal,' Goldstein says.
"Still, he clarifies that 'theres limited, if any, scientific
evidence that ADHD itself drives deceitful behavior. However, combined
with other personality and mental health challenges may lead to an
increased risk of lying.'
"Some people with ADHD may develop a habit of lying, which, for some,
could be a form of compulsive lying.
"Although lying can be a disruptive behavior, white lies can often be
harmless in nature. For example, difficulty staying focused during a
conversation can lead to someone lying to pretend like they were
listening to not hurt someones feelings.
"People with ADHD with a poor memory might also forget something that
happened, then say it didnt when it actually did. To the other person
in the conversation, this may appear as lying.
"Some other reasons why adults or kids with ADHD may lie may
include:
"covering up an impulsive behavior that resulted in an unwanted
consequence forgetting what happened and lying to pretend like they
remember responding impulsively with a lie due to hyperactivity hiding
a lack of understanding of something with a lie wrongly answering
questions they didnt listen to because they were distracted telling
white lies out of difficulty expressing themselves impulsively making
promises they cant keep Challenges with executive functions can also
make it harder for people with ADHD to process information or speak
and listen clearly. This could lead to miscommunications, which may
wrongly be considered lies."
https://psychcentral.com/adhd/adhd-and-lying#explanation
[1882]
According to "The Relationship between Adult Symptoms of
Attention-Deficit/Hyperactivity Disorder and Criminogenic Cognitions"
(2019) by Englehardt et al
"The relationship between ADHD in particular hyperactivity and
criminal behavior is well documented."
and
"The first multiple regression examined whether the factor-derived
subscales predicted total criminogenic cognitions. The overall model
was significant F(4,187) = 52.13, p < 0.001. The R2 was 0.53, and
age, gender, inattention/memory problems, and impulsivity/emotional
lability were all retained as predictors (see Table 4). As predicted,
higher age and being female were negatively related to criminogenic
cognitions, and the factor-derived subscales were positively related
to criminogenic cognitions. However, contrary to expectations,
inattention/memory problems was more strongly associated with
criminogenic cognitions than was impulsivity/emotional
lability."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6627881/
[1879]
120 years after Dr Still's lecture, instead of measuring big heads,
we now measure small brains.
According to "Subcortical brain volume differences in participants
with attention deficit hyperactivity disorder in children and adults:
a cross-sectional mega-analysis" by Hoogman et al, and published in
the Lancet (2017):
"Our sample comprised 1713 participants with ADHD and 1529 controls
from 23 sites with a median age of 14 years (range 463 years). The
volumes of the accumbens (Cohen's d=−015), amygdala
(d=−019), caudate (d=−011), hippocampus (d=−011),
putamen (d=−014), and intracranial volume (d=−010) were
smaller in individuals with ADHD compared with controls in the
mega-analysis. There was no difference in volume size in the pallidum
(p=095) and thalamus (p=039) between people with ADHD and controls.
Exploratory lifespan modelling suggested a delay of maturation and a
delay of degeneration, as effect sizes were highest in most subgroups
of children (<15 years) versus adults (>21 years): in the
accumbens (Cohen's d=−019 vs −010), amygdala (d=−018
vs −014), caudate (d=−013 vs −007), hippocampus
(d=−012 vs −006), putamen (d=−018 vs −008),
and intracranial volume (d=−014 vs 001). There was no difference
between children and adults for the pallidum (p=079) or thalamus
(p=089). Case-control differences in adults were non-significant (all
p>003). Psychostimulant medication use (all p>015) or symptom
scores (all p>002) did not influence results, nor did the presence
of comorbid psychiatric disorders (all p>05)."
Their interpretation of these and other results:
"With the largest dataset to date, we add new knowledge about
bilateral amygdala, accumbens, and hippocampus reductions in ADHD. We
extend the brain maturation delay theory for ADHD to include
subcortical structures and refute medication effects on brain volume
suggested by earlier meta-analyses. Lifespan analyses suggest that, in
the absence of well powered longitudinal studies, the ENIGMA
cross-sectional sample across six decades of ages provides a means to
generate hypotheses about lifespan trajectories in brain
phenotypes."
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(17)30049-4/fulltext
[1880]
What do the diagnosed ADHD cases, with their apparently permanently
misdeveloped brains, think about the utility of cannabis?
In "'I Use Weed for My ADHD': A Qualitative Analysis of Online Forum
Discussions on Cannabis Use and ADHD" Mitchell et al in North Carolina
examined 268 online forum threads. 20% were then randomly selected.
This 20% was then whittled down for various reasons, leaving 46
threads containing 880 individual posts of which 401
"Twenty-five (25%) percent of individual posts indicated that
cannabis is therapeutic for ADHD, as opposed to 8% that it is harmful,
5% that it is both therapeutic and harmful, and 2% that it has no
effect on ADHD. This pattern was generally consistent when the year of
each post was considered. The greater endorsement of therapeutic
versus harmful effects of cannabis did not generalize to mood, other
(non-ADHD) psychiatric conditions, or overall domains of daily life.
Additional themes emerged (e.g., cannabis being considered sanctioned
by healthcare providers)."
Co-author Dr Kollins
"...has received research support and/or consulting fees from the
following: Akili Interactive, Alcobra, Arbor, Atentiv, Ironshore,
Neos, NIH, Neurovance, Purdue, Rhodes, Shire, Sunovion, and Tris in
the past 2 years. This does not alter the authors adherence to PLOS
ONE policies on sharing data and materials. None of the other authors
have any additional declarations."
Here comes the "cannabis use disorder"...
"In the largest meta-analysis to date examining the prospective
association of ADHD with cannabis use, ADHD youth were nearly three
times as likely to report cannabis use in later life compared to
non-ADHD youth; and ADHD children were more than 1.5 times as likely
to be subsequently diagnosed with a CUD."
Well of course they are, because they are at the very least 1.5 times
more likely to come into contact with social workers who believe in
"cannabis use disorder". They are more likely to be in the justice or
mental health systems which take a criminal rather than a health-based
perspective. All these people would be very disappointed if cannabis
turned out to be a net positive. Their ignorance is motivated. This
study does not consider these effects on the prevalence - it's sole
purpose is to analyse the fora.
The authors find
"...that at least three times as many comments advocated for
therapeutic effects of cannabis on ADHD compared to comments that
cannabis is harmful, both therapeutic and harmful, or has no effect on
ADHD."
The authors do not mention placebo effect specifically, but do
admit:
"...no inferences can be drawn about the prevalence of perceptions
regarding the effects of cannabis on ADHD in patients with the
disorderthat was beyond the scope of the present study (i.e., to
assess the content of online data referring to cannabis and ADHD in
forums)."
https://journals.plos.org/plosone/article/file?id=10.1371/journal.pone.0156614&type=printable
[1181]
Perhaps the reason cannabis and ADHD is not such a popular area for
hard science lies, again, in the desires of the competitors - makers
of Ritalin and a panoply of other ADHD drugs. A study of patients with
medical cannabis and ADHD diagnoses, 70% with other mental health
conditions, concluded:
"Although MC is not directly indicated for ADHD, low ADHD symptom
frequency and ADHD medication-sparing effects were found to be
associated with MC treatment. In addition, high dosage of CBN was
associated with lower ASRS [ADHD self-report scale], hinting at a
possible combination effect in whole-plant MC treatment. Nevertheless,
although we found the abovementioned association with CBN, it is
minorly expressed in most MC cultivars, thus, we assume that other
phyto-cannabinoids might be more essential for the effect on ADHD
patients."
https://www.rmmj.org.il/userimages/1036/1/PublishFiles/1038Article.pdf
[1884]
Aleksi Hupli of the Tampere University in Finland presents a case
report in which an ADHD patient had gastric problems with Ritalin and
alcohol, and having heard about a delta-9 THC product Bedrocan was
able to move the mountain in just six months:
"After receiving this confirmation that the legal framework supported
his right to access cannabinoids, the patient began to formally seek
Bedrocan as a substitute medication for methylphenidate. It was hoped
that cannabinoids would offer equivalent or better efficacy with more
tolerable adverse effects. After failing to find a Finnish
psychiatrist or neurologist with sufficient medical knowledge of CT,
the patient exercised his right to patient self-determination and
finally, in June 2010, visited the prescribing physician behind the
small European ADHD study in Germany. Afterwards, the patient returned
to Finland with prescriptions for standardized Bedrocan and Bediol
medicinal cannabis products.
"Upon arrival to Finland, the next challenge for the patient was to
find a suitable Finnish physician to validate the prescriptions for
the cannabinoid treatment model. It took him until October 2010
− a period of almost 4 months − to find a suitably
qualified neurologist who was prepared to endorse the treatment model.
At that time, the patient presented the prescribing neurologist with a
challenge: no Finnish neurologist or psychiatrist had previously
substituted Bedrocan for short-acting methylphenidate as a
pharmacological intervention for a neuropsychiatric medical condition.
Clinical guidelines for adult ADHD were only introduced in Finland in
2017, updating pediatric treatment guidelines published in 2007, which
were updated for adolescents in 2013. These guidelines mention no
possibility of CT for either adult, adolescent, or pediatric ADHD.
However, the Bedrocan application was submitted to Fimea in late
November 2010 and approved by the end of December 2010."
Some other case reports are also presented.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8489316/
[3935]
In search of mechanisms which might explain the efficacy of cannabis
for some with ADHD, NIH neurophysiologists Lupica et al in "Marijuana
and cannabinoid regulation of brain reward circuits" (2009)
explain:
"Distinct physiological roles in which endocannabinoids act as
retrograde messengers have been described in several brain regions,
including the NAc and VTA (Robbe et al., 2002; Melis et al., 2004). In
this capacity, endocannabinoids that are released from postsynaptic
neurons upon depolarization activate presynaptic CB1 receptors and
inhibit neurotransmitter release. This suggests that the
endocannabinoid system may play additional important roles in the
regulation of ongoing synaptic brain function (Alger, 2002; Wilson
& Nicoll, 2002)."
The mechanisms elucidated by 2009 were:
"First, the ability of systemic cannabinoids to increase
extracellular DA concentrations in the NAc is reversed by systemic and
intra-VTA opioid antagonist administration (Chen et al., 1990; Tanda
et al., 1997), but the increase in DA neuron-firing rates caused by
Δ9-THC are not (French, 1997). Second, the direct infusion of
Δ9-THC into the VTA does not increase DA accumulation in the NAc
(Chen et al., 1993). Third, it has recently been demonstrated that
synthetic cannabinoid agonists and endocannabinoids, acting in a
retrograde manner, can also inhibit glutamate release onto neurons in
the VTA in vitro (Melis et al., 2004), which would tend to diminish
the excitatory input to DA neurons in the VTA and reduce the
probability of bursting (Johnson et al., 1992; Kitai et al., 1999).
Finally, preliminary data from our laboratory indicate that CB1
receptors are also located on GABAergic terminals believed to
originate from NAc medium spiny output neurons (Walaas & Fonnum,
1980; Heimer et al., 1991) that target GABAB receptors on DA neurons
in the VTA (Sugita et al., 1992), suggesting a second possible
disinhibitory mechanism (Riegel et al., 2003). This latter study,
taken together with that of Szabo et al. (2002), implies that
cannabinoids acting at CB1 receptors can inhibit the release of GABA
in the VTA that is derived from both intrinsic and extrinsic sources,
and further that the inputs from the NAc to the VTA may represent a
critical pathway for the expression of cannabinoid reward."
https://bpspubs.onlinelibrary.wiley.com/doi/full/10.1038/sj.bjp.0705931
[1885]
By 2009 Albayram et al felt able to declare with certainty that
"Mice lacking the Cnr1 gene (Cnr1−/−), which encodes the
cannabinoid receptor 1 (CB1), showed an accelerated age-dependent
deficit in spatial learning accompanied by a loss of principal neurons
in the hippocampus....The ongoing process of pyramidal cell
degeneration and neuroinflammation can exacerbate each other and both
contribute to the cognitive deficits. Deletion of CB1 receptors from
the forebrain GABAergic, but not from the glutamatergic neurons, led
to a similar neuronal loss and increased neuroinflammation in the
hippocampus as observed in animals lacking CB1 receptors in all cells.
Our results suggest that CB1 receptor activity on hippocampal
GABAergic neurons protects against age-dependent cognitive decline by
reducing pyramidal cell degeneration and neuroinflammation."
And that:
"During aging, an increase in the expression levels of proinflammatory
cytokines takes place in the brain. We detected a significant increase
in the expression of IL-6 in 12-moold Cnr1−/− mice,
whereas the expression of IL-1β, IL-6, or TNF did not differ
between 2-mo-old and 12-mo-old wild-type animals, in accordance with
previous reports. Changes in cell morphology and expression of surface
proteins and inflammatory cytokines have different dynamics and
onsets. Elevation of IL-6 levels has consistently been related to
aging, and high levels of IL-6 are associated with an increased risk
of cognitive decline. The fact that IL-6 but not IL-1β or TNF
expression is increased suggests that the increase in IL-6 expression
is one of the first steps in the gradual activation of microglial
cells."
https://www.pnas.org/doi/full/10.1073/pnas.1016442108
[5404]
Obviously, back in 2009, these authors were stuck in an anti-cannabis
mindset.
This has modified over the years. In 2022, to gauge attitudes of
perceived risk, Jack T Waddell of Arizona State University looked at
the trend:
"Public access data from the National Study on Drug Use and Health
from 2002 to 2019 were used (N = 1,005,421). Structural Equation
Models tested whether study year (linear trend), was associated with
alcohol- and cannabis-related risk perceptions (correlated outcomes),
and whether age (adolescence [12-17], emerging adulthood [18-25],
adulthood [26-35], middle adulthood [36-49], and older adulthood
[50+]) moderated time trends. Sex, race/ethnicity, and use frequency
were covaried.
"Results: The linear trend of study year was associated with
decreased cannabis-related risk perceptions (p < .001). There was
also a significant interaction of age by study year for
cannabis-related risk perceptions, such that adults, emerging adults,
and middle adults had the largest decrease in attitudes over time. For
alcohol-related risk perceptions, the linear trend of study year was
significantly associated with increased risk perceptions (p = .001),
but the interaction of time by age was non-significant;
alcohol-related effects were extremely small (b < 0.01)."
Mysteriously, Waddell concludes:
"Findings underscore the importance of targeting permissive
cannabis-related attitudes via prevention efforts."
But he doesn't say why all these people's perceptions are wrong, or
why he thinks his perception is better than all of theirs, or why he
thinks 18-49 year olds are particularly wrong.
https://pubmed.ncbi.nlm.nih.gov/34461500/
[1886]
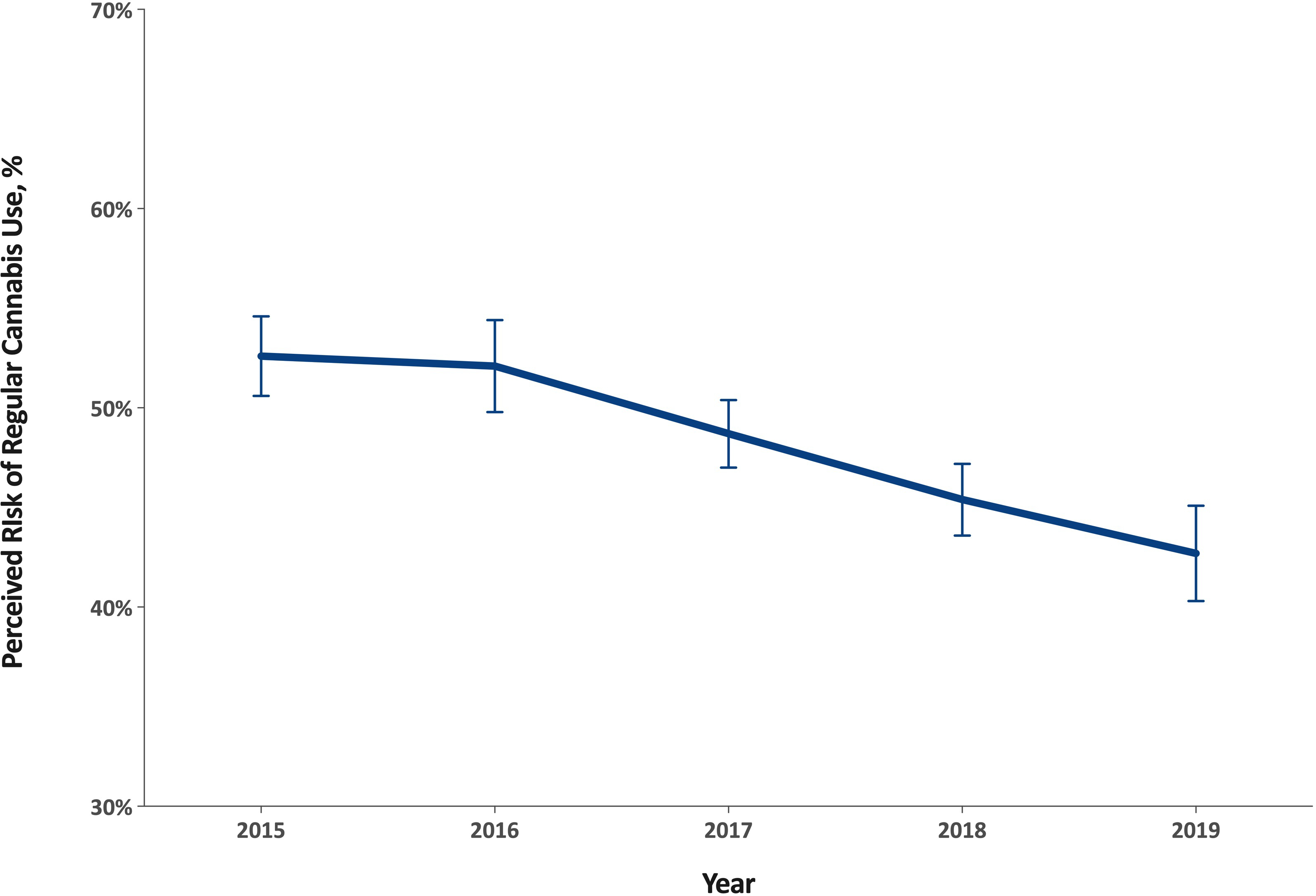
Another study of risk perception around cannabis enrolled 18,794
adults age ≥65 years participating in the 20152019 National Survey
on Drug Use and Health, a cross-sectional nationally representative
survey of non-institutionalized individuals in the U.S.
"Between 2015 and 2019, perceived risk associated with regular use
decreased from 52.6% to 42.7%, an 18.8% decrease (p<0.001).
Decreases in perceived risk were detected in particular among those
never married (a 32.6% decrease), those who binge drink (a 31.3%
decrease), use tobacco (a 26.8% decrease), have kidney disease (a
32.1% decrease), asthma (a 31.7% decrease), heart disease (a 16.5%
decrease), chronic obstructive pulmonary disease (a 21.5% decrease),
two or more chronic conditions (a 20.2% decrease), and among those
reporting past-year emergency department use (a 21.0% decrease)
(ps<0.05)."
The authors note:
"The increase in interest for cannabis use as a therapeutic drug for
a variety of health conditions and its decrease in stigma likely helps
explain the drop in perceived risk among older adults."
and most tellingly about knowability as a problem for the sheep-like
mentality upon which prohibition depends:
"We also found a larger decrease in risk perception in states where
cannabis is legal compared to states where it is not."
A moment's reflection will reveal to the curious onlooker that the
legal status of cannabis and the sum of the physical harms and
benefits are independent variables: there is no mechanism whereby
cannabis could affect ADHD or insulin or PPAR-gamma or melanoma rates
as a function of the law. The only harm which could arise as a
dependent variable of the legal status of cannabis is harm caused by
prohibition itself. Yet prohibition would like to arrange matters such
that it does not have to address health issues at all, preferring to
operate via innuendo and folk psychology
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8440375/
[1887]
So in relation to ADHD and cannabis, we have learned at least three
things: ADHD brain damage is irreparable, endocannabinoid mechanisms
are involved in the function of the VTA, and more patients think it
makes them think better than think the opposite.
In relation to cannabis safety generally, we have learned along the
way that large shifts in opinion towards cannabis are found in people
with no motivation to add to their health difficulties, and finally
that researchers in this area don't like this and are biased against
cannabis generally for no reason they care to explain.
"The global ADHD therapeutics market size is estimated to be worth
USD 29.56 billion in 2022 and USD 45.68 billion by 2027."
Besides COVID, which has boosted ADHD symptoms,
"The growing incidence of ADHD due to rough impact of unstable
lifestyles and additives in childrens diet across the world is
fundamentally driving the market growth as there is no treatment to
for this disorder."
https://www.marketdataforecast.com/market-reports/attention-deficit-hyperactivity-disorder-therapeutics-market
[1891]
My impression is Europe has nothing like the cornucopia of drug
choices available to American homo sapiens.
https://www.medicalnewstoday.com/articles/325201#medication-list
[1892]
The prohibition narrative grinds on, as in Huang and Lupica (2019)
whose glass half-empty view is that
"...chronic Δ9-THC shifts the strength of glutamatergic
activation of NAc from cortical to sub-cortical limbic sites, and we
hypothesize that this contributes to deleterious effects of cannabis
in humans."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7002212/
[1893]
Yet isn't this exactly what is claimed for Europe's ADHD drug of
choice Ritalin - methylphenidate hydrochloride?
https://pure.mpg.de/rest/items/item_1835660/component/file_1835659/content
[1894]
It turns out to be connected with the reason some people like
marijuana and some don't.
Rodents don't like THC, and why this should be is all about this
reward system.
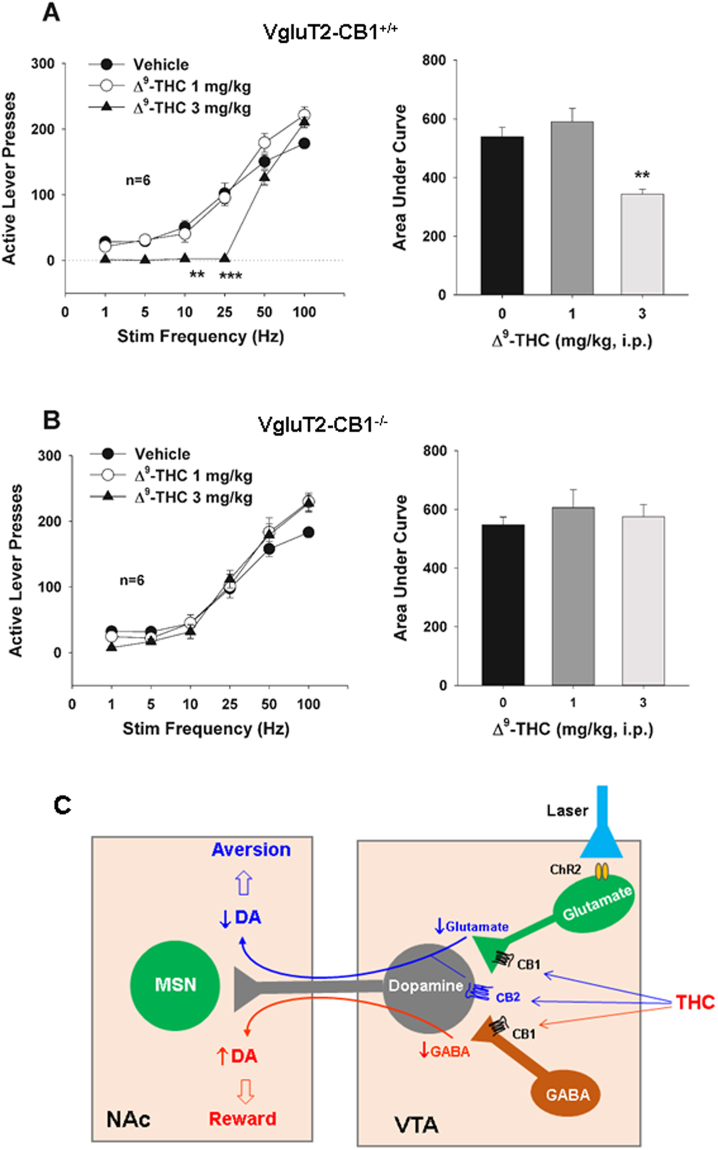
Thanks to Han et al (2017) who in "CB1 Receptor Activation on
VgluT2-Expressing Glutamatergic Neurons Underlies
Δ9-Tetrahydrocannabinol (Δ9-THC)-Induced Aversive Effects
in Mice" attest that:
"Δ9-tetrahydrocannabinol (Δ9-THC), the major psychoactive
component of cannabis, produced dose-dependent conditioned place
aversion and a reduction in the above optical ICSS [intra cranial self
stimulation] in VgluT2-cre control mice, but not in VgluT2-CB1
−/− mice. These findings suggest that activation of CB1Rs
in VgluT2-expressing glutamate neurons produces aversive effects that
might explain why cannabinoid is not rewarding in rodents and might
also account for individual differences in the hedonic effects of
cannabis in humans."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5614984/
[1896]
"The IRPBeijing study, together with other evidence, suggests that
THC will be experienced as pleasurable or otherwise depending largely
on its net effect on two sets of neurons (see Figure 2). In addition
to glutamatergic neurons, the VTA is also home to neurons that release
the neurotransmitter gamma-aminobutyric acid (GABA). Previous studies
have demonstrated that these two types of neurons exert opposite
effects on VTA dopamine-releasing neurons. Whereas glutamatergic
neurons stimulate the dopaminergic neurons to release dopamine into
the brains reward center, GABA-ergic neurons inhibit them.
Consequently, THC inhibition of VTA glutamate neurons indirectly
reduces dopamine activity in the reward center, leading to aversion,
and THC inhibition of GABA-ergic neurons increases dopamine activity,
producing euphoria.
"In the rodent VTA, the researchers note, glutamatergic neurons
produce more CB1 mRNA, and thus more CB1 receptors, than do GABA-ergic
neurons. Hence, when the rodent VTA is exposed to THC, the drugs
inhibition of CB1 in glutamatergic neurons predominates, producing
primarily aversive effects. In the human VTA, in contrast, CB1 levels
may be more similar in glutamatergic and GABA-ergic neurons. As a
result, when a person is exposed to THC, the experience can be
rewarding, aversive, or neutral."
https://nida.nih.gov/news-events/nida-notes/2018/03/why-marijuana-displeases
[1895]
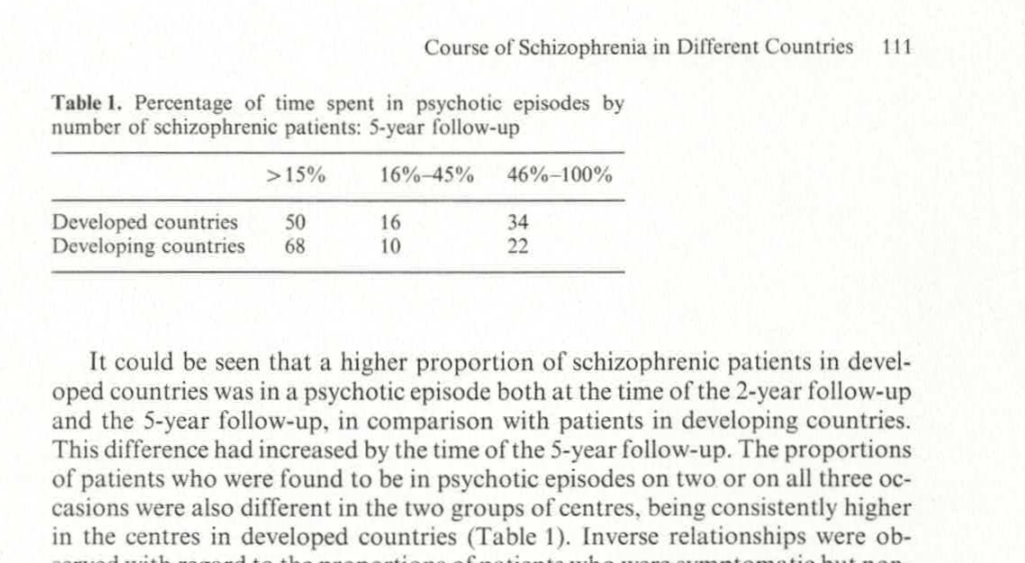
An unpopular association was obtained by "Course of Schizophrenia in
Different Countries" (1987):
https://www.researchgate.net/publication/284638496_Course_of_Schizophrenia_in_Different_Countries_Some_Results_of_a_WHO_International_Comparative_5-Year_Follow-up_Study/link/588f03aca6fdcc8e63cbb90a/download
[4177]
...while Saha et al (2007) add:
"The prevalence of schizophrenia in migrants was higher compared to
native-born individuals: the migrant-to-native-born ratio median
(10%-90% quantile) was 1.8 (0.9-6.4). When sites were grouped by
economic status, prevalence estimates from "least developed" countries
were significantly lower than those from both "emerging" and
"developed" sites (p = 0.04). Studies that scored higher on a quality
score had significantly higher prevalence estimates (p = 0.02)."
https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.0020141
[4178]
And now...brain volumes and schizophrenia.
For the psychiatrists of Bergen, there was simply no explanation.
"Paradoxically," they say, "most neurocognitive studies on
schizophrenia have shown cannabis use to be a marker of superior
performance on neuropsychological tests."
Why is it paradoxical? Experimenter bias?
"A systematic literature review revealed better cognitive functioning
in cannabis-using compared to non-cannabis-using patients in a
majority of the reviewed 23 studies (Lberg and Hugdahl, 2009). This
pattern has been replicated by later studies (DeRosse et al., 2010;
Rodriguez-Sanchez et al., 2010), also including two meta-analyses
(Rabin et al., 2011; Yucel et al., 2012)."
It's all very worrying for the anti-cannabis dogma, as:
"Studies comparing schizophrenia patients with and without cannabis
use by means of structural MRI and diffusion tensor imaging (DTI) have
shown more normalized (Dekker et al., 2010), more anomalous (Szeszko
et al., 2007; Bangalore et al., 2008; Rais et al., 2008; Ashtari et
al., 2011; Ho et al., 2011; James et al., 2011; Solowij et al., 2011),
and equivalent (Block et al., 2000; Cahn et al., 2004; Wobrock et al.,
2009; Cohen et al., 2012) brain anatomy in the cannabis group, thus
making firm conclusions difficult also when it comes to structural
imaging."
In their own test on 26 schizophrenics with and without previous
cannabis use (but not current use), Lberg et al found
"...the Can+ group showed increased activation in the task-present
condition and decreased activation in the default mode network in the
absence of the task as compared to the Can− group."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3483569/
[1923]
Cannabis schizophrenics had more insight and fewer abusive or
accusatory hallucinations:
"We used a case register that contained 757 cases of first onset
schizophrenia, 182 (24%) of whom had used cannabis in the year prior
to first presentation, 552 (73%) had not and 3% had missing data. We
completed the OPCRIT [Operational Criteria Checklist for Psychotic
Illness] checklist on all patients and investigated differences in the
proportion of people with distractibility, bizarre behaviour, positive
formal thought disorder, delusions of reference, well organised
delusions, any first rank symptom, persecutory delusions,
abusive/accusatory hallucinations, blunted affect, negative thought
disorder, any negative symptoms (catatonia, blunted affect, negative
thought disorder, or deterioration), lack of insight, suicidal
ideation and a positive family history of schizophrenia, using chi
square tests. Logistic regression modelling was then used to determine
whether prior cannabis use affected the presence of the
characteristics after controlling for age, sex and ethnicity.
"There was no statistically significant effect of cannabis use on the
presence of any of the above. There remained however a non-significant
trend towards more insight (OR 0.65 p = 0.055 for 'loss of insight')
and a finding of fewer abusive or accusatory hallucinations (OR 0.65 p
= 0.049) of borderline significance amongst the cannabis users. These
were in the hypothesised direction. There was no evidence of fewer
negative symptoms or greater family history amongst cannabis
users."
https://www.sciencedirect.com/science/article/abs/pii/S0920996407001508?via%3Dihub
[1924]
Ibarra-Lecue et al (2021) believe:
"The most accepted theory is that daily use of highpotency varieties
of cannabis may trigger the onset of schizophrenia in vulnerable
individuals."
So their own findings have a special way of describing unwanted
results:
"The aim of the present study was to evaluate 5-HT2AR protein
expression and the Akt functional status in platelet homogenates of
subjects diagnosed with schizophrenia, cannabis use disorder, or both
conditions, compared with age- and sex-matched control subjects.
Additionally, endocannabinoids and pro-inflammatory interleukin-6
(IL-6) levels were also measured in the plasma of these subjects.
Results showed that both platelet 5-HT2AR and the active phospho
(Ser473)Akt protein expression were significantly increased in
schizophrenia subjects, whereas patients with a dual diagnosis of
schizophrenia and cannabis use disorder did not show significant
changes. Similarly, plasma concentrations of anandamide and other
lipid mediators such as PEA and DEA, as well as the pro-inflammatory
IL-6, were significantly increased in schizophrenia, but not in dual
subjects."
The authors have explained their position about cannabis woo woo.
This is a woo-woo way of saying:
"Platelet 5-HT2AR, active phospho (Ser473)Akt protein expression,
plasma concentrations of anandamide, PEA, DEA, and IL-6 were
significantly increased in schizophrenia subjects, unless they used
cannabis."
https://onlinelibrary.wiley.com/doi/pdf/10.1111/adb.13233
[1969]
Perhaps we should not be surprised about Akt, aso known as protein
kinase B, as Ozaita et al (2007) say:
"We report that THC acute administration (10 mg/kg, i.p.) increases
the phosphorylation of Akt in mouse hippocampus, striatum, and
cerebellum. This phosphorylation was mediated by CB1 receptors as it
was blocked by the selective CB1 antagonist rimonabant."
and
"In conclusion, the present results demonstrate for the first time in
vivo that an exogenous cannabinoid, such as THC, activates the
neural-protective PI3K/Akt pathway and negatively regulates GSK-3b
activity in the mouse brain. These findings highlight the existence of
cannabinoid-induced activation of survival signaling pathways in the
brain, as previously reported in in vitro models. These molecular
events provide new insights for better understand the specific
mechanisms involved in the neuroprotective effects that have been
reported after the activation of CB1 receptors by cannabinoid
agonists."
and
"Several studies have shown that cannabinoids can protect neural
cells from different insults, such as glutamatergic excitotoxicity,
oxidative damage, traumatic injury, and ischemia (for review, see
Guzman 2005). Some of these effects are linked to the activation of
the PI3K/Akt pathway, which is closely involved in the survival
signaling in many cell types including neurons. Cannabinoids can
activate PI3K/Akt pathway by acting on both CB1 and CB2 receptors
(Sanchez et al. 2003), although the protective effects on primary
astrocytes (Gomez Del Pulgar et al. 2002) and oligodendrocytes
(Molina-Holgado et al. 2002) have been reported to involve CB1
receptor. The stimulation of the PI3K/Akt pathway is also required for
the neuroprotective effects of the synthetic cannabinoid HU-210 in
primary cortical neurons (Molina-Holgado et al. 2005)."
and
"We found a close regulation of Akt and GSK-3 phosphorylation by THC
in brain, acting on CB1 receptors, that could be related to the
neuroprotective effects induced by cannabinoids in insults such as
ischemia, glutamatergic excitotoxicity, mechanical trauma, and
oxidative damage through the modulation of these crucial components of
the cell survival pathway."
and
"Considerable evidence exists demonstrating that cannabinoids play a
role as neuroprotective agents by both receptordependent (reducing
Ca2+ conductances and excitability) and receptor-independent
mechanisms (anti-oxidative properties of cannabinoid compounds)
(reviewed in Sarne and Mechoulam 2005). The signaling events involved
in this beneficial action produced in vivo are largely unknown.
PI3K/Akt pathway promotes cell survival by both enhancing the
expression of anti-apoptotic proteins and inhibiting the activity of
pro-apoptotic ones. Direct intracellular targets of PI3K/Akt involved
in the control of apoptosis include Bad, caspase 9, transcription
factors of the Forkhead family, and GSK-3b (reviewed in Brunet et al.
2001). The ability of cannabinoids to activate the pro-survival
PI3K/Akt pathway has been reported in some in vitro studies and may
account for their protective role (Gomez Del Pulgar et al. 2002;
Molina-Holgado et al. 2002, 2005). Nevertheless, the signaling events
mediated by CB1-receptor stimulation in vivo remains poorly
understood. The results presented herein show that in vivo acute THC
administration in mice activated Akt by enhancing Ser473
phosphorylation in the hippocampus, cerebellum, striatum and, to a
minor extend, in the frontal cortex. This effect was common to all the
brain areas tested, supporting the idea that this signaling mechanism
is closely related to the activation of CB1 receptors in the brain.
The activation of Akt was dose dependent with a modest effect at 0.3
mg/kg of THC, reaching the maximum peak at 10 mg/kg. Therefore, the
dose of 10 mg/kg was used to characterize this signaling pathway in
vivo."
https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.1471-4159.2007.04642.x
[1970]
Peineau et al (2008) have a diagram
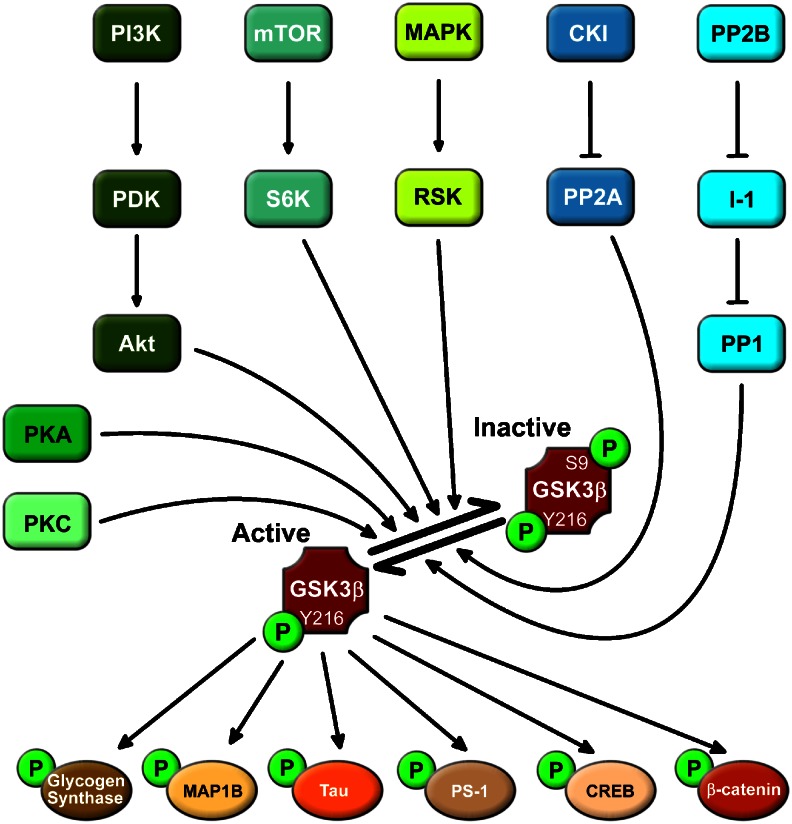
"Example of signalling pathways upstream and downstream of
GSK-3β. Under resting conditions, GSK-3β is basally
activated by phosphorylation at tyr216. Various ser/thr kinase
cascades result in phosphorylation of ser9 of GSK-3β, which
results in inhibition of its activity. Conversely, dephosphorylation
of this residue results in disinhibtion of the enzyme. GSK-3β
phosphorylates a wide range of substrates. A selection of such
substrates that relate to neuronal function is shown. CREB, cAMP
responsive element-binding protein; CK1, casein kinase 1; I-1,
inhibitor 1; MAP1B, microtubule-associated protein 1B; MAPK,
mitogen-activated protein kinase; mTOR, mammalian target of rapamycin;
PDK, phosphoinositide-dependent protein kinase; PI3K,
phosphatidylinositol 3-kinase; PP1, protein phosphatase 1; PP2A,
protein phosphatase 2A; PP2B, protein phosphatase 2B; PS-1, presenilin
1; RSK, p90 ribosomal S6 kinase; S6K, p70 ribosomal S6
kinase-1."
The authors have nothing to say about psychedelics, but in discuss
the link between GSK-3β and long term potentiation (LTP):
"Two independent studies have shown that following the induction of
LTP there is inhibition of GSK-3β (Hooper et al., 2007; Peineau
et al., 2007). This has been demonstrated following the induction of
LTP in vivo in both dentate gyrus and area CA1 in hippocampal slices
(Figure 5a). The inhibition of activity, assessed as an increase in
phosphorylation of ser9, was prominent 1020 min after the
induction of LTP and lasted for at least an hour. This link between
LTP and GSK-3β raises two questions. First, what influence
GSK-3β has on LTP and second, what role the LTP-induced
regulation of GSK-3β activity plays. With respect to the first
issue, it was shown that in a transgenic animal that overexpressed
GSK-3β, there was a pronounced inhibition of LTP (Figure 5b),
which could account for the learning deficits observed in these mice
(Hernandez et al., 2002). This deficit was restored by treatment with
lithium, suggesting that it was the overexpression of GSK-3β that
was responsible for the effect rather than some developmental
alteration (Hooper et al., 2007). Could GSK-3β, given that it is
constitutively active', be providing a tonic inhibition of LTP? In
which case, GSK-3β inhibitors would be expected to enhance LTP.
Quantitative comparisons of the effects of a range of GSK-3β
inhibitors on LTP will be required to address this issue."
https://pmc.ncbi.nlm.nih.gov/articles/PMC2268071/
[4938]
In 2013 Koriyama et al demonstrated the therapeutic role of
GSK-3β inhibition in neurodegenerative diseases with an
inflammatory component:
"Activated microglial cells play an important role in immune and
inflammatory responses in CNS and play a role in neurodegenerative
diseases. We examined the effects of lipoic acid (LA) on inflammatory
responses of BV-2 microglial cells activated by lipopolysaccharide
(LPS), and explored the underlying mechanisms of action of LA. BV-2
cells treated with LPS showed an up-regulation of mRNA of the
pro-inflammatory molecules, inducible nitric oxide synthase (iNOS). LA
suppressed the expression of iNOS and furthermore, LPS-induced
production of nitrite. Moreover, LA suppressed the nuclear
translocation of RelA, a component of nuclear factor-kappa B
(NF-κB) that contains transcriptional activator domain for LPS.
The mechanisms of LA-mediated anti-inflammatory effects on microglia
remain unknown, and we suggested an involvement of Akt/glycogen
synthase kinase-3β (GSK-3β) phosphorylation. The results
showed that inhibitor of phosphatidylinositol 3-kinase prevented
LA-mediated suppression of LPS induction of RelA and expression of
iNOS. Furthermore, these inflammatory actions were prevented by
GSK-3β inhibitors."
https://www.sciencedirect.com/science/article/abs/pii/S0168010213001788?via%3Dihub
[4939]
According to Hans O Kalkman (2023) of the Psychiatric University
Hospital, University of Zurich:
"Risk factors for depression initiate an infection-like inflammation
in the brain that involves activation [of] microglial Toll-like
receptors and glycogen synthase kinase-3β (GSK3β).
GSK3β activity alters the balance between two competing
transcription factors, the pro-inflammatory/pro-oxidative
transcription factor NFκB and the neuroprotective,
anti-inflammatory and anti-oxidative transcription factor NRF2. The
antidepressant activity of tricyclic antidepressants is assumed to
involve activation of GS-coupled microglial receptors, raising
intracellular cAMP levels and activation of protein kinase A (PKA).
PKA and similar kinases inhibit the enzyme activity of GSK3β.
Experimental antidepressant principles, including cannabinoid
receptor-2 activation, opioid μ receptor agonists, 5HT2 agonists,
valproate, ketamine and electrical stimulation of the Vagus nerve, all
activate microglial pathways that result in
GSK3β-inhibition."
https://www.mdpi.com/2227-9059/11/3/806
[4909]
In terms of convenience and safety, the Defendant rules out all
except the first of these as acceptable everyday experiences for the
purpose of inhibiting GSK3β - and adds a further example,
curcumin, per Bustanji et al (2008).
https://www.tandfonline.com/doi/10.1080/14756360802364377?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
[4910]
This shows cannabis belongs to a group of phytochemical sources
capable of inhibiting glycogen synthase kinase-3β. Yet curcumin
is not listed as a drug with no medical purposes, is not banned and,
notably, does not make the consumer notably happier. No other reason
for the distinction can be ascertained.
Back on the statistical battlefield, and using as the arbitrarily
defined criterion of inclusion that "cannabis-users had to either have
a diagnosis of cannabis use disorder or use cannabis at least twice a
week", along with "psychopathology of individuals with schizophrenia
spectrum disorders assessed by the Positive and Negative Syndrome
Scale (PANSS)", "Association between cannabis use and symptom
dimensions in schizophrenia spectrum disorders: an individual
participant data meta-analysis on 3053 individuals" by Argote et al
trawled the entire history of publications on the association up to
September 2022.
Despite all this effort, and completely ignoring the direction of
association issue - i.e. whether schizophrenics were more likely to
become cannabis users rather than the reverse - the findings were
unremarkable:
"Among the 1149 identified studies, 65 were eligible and 21 datasets
were shared, totaling 3677 IPD and 3053 complete cases. The adjusted
multivariate analysis revealed that relative to non-use, cannabis use
was associated with higher severity of positive dimension (3-factor:
Adjusted Mean Difference, aMD = 0.34, 95% Confidence Interval, CI =
[0.03; 0.66]; 5-factor: aMD = 0.38, 95% CI = [0.08; 0.63]), lower
severity of negative dimension (3-factor: aMD = −0.49, 95% CI
[−0.90; −0.09]; 5-factor: aMD = −0.50, 95% CI =
[−0.91; −0.08]), higher severity of excitement dimension
(aMD = 0.16, 95% CI = [0.03; 0.28]). No association was found between
cannabis use and disorganization (aMD = −0.13, 95% CI =
[−0.42; 0.17]) or depression (aMD = −0.14, 95% CI =
[−0.34; 0.06]). Interpretation No causal relationship can be
inferred from the current results. The findings could be in favor of
both a detrimental and beneficial effect of cannabis on positive and
negative symptoms, respectively. Longitudinal designs are needed to
understand the role of cannabis is this association. The reported
effect sizes are small and CIs are wide, the interpretation of
findings should be taken with caution."
Despite their literary adhesion to the
cannabis-increases-schizophrenia hypothesis, the results if anything
show an opposite trend, such that the authors are forced to admit that
despite their hopes
"...the lower severity of negative symptoms for cannabis-users cannot
be ignored. The presented results support both the selfmedication and
toxicity hypotheses of cannabis use, with differential effects on
positive and negative symptoms."
https://www.thelancet.com/pdfs/journals/eclinm/PIIS2589-5370(23)00376-0.pdf
[4267]
Let's take a look at fold counts. This is a measure of the
overexpression or underexpression of some gene compared to a baseline.
To produce easier to handle numbers, fold count (FC) is expressed as a
logarithm in base 2, so you will see logFC.
"Fold change is the number of times a gene is over-expressed (or
under), compared to some baseline (your control, or the reference
gene, etc.). A sample could be 100X more expressed, or 1/100th the
expression of the baseline. Because this is hard to show in a graph,
we plot in log. It "flattens" the data out to make it more
visible.
"Furthermore, because we tend to think of expression in terms of
copies of genes, or rather copies of copies of copies, we think of it
in terms of doubling which is why Log2 is frequently used to display
the data - you show the not the quantity, but the rounds of
amplification of it. to give better context between exponential
differences in gene expression.
"In the instance of 'no difference' between a sample and its
baseline, or logFC = 0, the fold change, or ratio of a sample and
control is one, or one-to-one.
"If a sample is expressed twice as much as the control (FC = 2), the
logFC = 1; one doubling of the gene compared to baseline.
"So, to answer your question: if logFC = -0.5, then FC = 2-0.5, or
0.7071, which means about 70% of the baseline, not 50%... 50%
reduction in expression would be a logFC of -1.
"if LogFC if 0.05, then your actual fold change is 1.0353... which is
effectively 1, or rather, no significant change.
"To convert a logFC value, simply use it as the exponent of two:
2logFC. In Excel, use the function "=2x". To convert a FC value, take
the log2. In Excel, use function: "=log(x,2). (where x = the cell with
your data)."
https://www.reddit.com/r/labrats/comments/7odtki/dumb_question_about_logfc/
[1897]
The relevance of this becomes clear when we look at "THC exposure of
human iPSC neurons impacts genes associated with neuropsychiatric
disorders" which the authors claim, in very controlled language, to
show
"significant alteration in THC-related genes associated with autism
and intellectual disability, suggesting shared molecular pathways
perturbed in neuropsychiatric disorders that are exacerbated by
THC."
Reading the text you would hardly guess that not all of these
alterations are of the type "more gene alteration equals more
schizophrenia and more autism and more intellectual disability".
Nothing could be further from the facts, the reality is far more
nuanced.
"There is a significant association between cannabis use and
schizophrenia in human subjects, however, whether this reflects
patient self-medication of prodromal symptoms or an environmental
modulation of genetic susceptibility remains an ongoing discussion. We
recently reported molecular abnormalities in schizophrenia patient
hiPSC-derived neurons in response to neural activity; here we describe
a distinct overlap in hypo-excitability, particularly in the glutamate
system, between schizophrenia patient-derived neurons and those
treated with THC. THC exposure seems to deregulate glutamate receptors
and other genes involved in synaptic function. We observe significant
THC-dependent changes in postsynaptic density, ion channel and WNT
[Wingless/Int1 Trail] pathway genes, and epigenetic regulators; and
molecular connections to autism and intellectual disability. Although
the molecular mechanisms may not be precisely the same, the
convergence of glutamatergic hypo-function may partially explain the
increased risk for psychiatric disorders amongst those exposed to
cannabis."
What do they mean by "not precisely the same"? It means the molecular
mechanisms are different.
"Relative to vehicle treatment, acute THC exposure resulted in 497
genes significantly altered in hiPSC- derived neurons compared to
untreated controls, while chronic THC exposure perturbed 810 genes
(Fig. 1a; Supplementary Table S3; Supplementary Figure 1)."
Let's take a look at Supplementary Table S3
https://static-content.springer.com/esm/art%3A10.1038%2Fs41398-018-0137-3/MediaObjects/41398_2018_137_MOESM4_ESM.pdf
[1898]
We can see logFCs for the "perturbed" genes - genes which are of
course perturbed not only by THC but by all sorts of things - and it
is easily observed that some are numbers above 0 and some are below 0.
The Court will recall that a logFC of 1 represents a doubling of
expression, a logFC of -0.5 is about 70% of the control value.
If we look at the authors' Figure 2a we can see the non-log fold
changes are almost all positive - in this case remember the no-change
value is 1. We don't necessarily know whether more or less of some
activation is a good thing or a bad thing, or for whom.
The authors have selected HOMER1 for their example in 2b, which is
the only lowered value among the postsynaptic density genes, for
"acute" THC, and one of only three out of 15 with a lowered fold count
in the "chronic" THC model.
2c shows postsynaptic density and ion channel genes plotted by
function but, again, there's nothing here showing anything more than
"perturbation" - we don't know if we want each of these perturbing, or
in which direction.
"Network analysis combining all THC-related genes from acute and
chronic THC treatment shows broad changes to fundamental cellular
functions such as RNA biology, chromatin regulation and
development."
In Figure 3 the perturbed genes are counted by association with THC
and the three disorders. Again this says nothing about positive or
negative influences per se, and a certain degree of tunnel vision is
already developing.
"We noticed that many genes implicated in psychiatric disease
coincided with genes altered in response to THC treatments. In order
to calculate statistical relevance we needed to first update the
numbers of genes associated with these disorders and found genes
related to autism spectrum disorder (1037 genes), intellectual
disability (2461 genes) and schizophrenia (723 genes; see
Supplementary Information Generation of Gene Databases for details;
Supplementary Table S7). Included in our list of significantly altered
transcripts following THC exposure is a substantial number of genes
linked to autism (80 genes) and intellectual disability (167 genes),
with fewer overlapping with schizophrenia (Fig. 3a); autism and
intellectual disability associated genes are significant for both
p-value and odds ratio using the Fishers exact test (Fig. 3b). These
data suggest that endogenous THC responsive pathways include many
psychiatric disease-associated genes and that changes in these genes,
either genetically or epigenetically, may contribute to
cannabis-related adverse reactions such as psychosis in some
users."
But the "suggestion" is not a valid statement - or at least
non-neutral - as the outcomes have not been shown to be universally
"adverse" at all. Indeed, although for intellectual disability and
autism the odds ratio for this association - not the disease - are 1.7
and 1.9 respectively, the odds for an association with schizophrenia -
not the disease - are less than unity - 0.9.
The association is between genes connected with THC good or bad and
genes connected with schizophrenia good or bad. It tells us nothing
about THC and schizophrenia...
The well-known gene for dopamine metabolism COMT is found in the
autism and schizophrenia lists at Supplementary Table 7, but not the
intellectual disability list.
https://static-content.springer.com/esm/art%3A10.1038%2Fs41398-018-0137-3/MediaObjects/41398_2018_137_MOESM8_ESM.pdf
All the "THC-related pathways" are also anandamide-related pathways.
As early as 1998 Adams et al the Medical College of Virginia
wrote:
"Anandamide is the newly discovered endogenous cannabinoid ligand
that binds to brain cannabinoid receptors and shares most, but not
all, of the pharmacological properties of delta 9-THC. Therefore, this
study was undertaken to determine whether its interaction with the CB1
receptor in brain was identical to that of delta 9-THC. Anandamide
depressed spontaneous activity and produced hypothermia,
antinociception and immobility in mice after i.v. administration.
However, none of these effects was blocked by pretreatment with the
selective CB1 antagonist, SR 141716A. However, the metabolically
stable analog 2-methyl-2'-fluoroethylanandamide produced reductions in
motor activity and antinociception in mice, effects that were blocked
by the antagonist. To determine whether anandamide's receptor binding
mimicked that of other cannabinoids, an autoradiographic comparison of
anandamide, SR 141716A and CP 55,940 competition for [3H]CP55,940
binding was conducted throughout rat brain. The receptor affinities
for all three compounds did not change according to brain area. As
expected, Bmax values differed dramatically among differ brain areas.
However, the Bmax values for each brain area were similar regardless
of the compound used for displacement. These data suggest that
anandamide, SR 141716A and CP 55,940 compete for the same cannabinoid
receptor throughout brain despite SR 141716A's failure to block
anandamide's pharmacological effects. Although there is no question
that anandamide binds to the cannabinoid receptor, failure of SR
141716A to block its pharmacological effects in mice poses a dilemma.
The results presented herein raise the possibility that anandamide may
not be producing all of its effects by a direct interaction with the
CB1 receptor."
https://pubmed.ncbi.nlm.nih.gov/9495885/
[1929]
As for the Jaccard Index
"The class also calculates the Jaccard index which measures the
similarity between two lists. The Jaccard index varies between 0 and
1, with 0 meaning there is no similarity between the two and 1 meaning
the two are identical."
The findings prove nothing for any individual case and are more aimed
at pharmaceutical research.
https://static-content.springer.com/esm/art%3A10.1038%2Fs41398-018-0137-3/MediaObjects/41398_2018_137_MOESM1_ESM.pdf
[1900]
Justin Jackson at medicalxpress.com writes:
"Debate continues regarding the nature of the association between
adolescent cannabis use and psychosis risk, with theories including
the contributing risk hypothesis, the shared vulnerability hypothesis,
and the self-medication hypothesis.
"In the contributing risk hypothesis, cannabis use causes the
emergence and progression of psychosis through disruption of the
neurodevelopmental processes during adolescence.
"According to the shared vulnerability hypothesis, genetic,
gestational, or environmental factors predispose individuals to both
cannabis use and psychosis. In this scenario, the likelihood of
engaging in cannabis use shares the same origin as the risk of
psychosis spectrum symptoms.
"The self-medication hypothesis suggests that individuals may turn to
cannabis use as a means to alleviate distressing symptoms associated
with the psychosis spectrum.
"Previous research has provided evidence supporting each of these
models, but there is a lack of prospective longitudinal studies
focusing on early adolescence.
"In a study, 'Psychosis Spectrum Symptoms Before and After Adolescent
Cannabis Use Initiation,' published online in JAMA Psychiatry, the
researchers analyzed psychosis spectrum symptom trajectories before
and after cannabis initiation in 11,868 adolescents aged 9 to 10 years
at baseline using data from five waves over four years from the
Adolescent Brain Cognitive Development (ABCD) Study.
"Cannabis initiation did not consistently lead to an increase in
psychosis symptoms, providing no significant support for the
contributing risk hypothesis.
"Adolescents who used cannabis at any point during the study period
reported a greater number of psychosis spectrum symptoms and more
distress compared to those who never used cannabis, supporting the
shared vulnerability hypothesis.
"An increase in the number of psychosis spectrum symptoms and
associated distress leading up to cannabis initiation was observed
before cannabis use started, aligning well with the self-medication
hypothesis.
"Based on the findings, the current research supports the shared
vulnerability and self-medication explanations for the associations
between cannabis use and psychosis risk."
https://medicalxpress.com/news/2024-11-psychosis-symptoms-adolescent-cannabis.html
[3709]
The study, "Psychosis Spectrum Symptoms Before and After Adolescent
Cannabis Use Initiation" by Osborne et al (2024) reports:
"Among the 11 858 participants at wave 1, the mean (SD) age was 9.5
(0.5) years; 6182 (52%) participants were male. Consistent with a
shared vulnerability hypothesis, adolescents who used cannabis at any
point during the study period reported a greater number of psychosis
spectrum symptoms (B, 0.86; 95% CI, 0.68-1.04) and more distress (B,
1.17; 95% CI, 0.96-1.39) from psychosis spectrum symptoms relative to
those who never used cannabis. Additionally, consistent with a
self-medication hypothesis, the number of psychosis spectrum symptoms
(B, 0.16; 95% CI, 0.12-0.20) and distress (B, 0.23; 95% CI, 0.21-0.26)
from psychosis spectrum symptoms increased in the time leading up to
cannabis initiation. We observed mixed evidence for an increase in
psychosis symptoms after cannabis initiation (ie, contributing risk
hypothesis)."
https://jamanetwork.com/journals/jamapsychiatry/article-abstract/2825423
[3710]
A case study demonstrates that:
"...in some cases people with ADHD may show unusual effects after the
consumption of THC. A 28-year-old male, who showed abnormal behaviour
and seemed to be significantly maladjusted and inattentive while
sober, appeared to be completely normal with a very high plasma level
of THC. Performance tests conducted with the test batteries ART2020
and TAP provided average and partly above-average results in functions
related to driving. Thus, it has to be taken into account that in
persons with ADHD THC may have atypical and even performance-enhancing
effects."
https://pubmed.ncbi.nlm.nih.gov/17879702/
[1903]
According to Aran et al at the Neuropediatric Unit, Shaare Zedek
Medical Center, Jerusalem, Israel (2019)
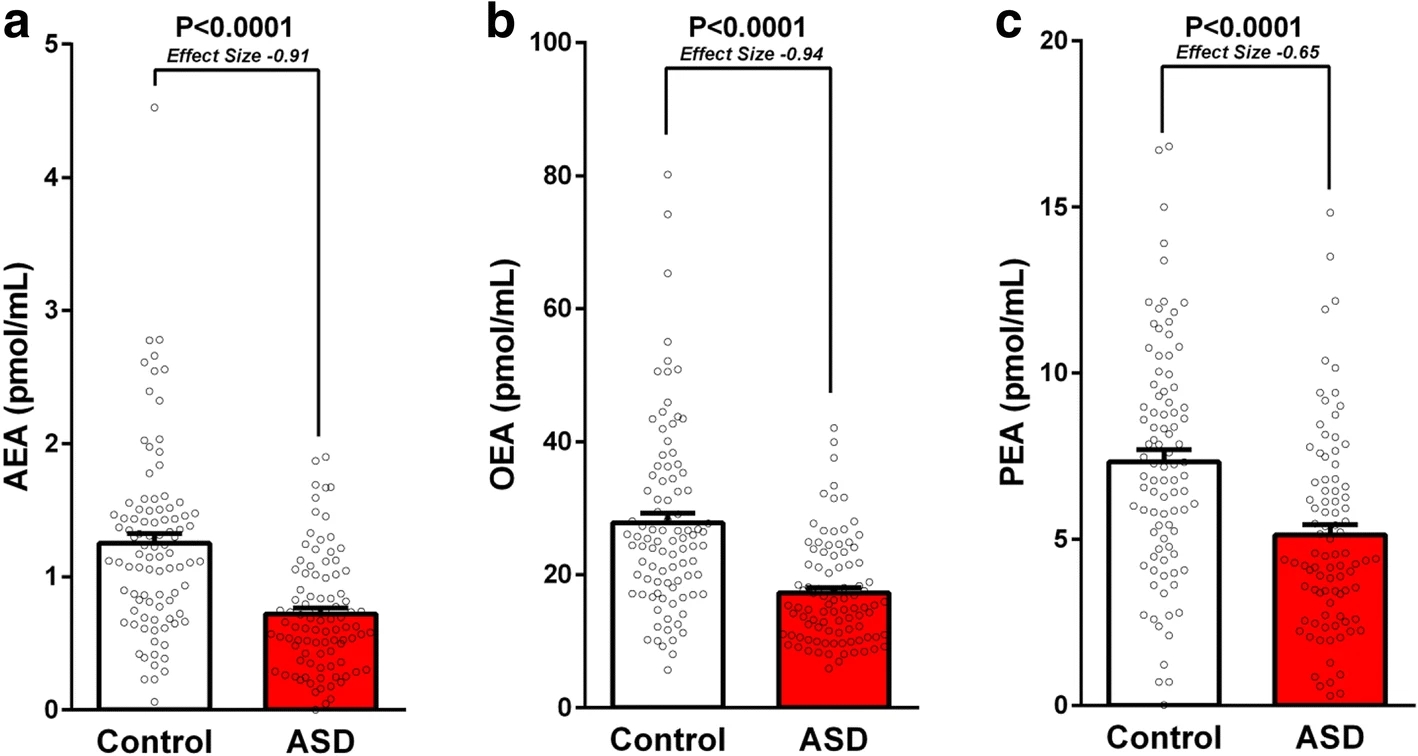
"Serum levels of the main endocannabinoids,
N-arachidonoylethanolamine (AEA or anandamide) and
2-arachidonoylglycerol (2-AG), and their related endogenous compounds,
arachidonic acid (AA), N-palmitoylethanolamine (PEA), and
N-oleoylethanolamine (OEA), were analyzed by liquid
chromatography/tandem mass spectrometry in 93 children with ASD
(age = 13.1 4.1, range 621; 79% boys) and
93 age- and gender-matched neurotypical children
(age = 11.8 4.3, range 5.521; 79% boys).
Results were associated with gender and use of medications, and were
correlated with age, BMI, and adaptive functioning of ASD participants
as reflected by scores of Autism Diagnostic Observation Schedule
(ADOS-2), Vineland Adaptive Behavior Scale-II (VABS-II), and Social
Responsiveness Scale-II (SRS-2).
"Results
Children with ASD had lower levels (pmol/mL, mean SEM)
of AEA (0.722 0.045 vs. 1.252 0.072,
P < 0.0001, effect size 0.91), OEA
(17.3 0.80 vs. 27.8 1.44,
P < 0.0001, effect size 0.94), and PEA
(4.93 0.32 vs. 7.15 0.37,
P < 0.0001, effect size 0.65), but not AA and 2-AG.
Serum levels of AEA, OEA, and PEA were not significantly associated or
correlated with age, gender, BMI, medications, and adaptive
functioning of ASD participants. In children with ASD, but not in the
control group, younger age and lower BMI tended to correlate with
lower AEA levels. However, these correlations were not statistically
significant after a correction for multiple comparisons."
In their conclusion, the authors of "Lower circulating
endocannabinoid levels in children with autism spectrum disorder"
suggest using these as a diagnostic:
"We found lower levels of the endocannabinoids AEA, OEA, and PEA in
serum samples of 93 children with ASD compared with samples of matched
neurotypical control group. These findings are in line with the
results of numerous former studies in animal models of ASD as well as
an initial human study that demonstrated lower endocannabinoid tone in
ASD. Our findings suggest the use of circulating AEA, OEA, and PEA as
stratifying biomarkers of ASD and future studies should assess the
clinical significance of this stratification. These markers can also
be easily measured longitudinally in humans and in animal models
alike, and future studies should evaluate their potential to assist in
the monitoring of treatment response. Further studies are needed to
determine whether circulating endocannabinoid levels are also lower in
infants and can assist in pre-symptomatic diagnosis and if they
reflect lower endocannabinoid tone in the brain, as found in animal
models of ASD."
https://molecularautism.biomedcentral.com/articles/10.1186/s13229-019-0256-6
[2051]
As Janna Champagne (2024) explains in "EndoCannabinoid Deficiency and
Autism" the general bias has been to ignore the unprofitable ECS and
gut-brain axis:
"Autism Spectrum Disorder (ASD) results from many complex
contributors creating pervasive imbalances. Research has theorized
about the involvement of dozens of genetic mutations for predisposing
Autism, and unfortunately the absence of targeted biomarkers spawned a
high reliance on behaviors to establish diagnostic criteria, as
detailed in the Diagnostic & Statistical Manual for Mental
Disorders (DSM-V). This lends to classification of ASD as a mental
health disorder, and approaches for alleviating the underlying
physical imbalances are often overlooked or dismissed in favor of
prescribing mental health pharmaceuticals (Pietropaolo, 2021).
"However, as we know of other mental health disorders, there are
underlying physical imbalances contributing to Autism symptoms and
behaviors, primarily in the Gastrointestinal (GI) tract, plus the
Immune & Neurological systems. These imbalances may be identified
and targeted through biometric assessment, and interventions are
proving beneficial for promoting improved long- term outcomes. In
recent years, many research studies reflect a strong link between
dysfunction of the EndoCannabinoid System (ECS) as a factor in
diagnosis of Autism (Pietropaolo, 2021).
"One major role of the ECS is creation of EndoCannabinoids, from
precursory intake of Omega fatty acids. These EndoCannabinoids
circulate throughout the body, similarly to the physiology of the
Endocrine system, producing substances and distributing them for
interaction with receptors located throughout the body. The ECS
receptors are found in every other system of the body, and the
interactions at these sites promote systemic homeostasis (Castillo,
2012)."
The problem is the alleged solution:
"The US Food & Drug Administration (FDA) approved pharmaceuticals
for addressing ASD symptoms are two anti-psychotics: Abilify and
Risperidone. Additionally, physicians often prescribe off-label use
medications as an attempt to de-escalate ASD behaviors, including
Selective Serotonin Reuptake Inhibitor (SSRI) anti-depressants,
Benzodiazepine anxiolytics, Ritalin/Adderall, and Anticonvulsants.
These medications entail substantial risk for side effects that may
impair quality of life, including Extra-Pyramidal Symptoms, seizures,
mitochondrial damage, paradoxical effects, and male breast
development. In addition, use of these medications entails known risks
of severe adverse effects that may be life-threatening, such as
Neuroleptic Malignant Syndrome, Steven Johnson Syndrome, and suicidal
ideation (Autism Research Institute, 2024). Compared objectively with
medical cannabis, and its mild or pleasurable side effects, and no
reports of substantiated harm, cannabis use entails fewer risk factors
(Goldstein, 2023)."
In her own results:
"Upon receiving treatment with medical cannabis, the subjects with
ASD were tested and salivary biomarkers were compared with the prior
levels from the ASD subjects, as well as the control groups
neurotypical baseline levels. The result of this data compilation
reflected that of the sixty-five biomarkers included, twenty-three of
the parameters shifted positively towards neurotypical baseline
(Siani-Rose, 2021).
"Additionally, the parent reporting reflected improved symptom and
behavior management after cannabis administration, compared with the
individual baseline. Overall, this evidence supports cannabis as a
harm reduction tool for addressing symptoms of ASD, strengthened by
case studies, patient outcomes, and this recent proof of improvement
in ASD-applicable biomarkers (Siani-Rose, 2021)."
https://www.researchgate.net/profile/Janna-Champagne/publication/388277723_EC_deficiency_and_Autism/links/67915d4495e02f182eae5dfb/EC-deficiency-and-Autism?_tp=eyJjb250ZXh0Ijp7ImZpcnN0UGFnZSI6InB1YmxpY2F0aW9uIiwicGFnZSI6InB1YmxpY2F0aW9uIn19
[4851]
At the time of the visit, did you know anything about the Defendant's
AEA, OEA or PEA levels?
More about PEA:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3744360/
[2053]
More about AEA, OEA, PEA, and SEA from Fezza et al (2014)
"AEA belongs to a class of naturally occurring molecules (NAEs) known
for a long time. One of its members, N-palmitoylethanolamine (PEA),
was first reported almost 50 years ago in humans, yet its
physiological relevant remains under debate when the mechanism is
other than via CBRs.
"PEA and other NAEs share with true eCBs many degradative mechanisms,
and they potentiate the effect of eCBs at their receptor targets by
competitively inhibiting their hydrolysis, or by allosterically
modulating their receptor binding: the so-called 'entourage effect'.
On this basis, these substances are also known as 'eCBs-like'
compounds (Table 1).
"Among the most studied eCBs-like compounds, the anti-inflammatory
agent PEA and the appetite-suppressor N-oleoylethanolamine (OEA) can
be listed (Table 1). Their biological activity often engages
PPARα and TRPV1 activation, although some of their actions are
prevented by CB1 antagonists. Among the eCBs-like compounds OEA shows
the highest affinity for PPARα, and consistently some of its
biological effects are absent in PPARα deficient mice. Yet, the
antinociceptive properties of OEA are exercised also through a
PPARα-independent mechanism.
"OEA, as well as PEA and 2-oleoylglycerol (2-OG) (Table 1), can also
activate GPR119, a GPCR expressed predominantly in human and rat
pancreas, suggesting that the effects of OEA on food intake may be
mediated, at least in part, via GPR119. Conversely, Lan and coworkers
reported that the hypophagic effect of OEA was preserved in
Gpr119(-/-) mice. Not surprisingly, there is also evidence that OEA
(as well as PEA) can engage, even though at high concentrations,
additional receptors like GPR55.
"Another saturated NAE, N-stearoylethanolamine (SEA), was reported to
act as a cell growth controller and anti-inflammatory/immunomodulatory
agent, through yet unknown targets. SEA also shows anorexic effects
that are PPAR-independent and, together with PEA, plays an
antinociceptive role in humans.
"As reported above, also the endogenous levels of these eCBs-like
compounds (PEA, OEA and SEA) are affected by different dietary
regimens, with different hits in the brain compared to peripheral
tissues."
[eCBs and eCBs-like compounds, molecular targets, biosynthetic and
catabolic enzymes 2054]
https://www.mdpi.com/1420-3049/19/11/17078
[2054]
Is alcohol connected with brain volumes?
In their narrative review of studies pertaining to the assessment of
CBD efficiency on drinking reduction, or on the improvement of any
aspect of alcohol-related toxicity in AUD, French researchers De
Ternay et al find:
"ARLD is a progressive alcohol-induced liver injury, which starts
with an increase in the amount of fat in the livera process called
steatosisand continues into a progressive cell loss, fibrosis, and
hepatic insufficiencya process called cirrhosis (OShea et al., 2010).
ARLD may result in severe liver failure, and represents a major risk
factor for liver cancer. Overall, alcohol-attributable liver damage is
responsible for 493,300 deaths every year, and 14,544,000 disability
adjusted life years (DALYs), representing 0.9% of all global deaths
and 0.6% of all global DALYs all over the world (Rehm et al., 2013).
In subjects with ARLD, preventing the transition from steatosis to
cirrhosis is a major treatment goal, and this usually requires to stop
or to dramatically reduce the average amount of consumed alcohol in
the long term (European Association for the Study of the Liver A et
al., 2018). AUD also affects the brain, through ARBI. Subjects with
AUD display reduced gray matter volumes and reduced cortical
thickness, as well as increased ventricular volumes, when compared to
matching healthy controls (Bhler and Mann, 2011). The most significant
reductions in grey matter volumes are observed in the
corticostriatallimbic circuits, including the insula, superior
temporal gyrus, dorso-lateral prefrontal cortex, anterior cingulate
cortex, striatum, and thalamus (Bhler and Mann, 2011). Cognitive
functions associated with these brain areas (e.g., executive
functions, working memory, emotion recognition, or long-term memory)
are impaired in subjects with AUD (Stavro et al., 2013). Generally,
cognitive dysfunctions start to improve quickly after alcohol
withdrawal, but patients substantially recover only within the first
weeks to months of alcohol abstinence, and sometimes remain impaired
(Stavro et al., 2013; Schulte et al., 2014). Similarly, the recovery
of structural brain alterations can be highly variable depending on
brain areas and individual features (Durazzo et al., 2015; Zou et al.,
2018). Overall, both ARLD and ARBI involve alcohol-related
inflammatory processes (Mandrekar and Ambade, 2014; Neupane, 2016).
Current medications for reducing alcohol drinking or supporting
alcohol abstinence in AUD subjects are still insufficiently effective
at a population level, and new therapeutic prospects are needed
(Rolland et al., 2016; Soyka and Mller, 2017). Moreover, no drug for
reducing alcohol-related harms, either on the brain or the liver, has
ever been studied."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6554654/
[1921]
Luckily we've been studying it for 12,000 years.
In "Regional Brain Volume Changes in Alcohol-dependent Individuals
during Short-term and Long-term Abstinence" Zou et al elaborate:
"Widespread brain atrophy in alcohol-dependent individuals (ALC) has
been consistently documented in pathological and magnetic resonance
imaging (MRI) studies. Longitudinal MRI studies have shown that the
regional brain volume losses in ALC are partially reversible during
abstinence from alcohol. The goal of this study was to determine
volume reductions in cortical and subcortical regions functionally
important to substance use behavior and their changes during
short-term (1 week to 1 month) and long-term abstinence (1 month to 7
months) from alcohol. The regions of interests (ROIs) were: anterior
cingulate cortex (ACC), dorsolateral prefrontal cortex (DLPFC),
orbitofrontal cortex (OFC), insula, amygdala, and hippocampus."
You can see the brain volumes increasing after one week, one month,
and 7 months of abstinence at their Figure 1
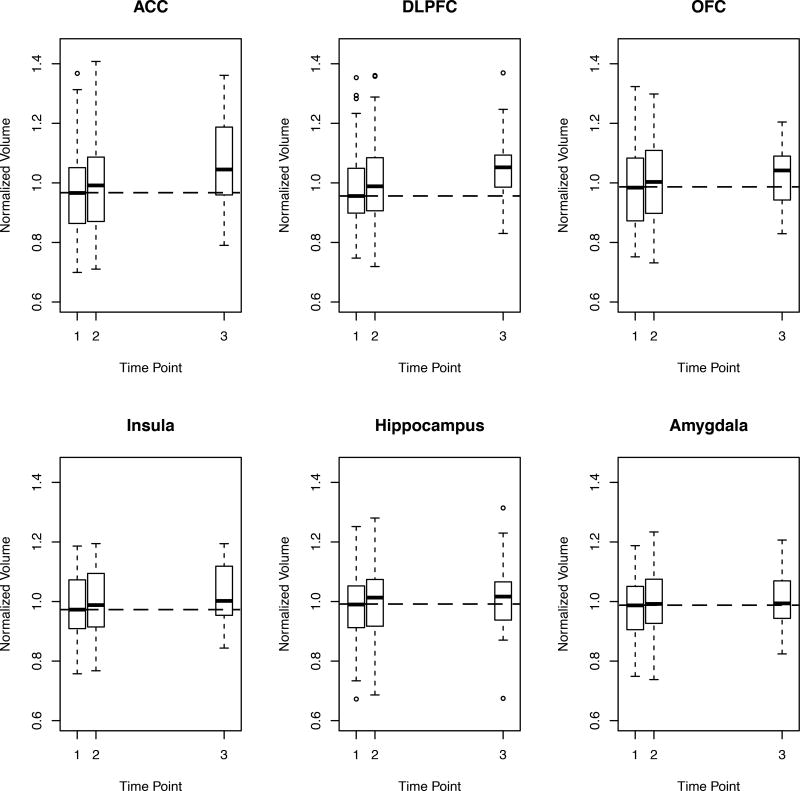
In their Table 2 you can see the amount of brain involved. To begin
with, all the drinkers' brains are smaller in volume than the
non-drinkers. For instance the dorsolateral prefrontal cortex grew
back at a quadratic rate of 28.0 mm3/month2.
In summary:
"The regional volumes in CON did not change significantly over the
10-months scan interval, attesting to the stability of our measurement
paradigm over time. By contrast, in ALC, the volumes of DLPFC, OFC,
insula, and hippocampus increased over the TP1-TP2 (all p < 0.005)
and TP2-TP3 intervals (all p < 0.012). The ACC volume increased
significantly only over TP2-TP3 (p = 0.013), but the volume did not
increase significantly over the TP1-TP2 interval. The amygdala volume
tended to increase only during the TP1-TP2 interval (p = 0.058) and
remained practically unchanged after TP2. The linear monthly volume
change rates in the DLPFC, OFC, and insula were about 4 to 6 times
higher during short-term than long-term abstinence (2.5 times for the
ACC), so that up to 50% of the observed volume increases in these ROIs
over the entire 7-months abstinence period occurred during the first
month of abstinence. Over the entire abstinence period, the DLPFC,
OFC, and insula also showed significant non-linear volume recovery
trajectories, i.e., the quadratic monthly volume change rates were
significant (all p < 0.009) (see Table 2). The significant
quadratic rates of these three ROIs were all negative (i.e., frowning
parabolas), indicating that the volumes of these three ROIs increased
faster during short-term abstinence than long-term abstinence."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5984169/
[2868]
A 2021 UK Biobank study from Topiwala et al, was
"...one of the largest imaging investigations into the impact of
alcohol consumption on brain health to date. The very large sample
size provided great statistical power to detect associations across
almost the whole cortex, subcortical structures and cerebellum that
have previously been uncharacterized, as well as extensively explore
interactions with clinical and drinking behaviours. It used
state-of-the-art neuroimaging and results were stringently controlled
for more potential confounders than ever before, as well as multiple
testing which increases confidence in the findings."
Which showed no lower threshold for alcohol damage in terms of grey
matter volume:
"Alcohol consumption was negatively linearly associated with global
brain grey matter volume (beta= -0.1, 95%CI= -0.11 to -0.09,
p<2x10-16). The association with alcohol was stronger than other
modifiable factor tested and robust to unobserved confounding.
Widespread negative associations were observed with white matter
microstructure (beta= -0.08, 95%CI= -0.09 to -0.06, p<2x10-16) and
positive correlations with functional connectivity. Higher blood
pressure and body mass index increased risk of alcohol-related harm
(SBP*alcohol: beta= - 0.01, 95%CI = -0.02 to -0.004, p=0.005;
BMI*alcohol: beta= -0.01, 95%CI = -0.02 to -0.002, p=0.02). Binging on
alcohol had additive negative effects on brain structure on top of the
absolute volume consumed (daily compared to never binging: beta=
-0.19, 95%CI= -0.30 to -0.08, p<0.01). No evidence was found for
differential effects of drinking wine, beer or spirits.
"Conclusions
No safe dose of alcohol for the brain was found. Moderate consumption
is associated with more widespread adverse effects on the brain than
previously recognised. Individuals who binge drink or with high blood
pressure and BMI may be more susceptible. Detrimental effects of
drinking appear to be greater than other modifiable factors. Current
'low risk' drinking guidelines should be revisited to take account of
brain effects."
https://www.medrxiv.org/content/10.1101/2021.05.10.21256931v1.full.pdf
[3542]
In 2022's "Association Between Brain Structure and Alcohol Use
Behaviors in Adults: A Mendelian Randomization and Multiomics Study"
Mavromatis et al set out in JAMA Psychiatry:
"To use mendelian randomization (MR) to identify directional
associations between brain structure and alcohol use and elucidate the
transcriptomic and cellular underpinnings of identified
associations."
as
"Recently developed genomics methods, including latent causal
variable analysis and mendelian randomization (MR), facilitate the
identification of directional associations between genetically
influenced variables from population based observational data and have
been underapplied to questions regarding alcohol use and brain
structure."
and
"The main bidirectional MR analyses were performed in samples
totaling 763 874 individuals, among whom more than 94% were of
European ancestry, 52% to 54% were female, and the mean cohort ages
were 40 to 63 years. Negative associations were identified between
genetically predicted GCT and binge drinking (β, −2.52; 95%
CI, −4.13 to −0.91) and DPW (β, −0.88; 95% CI,
−1.37 to −0.40) at a false discovery rate (FDR) of 0.05.
These associations remained significant in multivariable MR models
that accounted for neuropsychiatric phenotypes, substance use, trauma,
and neurodegeneration. TWAS [transcriptome-wide association studies]
of GCT [global cortical thickness] and alcohol use behaviors
identified 5 genes at the 17q21.31 locus oppositely associated with
GCT and binge drinking or DPW [drinks per week] (FDR = 0.05).
Cell-type enrichment analyses implicated glutamatergic cortical
neurons in alcohol use behaviors."
and
"Our large sample sizes (between 19 629 and 537 349 participants)
increased statistical power relative to previous brain
structurealcohol consumption studies. Our findings suggest that a
predisposition toward lower GCT may be associated with greater alcohol
consumption and binge drinking. Conversely, we failed to find strong
evidence that a genetic predisposition for alcohol associated with
brain structure or its longitudinal plasticity."
and
"Our investigation of the transcriptomic relationship between GCT and
alcohol use identified 5 protein coding genes oppositely associated
with GCT and alcohol use behavior: PLEKHM1, LRRC37A2, CRHR1, ARHGAP27,
and LRRC37A. These 5 genes could contribute to the negative
association between GCT and alcohol use. All 5 are located at
17q21.31. This locus, characterized by extensive linkage
disequilibrium, is the site of 2 haplotypes: the inverted H2 haplotype
(found in approximately 20% of individuals of European ancestry), and
the H1 haplotype."
and
"Our cell-type analysis also found that excitatory neurons may
underlie GCTs association with alcohol use. These data support the
notion that glutamatergic transmission plays an important role in
alcohol misuse. Interestingly, CRHR1 is expressed in glutamatergic,
but not GABAergic, cortical neurons. Activation of CRHR1 in the
forebrain is associated with alteration in glutamatergic
neurotransmission and increased behavioral susceptibility to stress in
mice. Therefore, our single-cell findings support our hypothesis
associating cortical CRHR1 expression with increased stress
susceptibility, cortical thinning, and alcohol misuse."
https://jamanetwork.com/journals/jamapsychiatry/articlepdf/2795312/jamapsychiatry_mavromatis_2022_oi_220047_1662054847.3687.pdf
[2140]
Durazzo et al (2023) concentrated on cortical thickness in alcohol
withdrawal, but for a longer period than previous attempts. As the
authors explained:
"Cortical thickness may show a differential pattern of recovery with
abstinence in alcohol use disorder (AUD) compared to volume and
surface area measures in the same brain regionsThe cerebral cortex is
primarily composed of neuronal and glial cells [i.e., astrocytes,
oligodendrocytes, and microgliaand the ratio of glial cells to neurons
is approximately 0.7:1; accordingly, cortical thickness may serve as a
macroscopic surrogate marker of the cytoarchitectural integrity of
cells comprising the cortex."
So
"AUD participants were studied at approximately 1 week (n=68), 1
month (n=88) and 7.3 months (n=40) of abstinence.
"Forty-five never-smoking controls (CON) completed a baseline study,
and 15 were reassessed after approximately 9.6 months. Participants
completed magnetic resonance imaging studies at 1.5T and cortical
thickness for 34 bilateral regions of interest (ROI) was quantitated
with FreeSurfer. AUD demonstrated significant linear thickness
increases in 25/34 ROI over 7.3 months of abstinence."
But the
"...rate of change from 1 week to 1 month was greater than 1 month to
7.3 months in 19/34 ROIs."
Overall
"After 7.3 months of abstinence, AUD were statistically equivalent to
CON on cortical thickness in 24/34 ROIs; the cortical thickness
differences between AUD and CON in the banks superior temporal gyrus,
post central, posterior cingulate, superior parietal, supramarginal
and superior frontal cortices were driven by thinner cortices in AUD
with proatherogenic conditions relative to CON. In actively smoking
AUD, increasing pack-years was associated with decreasing thickness
recovery primarily in the anterior frontal ROIs..."
and
"Widespread bilateral linear cortical thickness recovery over 7.3
months of abstinence was the central finding for this AUD cohort.
Proatherogenic conditions were associated with decreased thickness
recovery and thinner cortex after 7.3 months of abstinence in several
ROIs; this suggests alterations in perfusion or vascular integrity may
relate to structural recovery in AUD. These results support the
adaptive and beneficial effects of sustained sobriety on brain
structural recovery in those with AUD."
https://www.sciencedirect.com/science/article/abs/pii/S074183292300263X
[4191]
Shapson-Coe et al (2024) found a different glia to neuron ratio in
their 1 cubic mm sample:
"To fully understand how the human brain works, knowledge of its
structure at high resolution is needed. Presented here is a
computationally intensive reconstruction of the ultrastructure of a
cubic millimeter of human temporal cortex that was surgically removed
to gain access to an underlying epileptic focus. It contains about
57,000 cells, about 230 millimeters of blood vessels, and about 150
million synapses and comprises 1.4 petabytes. Our analysis showed that
glia outnumber neurons 2:1, oligodendrocytes were the most common
cell, deep layer excitatory neurons could be classified on the basis
of dendritic orientation, and among thousands of weak connections to
each neuron, there exist rare powerful axonal inputs of up to 50
synapses. Further studies using this resource may bring valuable
insights into the mysteries of the human brain."
https://www.science.org/doi/10.1126/science.adk4858
[4641]
Alcohol is not a drug, it's a drink. So we don't need to worry about
these brain volumes or cortical thicknesses in Ptuj, where I think you
would struggle to find 40 people who didn't have a drink for 7.3
months.
It is sufficient to note that any change in cortical thickness from
cannabis alone is a separate and distinct effect from cortical
thinning caused by alcohol consumption.
Owens et al (2022) say
"Cortical thinning in adolescence is well-established as a normal
trajectory of brain development. Studies estimate cortical thinning of
around 1% annually, which comes out to around 0.030.06 millimeters per
year."
Moreover there is research
"...suggesting that the accelerated thinning may be mediated, in
part, by cannabis exposure affecting the brains endogenous cannabinoid
system. That said, it remains possible that these brain changes may
not be a consequence of the cannabis exposure but may reflect instead
a neurodevelopmental trajectory caused by other factors that is
related to a higher likelihood of adolescent cannabis use."
https://www.nature.com/articles/s41398-022-01956-4
[4193]
The good news is that marijuana use appears, for whatever reason, to
ameliorate cortical thinning in drinking teenagers. From the
perspective of this metric you are better off with both than alcohol
alone.
In "Adolescent Cortical Thickness Pre- and Post Marijuana and Alcohol
Initiation" by Jacobus et al (2016):
"Adolescents (N=69) were followed from ages 13 (pre-initiation of
substance use, baseline) to ages 19 (post-initiation, follow-up).
Three subgroups were identified, participants that initiated alcohol
use (ALC, n=23, >20 alcohol use episodes), those that initiated
both alcohol and marijuana use (ALC+MJ, n=23, >50 marijuana use
episodes) and individuals that did not initiate either substance
regularly by follow-up (CON, n=23, <3 alcohol use episodes, no
marijuana use episodes). All adolescents underwent neurocognitive
testing, neuroimaging, and substance use and mental health
interviews."
This is their Figure 2:
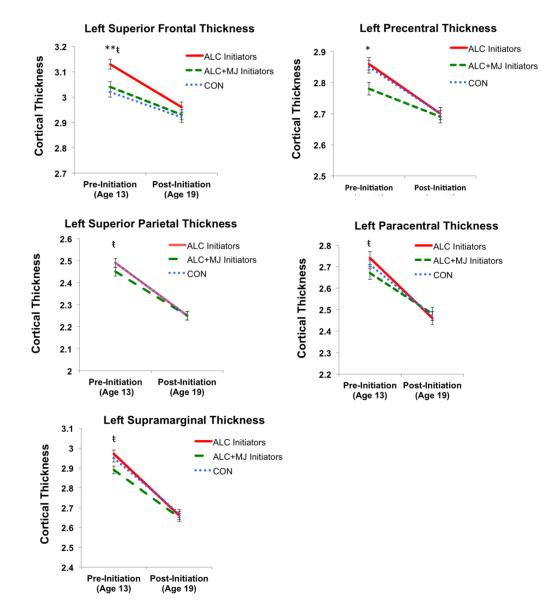
"Examination of 34 independent cortical regions in each hemisphere
revealed significant Group by Time effects, largely consistent with a
significant decrease in cortical thickness over time in the ALC group
compared to the ALC+MJ group (ps<.05). Findings within each lobe of
the brain are presented below (see Figures 2--4).4). Intracranial
volume (ICV) was identified a priori as a covariate."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5072451/
[4192]
If you are banning marijuana for reasons of cortical thickness, it
only raises questions as to why there is no minimum age for drinking
alcohol in public in Slovenia, since these authors didn't even bother
to find a marijuana-only cohort, suggesting alcohol might be a gateway
drug. I think we can also conclude these studies were not as advanced
in 1925, 1961, 1971 and 2000, as they today are, and this topic played
no role in the prohibition of cannabis.
Despite this, unlike our alcoholic cousins, cannabis users know very
well that THC isn't for everyone. Who knew? Where is the equivalent
analysis for wine? Can we find more than associations. Can we actually
say there are genes which CAUSE people to drink?
With a lot of data and math, we can. After finding correlations
between schizophrenia and opioids, nicotine, cannabis and - most of
all - alcohol...
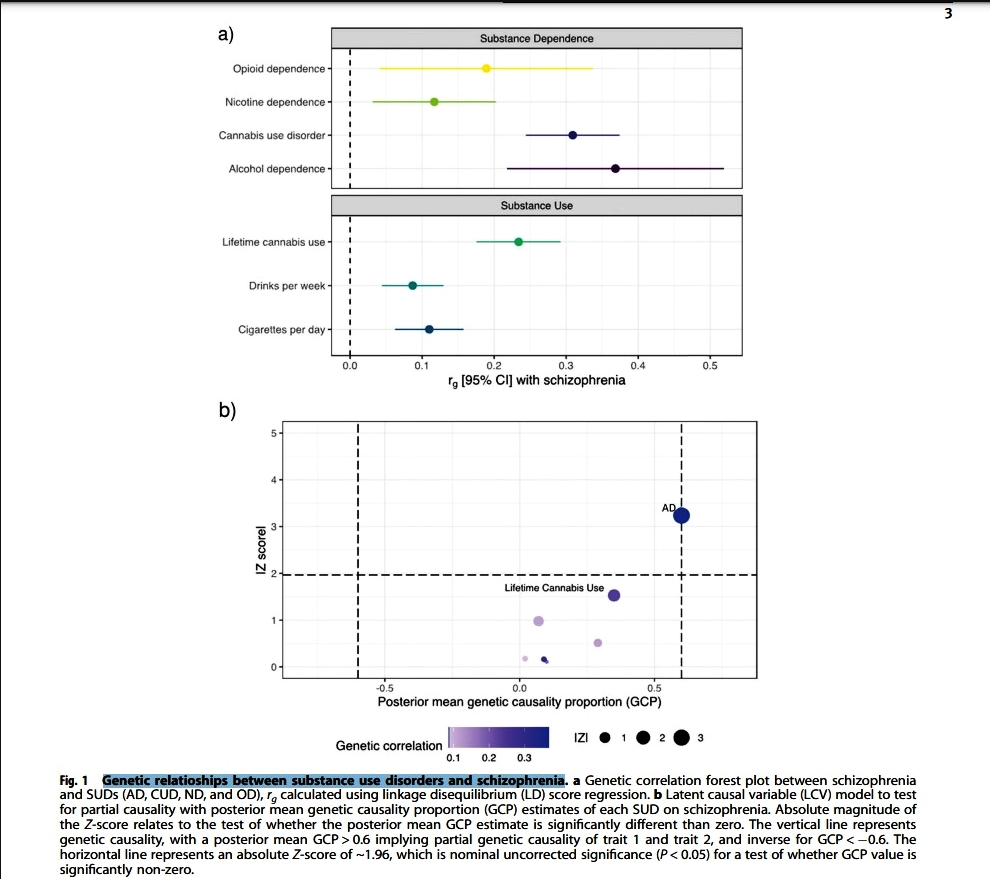
...Greco et al in Translational Psychiatry (2022) write:
"Evidence for partial genetic causality of alcohol dependence on
schizophrenia LD score regression (LDSR) analysis revealed significant
genetic correlations between schizophrenia and several of the SUD
phenotypes after correcting for the number of tests performed (Fig.
1a). Specifically, schizophrenia was positively genetically correlated
with AD (rg = 0.368, SE = 0.076, P = 1.61 10−6 ), CUD (rg =
0.309, SE = 0.033, P = 1.97 10−20), ND (rg = 0.117, SE = 0.043,
P = 7.0 10−3 ), and the substance use phenotypes CPD (rg = 0.11,
SE = 0.024, P = 4.93 10−6 ), DPW (rg = 0.087, SE = 0.021, P =
6.36 10−5 ) and LCU (rg = 0.234, SE = 0.029, P = 3.74
10−15). We also found nominally positive genetic correlation
between schizophrenia and OD (rg = 0.184, SE = 0.075, P = 0.0142),
however, this did not survive multiple-testing correction. LCV models
were then constructed for the significant traits for which their
schizophrenia genetic correlation estimate passed multiple-testing
correction (AD, CUD, ND, CPD, DPW, and LCU) to investigate whether any
of the observed genetic correlations between SUD and schizophrenia may
constitute a causal relationship (Fig. 1b, Supplementary Table 1).
There was no evidence for partial genetic causality of CUD, ND, CPD,
DPW, and LCU on schizophrenia, but there was moderate evidence that AD
was partially genetically causal for schizophrenia (GCP = 0.60, SE =
0.22, P = 0.001). We note that while the SNP heritability estimate for
AD was significantly non-zero, the Z-score for AD (h2 / SE) was
somewhat noisier (Zh 2 = 5.98) than recommended by the authors of the
LCV method (Zh 2 > 7). As a result, this inference of partial
genetic causality needs to be cautiously interpreted in light of this,
with larger GWAS of AD diagnosed using DSM-IV/DSM-V or similar likely
required to boost the precision of AD SNP heritability. DPW did not
show any evidence for a causal relationship with schizophrenia like
alcohol dependence. Interestingly, AD and DPW showed genetic
correlation (rg = 0.709, SE = 0.105, P = 1.38 10−11), as did CUD
and LCU (rg = 0.476, SE = 0.049, P = 2.71 10−22) but there was
no evidence of partial genetic causality of DPW on AD (GCP = 0.05, SE
= 0.56, P = 0.88) or CUD and LCU (GCP = 0.02, SE = 0202, P = 0.976).
No evidence of genetic correlation was observed among ND and CPD (rg =
0.071, SE = 0.054, P = 0.192). These results suggest that the
underlying mechanisms driving AD, CUD, and ND may not strongly present
in substance use observed in a population sample, although this
requires further investigation."
With this collection of correlations Greco et al go on to reveal some
evidence for causation:
"In the pairwise meta-analysis, 73 gene-sets were statistically
significant (FDR < 0.05), for schizophrenia meta-analysed with AD,
with 10 gene-sets not previously observed in the individual
schizophrenia GWAS (Supplementary Table 10), including longterm
synaptic potentiation (ngenes = 81, P = 5.71 10−5, FDR = 0.02),
exocytic vesicle (ngenes = 196, P = 1.23 10−4, FDR = 0.03),
paroxysmal ventricular tachycardia (ngenes = 23, P = 1.70 10−4,
FDR = 0.03), peptidyl serine dephosphorylation (ngenes = 19, P = 1.75
10−4, FDR = 0.04), hypoplasia of the olfactory bulb (ngenes = 4,
P = 2.12 10−04, FDR = 0.04), regulation of heart contraction
(ngenes = 221, P = 2.32 10−4, FDR = 0.04), and regulation of
peptidyl serine dephosphorylation (ngenes = 5, P = 2.32 10−4,
FDR = 0.04)."
"We further constructed latent causal variable (LCV) models to test
for partial genetic causality and found evidence for a potential
causal relationship between alcohol dependence and schizophrenia (GCP
= 0.6, SE = 0.22, P = 1.6 10−3 ). This putative causal effect
with schizophrenia was not seen using a continuous phenotype of drinks
consumed per week, suggesting that distinct molecular mechanisms
underlying dependence are involved in the relationship between alcohol
and schizophrenia. To localise the specific genetic overlap between
schizophrenia and substance use disorders (SUDs), we conducted a
gene-based and gene-set pairwise meta-analysis between schizophrenia
and each of the four individual substance dependence phenotypes in up
to 790,806 individuals. These bivariate meta-analyses identified 44
associations not observed in the individual GWAS, including five
shared genes that play a key role in early central nervous system
development. The results from this study further supports the
existence of underlying shared biology that drives the overlap in
substance dependence in schizophrenia, including specific biological
systems related to metabolism and neuronal function."
and
"We then considered the association of 2,598 microRNA (miRNA)
regulatory target prediction gene-sets with each individual GWAS,
followed by the bivariate meta-analyses (Supplementary Tables 1418).
There were 239 miRNA that passed FDR correction for the individual
schizophrenia GWAS, no miRNA regulator target genesets passed FDR
correction for any of the individual substance dependence phenotypes.
Notably, each of the meta-analyses revealed a total of 17 microRNA
regulatory target gene-sets, not seen in the individual phenotypes,
including six found in more than one bivariate meta-analysis. One such
interesting example was the predicted target genes of miR-495, a
microRNA that is highly enriched in the nucleus accumbens and has been
shown to play a role in addiction-related behaviours. MiR-495 survived
correction in both schizophrenia and AD meta-analysis (ngenes = 231, P
= 2.43 10−3, FDR = 0.03), and the schizophrenia and ND model
(ngenes = 231, P = 5.88 10−5, FDR = 0.01) but was only nominally
significant in the individual schizophrenia GWAS (P = 0.007),
supporting how this meta-analysis approach can increase discovery
power."
The authors discuss this
"...further evidence of a causal relationship between alcohol
dependence and schizophrenia. Interestingly, there was no causal
relationship between the consumption of alcohol (drinks per week) and
schizophrenia, or between AD and DPW [drinks per week]. This was
consistent with the transancestral GWAS [genome-wide association
study] of alcohol dependence, which suggested there is a distinction
in the underlying molecular mechanisms driving pathological and
non-pathological behaviours for substance use and dependence,
particularly within biological pathways implicated in the
psychopathological aspects of problematic drinking. Additionally, it
is also well known that psychotic symptoms can occur in several
clinical conditions related to alcohol such as intoxication,
withdrawal, alcohol-induced psychotic disorder, and delirium. Although
registry data-sets come with several limitations such as the threat of
false-negatives due to under-reporting of substance use, a study on
18,478 Finnish inpatients found alcohol-induced psychosis was the most
common type of substance-induced psychotic disorder (SIPD), with a
separate Swedish study that followed 7606 individuals for 84 months
between 1995 and 2015 found that for alcohol the risk for SIPD was
4.7%. Interestingly, 22.1% (95% CI = 17.6−27.5) of patients who
had previously received a diagnosis of alcohol-induced psychosis went
on to develop schizophrenia. The putative causal relationship of AD on
schizophrenia warrants further epidemiological and biological
interrogation. There are also some important limitations to the use of
LCV [latent causal variable] modelsspecifically, they are bivariate in
nature, and thus, cannot model the effect of other plausible mediators
or confounders, while the posterior mean GCP [gradient conjugate
prior] estimate is also not a causal estimate that could be afforded
by approaches like Mendelian randomisation. However, the use of
Mendelian randomisation with a binary exposure like AD can be
challenging, particularly as only a handful of genome-wide significant
SNPs have been identified that could be suitable instrumental
variables."
https://www.nature.com/articles/s41398-022-02186-4.pdf
[1901]
The key idea of Mendelian randomisation is that, per Mendel's Law of
Independent Assortment, the random assignment of genetic variants
during meiosis mimics the randomisation that occurs in a randomised
control trial. All confounders (biological and social factors) are
otherwise balanced if we study people according to their allocated
genetic variants,
"The use of the terms loci, alleles, genes, genotype, and
polymorphisms has evolved since Mendels use of differentiating
characteristics, and conventions in usage differ between human and
animal geneticists, which adds to confusion. For clarity, these terms
are defined (Box 4, Figure 2) [below]. Briefly, the genotype of an
individual refers to the two alleles inherited at a specific locusif
the alleles are the same, the genotype is homozygous, if different,
heterozygous. A polymorphism is the existence of two or more variants
(e.g. SNPs) at a locus. The basic ideais that, if such polymorphisms
produce phenotypic differences that mirror the biological effects of
modifiable environmental exposures which in turn alter disease risk,
the different polymorphisms should themselves be related to disease
risk to the extent predicted by their influence on the phenotype.
Common polymorphisms that have a well-characterized biological
function can therefore be utilized to study the effect of a suspected
exposure on disease risk. One key point is that the distribution of
such polymorphisms is largely unrelated to the sorts of
confounderssocioeconomic or behaviouralthat were identified above as
having distorted interpretations of findings from observational
epidemiological studies."
And their glossary of genetic terms:
"alleles are the variant forms detectable at a locus
canalization is the process by which potentially disruptive
influences on normal development from genetic (and environmental)
variations are damped or buffered by compensatory developmental
processes
a gene comprises a DNA sequence, including introns, exons, and
regulatory regions, related to transcription of a given RNA
genotype of an individual refers to the two alleles inherited at a
specific locusif the alleles are the same, the genotype is homozygous,
if different, heterozygous
a haplotype is the set of alleles present at a series of linked loci
on a chromosome; a person has two haplotypes for any such series of
loci, one inherited maternally and the other paternally
linkage disequilibrium is the association between alleles at
different loci within the population. Linkage disequilibrium can exist
because alleles are physically close together and tend to be
co-inherited, or because they occur together for reasons of population
origin in subsections of an overall population and therefore
demonstrate a statistical association within the overall
population
a locus is the position in a DNA sequence and may be used to refer to
a single nucleotide polymorphism (SNP), or to larger regions of DNA
sequence
a marker is a segment of DNA with an identifiable physical location
on a chromosome, whose inheritance can be followed and can be assayed
in genetic association studies. In such studies, markers are of
interest if they are linked to polymorphisms with functional
significance. A marker can be a gene, an SNP or a section of DNA with
no known function
a mutation is a permanent structural alteration in DNA or the process
by which a DNA sequence is altered
pleiotropy is the potential for polymorphisms to have more than one
specific phenotypic effect
polymorphism is the existence of two or more variants at a locus.
Conventionally, the prevalence in the population should be above 1% to
be referred to as a polymorphism; if prevalence is below this,
variants are referred to as mutations
population stratification is an example of confounding in which the
co-existence of different disease rates and allele frequencies within
population sub-sections lead to an association between the two at a
whole population level
single nucleotide polymorphisms (SNPs) are positions along a
chromosome where the genetic code varies between individuals by a
single base pair (pronounced snips)"
https://academic.oup.com/ije/article/32/1/1/642797?login=false
[1960]
The verbal idea of characteristics "Mendelizing" can be traced back
to Morgan in 1913.
https://archive.org/details/hereditysex00morg/page/87/mode/1up?ref=ol&view=theater&q=Mendelize
[1960]
Havard epidemiologists O'Connor and Price describe the LCV
model:
"The latent causal variable (LCV) model is based on a latent variable
L that mediates the genetic correlation between the two traits (Figure
1a). Under the LCV model, trait 1 is fully genetically causal for
trait 2 if it is perfectly genetically correlated with L; ``fully"
means that the entire genetic component of trait 1 is causal for trait
2 (Figure 1b). More generally, trait 1 is partially genetically causal
for trait 2 if the latent variable has a stronger genetic correlation
with trait 1 than with trait 2; ``partially" means that part of the
genetic component of trait 1 is causal for trait 2. In order to
quantify partial causality, we define the genetic causality proportion
(gcp) of trait 1 on trait 2. The gcp ranges between 0 (no partial
genetic causality) and 1 (full genetic causality). A high value of gcp
(even if it is not exactly 1) implies that interventions targeting
trait 1 are likely to affect trait 2. An intermediate value implies
that some interventions targeting trait 1 may affect trait 2....We
caution that low gcp estimates are not evidence of full genetic
causality, and we refer to trait pairs with low gcp estimates as
having limited partial genetic causality. LCV p-values test the null
hypothesis that gcp=0, and a highly significant p-value does not imply
a high gcp."
https://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC6684375&blobtype=pdf
[1962]
According to Lu Qi of the Department of Nutrition, Harvard School of
Public Health, Boston and elsewhere:
"The Mendelian randomization approach also holds considerable promise
in the study of intrauterine influences on offspring health
outcomes."
and
"Mendelian randomization studies may have particular relevance in
assessing the effects of long-term (lifetime) exposures, such as
dietary intake, lifestyle, and excessive adiposity, whereas RCTs can
examine only short-term effects. Interest in using Mendelian
randomization in causality inference has been growing rapidly over the
past 5 years."
and has a little more on the maths:
"Recently, the instrumental variable (IV) method was introduced as a
formal test of Mendelian randomization using the genetic markers as
IVs. This method calculates the predicted effect of exposure on
outcome, given the associations between genotype and exposure and
between genotype and outcome. The IV approach is widely used in
econometrics to deal with 'endogeneity,' a broad term covering
confounding, reverse causality, and regression dilution bias. An IV
should be: 1) not correlated with the confounders; 2) related to the
exposure of interest; and 3) related to the outcome only through the
exposure of interest. In the context of Mendelian randomization
analysis, the genetic variant, which is not associated with
confounding variables, can act as an IV for the environment exposure.
The two-stage least squares (2SLS) method is most widely used to fit
the IV models. In brief, in the first stage of the analysis, IV is
used to generate predicted values for the independent exposure
(endogenous) variable. The predicted value is then used in a
second-stage regression to explain the variation in outcome. The
F-statistics from the first-stage regressions can be used to evaluate
the strength of the IV in estimating the exposure. A value greater
than 10 is generally assumed to be a sign of sufficient strength.
Because genotype is associated with the exposure but not the
confounders, the predicted exposureoutcome association is not
confounded and is likely the estimate for the causal effect. Other
methods such as a structural equation model have also been used in
Mendelian randomization analysis. In the case of non-linear variables,
the structural equation approach allows a simpler interpretation of
the regression coefficients when compared with an IV approach."
Mendelian randomization has supported causality in some associations,
and abolished it in others (Table 1). They describe how genetic risk
factors for esophegal cancer were calculated:
"Alcohol consumption has been related to the risk of esophageal
cancer, partly through the carcinogenic effects of alcohols principal
metabolite acetaldehyde. However, alcohol intake tends to be
correlated with other lifestyle risk factors such as smoking and diet.
Lewis et al. examined the causal relation between alcohol and
esophageal cancer risk using genetic data on the ALDH2 (aldehyde
dehydrogenase 2 family) gene, which encodes the major enzyme
eliminating acetaldehyde. A single point mutation in ALDH2 results in
the 2*2 allele (glutamic acid to lysine substitution at residue 487)
and inactivation of the enzyme. This in turn leads to an accumulation
of acetaldehyde after alcohol intake. Individuals who are homozygous
for the 2*2 allele have peak blood alcohol levels that are 18 times
higher and heterozygotes 5 times higher than *1*1 homozygotes.
Drinking alcohol is likely to cause unpleasant symptoms such as
nausea, drowsiness, and headache in the carriers. Therefore, *2*2
homozygotes drink significantly less alcohol than the wild-type
carriers, and heterozygotes fall somewhere in the middle. The authors
performed a meta-analysis including 905 cases of esophageal cancer and
2,078 controls from seven studies carried out in Japan, Taiwan, and
Thailand. The relative risk (RR) of esophageal cancer for *1*1
homozygotes versus *2*2 homozygotes was 2.77 [95% confidence interval
(CI), 1.256.12]. The authors predicted RR for genotype *1*1 based on
the following data: 1) A meta-analysis that found light, moderate, and
heavy drinkers had 1.8-, 2.38-, and 4.36-fold higher risk of cancer,
respectively, than nondrinkers.27 2) One study reported that 9.4%,
28.2%, 39.6%, and 22.9% of *1*1 individuals were non-, light,
moderate, and heavy drinkers, respectively; whereas all 2*2
individuals were virtually nondrinkers. The overall RR for *1*1
homozygotes was then derived with a formula RR = RRi Pi, where i
denotes the drinking category (non-, light, moderate, or heavy), RRi
is the relative risk in the ith drinking category estimated by a
meta-analysis, and Pi is the assumed proportion of ith drinking
category among controls. The predicted RR was 2.54, comparable to the
meta-analysis on the non-confounded genetic association (RR = 2.77).
The data support a causal effect of drinking on esophageal cancer
risk."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3671930/
[1961]
Continuing with the drinking:
In Kapoor et al: "Multi-omics integration analysis identifies novel
genes for alcoholism with potential overlap with neurodegenerative
diseases" in Nature Communications 2021, the authors looked for causal
variants and genes...underlying the biology of alcohol use disorder
(AUD) and drinks per week (DPW):
"Using Mendelian Randomization-based methods on the largest available
transcriptomic and epigenomic data for brain tissues (Supplementary
Data 1) and myeloid cells, we prioritized regulatory variants that
influence AUD and DPW (Fig. 1). The current manuscript explored the
multi-omic integration results in AUD and DPW separately and
subsequently focused on the overlapping genes between these two
traits. Overlapping genes prioritized in current analysis are
primarily driven by individual GWASs. Therefore, these signals are
minimally influenced by the sample size bias that might arise due to
the integration of two correlated traits with extreme differences in
power....To the best of our knowledge, this is the largest systematic
multi-omics integration analysis to identify the functional impact of
variants and genes associated with two correlated but etiologically
distinct aspects of alcohol involvement."
Among the results:
"AUD meta-analysis. The large meta-analysis of AUD GWAS summary
statistics (N = 48,545 AUD cases and 187,065 controls) from the
Million Veterans Program (MVP)19, the Psychiatric Genetics consortium
(PGC-SUD)12 and the Collaborative Studies on Genetics of Alcoholism
(COGA)20 identified 1157 SNPs (31 independent lead SNPs) within or
near 79 genes at 10 independent loci associated with AUD
(Supplementary Figs. 14). We did not include UKB-AUDIT-P in this
meta-analysis to specifically focus on AUD. Many of these loci were
shared between the AUD GWAS meta-analysis and the DPW GWAS by Liu et
al. who identified 81 independent loci represented by 5197 (>200
independent lead) SNPs. A total of 360 SNPs associated with AUD and
DPW were in common (i.e., p < 5 10−8 in both GWAS)
(Supplementary Fig. 5). A large and nominally significant proportion
(45%) of AUD and DPW-associated SNPs were within intronic, UTR and
non-coding regions of the genome (Supplementary Fig. 6). LDSC analysis
using tissue specific epigenetic annotations. We used the stratified
linkage disequilibrium score (LDSC) regression to test whether the
heritability of AUD and DPW is enriched in regulatory regions
surrounding genes in a specific tissue. Using multi-tissue chromatin
(ROADMAP and ENTEX) data, we observed a significant enrichment of
promoter-specific epigenetic markers (H3K4me1/me3) in the fetal and
the adult (germinal matrix, frontal-cortex) brain (P < 5
10−8) (Fig. 2; Supplementary Data 2 and 3) for the SNPs
associated with AUD and DPW, respectively."
and
"Identification of SPI1 and MAPT as genes for AUD are good examples
of pleiotropy and/ or causal links between the alcohol intake and
susceptibility to AUD, other psychiatric disorders (e.g., depression),
and even Alzheimers disease and other neurodegenerative diseases. We
found that increased SPI1 expression in myeloid lineage cells was
associated with a higher DPW and higher risk for AUD. Recently, Zhang
and colleagues observed that protein expression levels of SPI1 in the
cerebellum and spleen from subjects with Major depressive disorder and
schizophrenia were significantly higher than in controls. In the past,
we have demonstrated that functional variants related to SPI1
expression are associated with the risk of Alzheimers disease. Similar
to this study, higher levels of expression of SPI1 is associated with
increased risk for Alzheimers disease. SPI1 (Spi-1 Proto-Oncogene)
encodes an ETS-domain transcription factor (PU.1) that regulates gene
expression during myeloid and B-lymphoid cell development and
homeostasis. This nuclear protein binds to a purine-rich sequence
known as the PUbox found near the promoters of target genes and, in
coordination with other transcription factors and cofactors, regulates
their expression; among the genes are LXR/RXR nuclear receptors. In
the brain, SPI1 is specifically expressed in microglia. Given SPI1s
control over expression of several downstream genes, this gene may be
a major reason enrichment of immune pathways is observed in
transcriptomic analysis of human and animal brains. Because of the
small fraction of microglia in bulk brain tissue, it is difficult to
study the expression of this transcription factor in transcriptomic
datasets from whole brains. Some studies using animal models have
reported that chronic alcohol consumption can influence the expression
of PU.1 in isolated microglia and peripheral lung macrophages.
However, these studies report the consequences of drinking on PU.1
expression whereas our study uses genomic evidence to demonstrate that
regulation of innate immune response likely underlies, at least in
part, susceptibility to increased drinking and eventual risk for AUD.
MAPT is another example of a pleiotropic relationship between AUD and
other neuropsychiatric and neurodegenerative disorders. Located on
chromosome 17, MAPT, encodes the tau proteins best known medically for
their role in central nervous system disorders such as Alzheimers
disease, frontotemporal dementia, Parkinsons disease, and the primary
tauopathies progressive supranuclear palsy and corticobasal
degeneration. Recently, Hoffman and colleagues showed that alcohol use
can upregulate the expression of pTau (Ser199/Ser202) in the
hippocampus of C57BL/6J mice. Another study in humans observed
differences in CSF-Tau levels in demented people with alcohol use vs
Alzheimer disease patients. CRHR1 (corticotropinreleasing hormone type
I receptor) is another gene on 17q.21.31, that has been reported to be
associated with alcoholism. However, in our analysis, we did not
observe an association between CRHR1 expression and alcohol
consumption. We also identified other genes that might be involved in
increased alcohol consumption through a variety of biological
mechanisms. For example, VPS4A at 16q23.1 has been implicated in
dopamine regulation, reward anticipation, and hyperactivity in an fMRI
study. We also identified functional variants for SULT1A1 and SULT1A2
genes that encode for Sulfotransferase Family 1A enzymes catalyzing
the sulfate conjugation of many hormones, neurotransmitters, drugs,
and xenobiotic compounds. In IPA disease enrichment analysis, we
observed a nominally significant overlap between genes implicated in
DPW with other neurological, behavioral and immune-related disorders
(Supplementary Fig 16). The genes associated with DPW also showed
significant enrichment for pathways related to TR/ RXR activation,
Lipoate biosynthesis, Estrogen biosynthesis, and Sirtuin signaling
(Supplementary Data 8). TRs (Thyroid hormone receptor) control the
expression of target genes involved in diverse physiological processes
and diseases, such as metabolic syndrome, obesity, and cancer, and,
therefore, are considered as important targets for therapeutic drug
development. RXRs (Retinoic X Receptor) are known to potentially
regulate the ethanol metabolizing enzymes after chronic alcohol
consumption. It has been reported that the human aldehyde
dehydrogenase-2 (ALDH2) promoter contains a retinoid response element,
which might be contributing to the regulation of the gene. Sirtuins
signaling has been shown to play an important role in cocaine and
morphine Action in the Nucleus Accumbens. Ferguson and colleagues
demonstrated that systemic administration of a nonselective
pharmacological activator of all sirtuins can increase the cocaine
reward."
"We have identified a number of candidate causal genes for DPW and
AUD, resulting from a multi-omic analysis of human genetic and
expression data."
Again attention is drawn to the lack of any practical use of this
data in treating the individual with the information available to him
or her under the present circumstances. What the everyday drinker or
his bar knows about, say, Slovenia's predisposing genes, is negligible
to nothing.
https://www.researchgate.net/journal/Nature-Communications-2041-1723/publication/354030227_Multi-omics_integration_analysis_identifies_novel_genes_for_alcoholism_with_potential_overlap_with_neurodegenerative_diseases/links/61208e290c2bfa282a5ce4ca/Multi-omics-integration-analysis-identifies-novel-genes-for-alcoholism-with-potential-overlap-with-neurodegenerative-diseases.pdf
[1902]
And let's not forget "Transancestral GWAS of alcohol dependence
reveals common genetic underpinnings with psychiatric disorders"
(2018) in which Walters et al remind us that
"Liability to alcohol dependence (AD) is heritable, but little is
known about its complex polygenic architecture or its genetic
relationship with other disorders. "
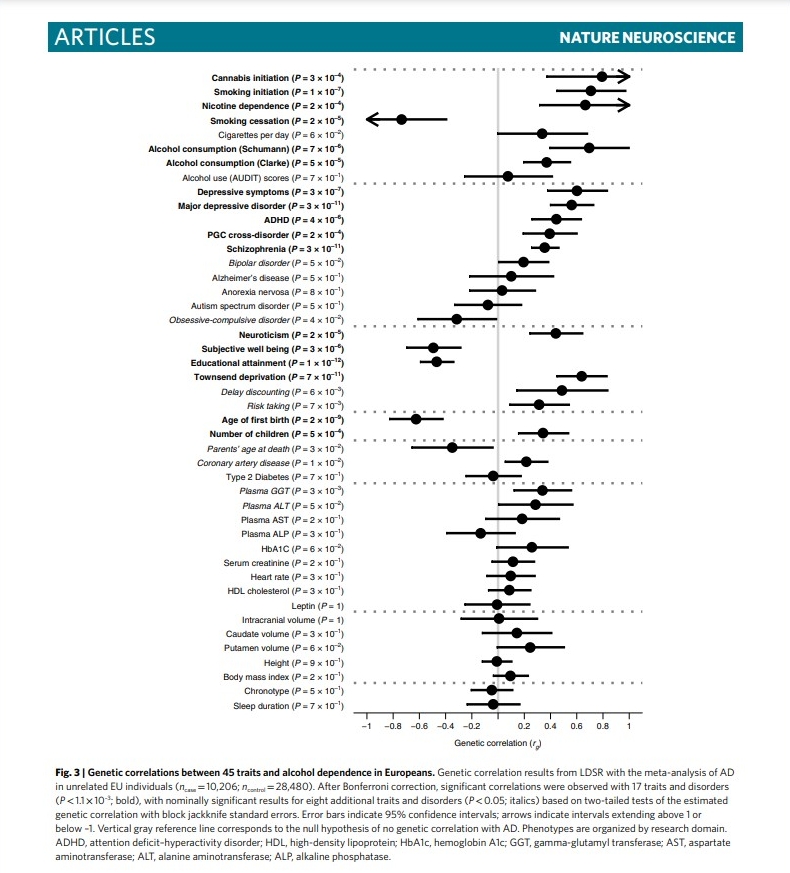
"The current analysis identified robust genetic correlation of AD
with a broad variety of psychiatric outcomes. This correlation was
strongest for aspects of negative mood, including neuroticism and
major depression, as also seen in twin studies and through recent
specific molecular evidence for pleiotropy. Taken together with
evidence from other recent genomic studies, and with null correlations
for other GWAS of alcohol consumption but not for measures of problem
drinking (for example, AUDIT-P), these findings suggest that major
depression may primarily share genetic liability with alcohol use at
pathological levels.
"AD was also strongly genetically correlated with poor educational
and socioeconomic outcomes and marginally correlated with measures of
risk-taking. Nominally significant genetic correlations with delay
discounting (i.e., favoring immediate rewards) and risktaking, and the
strong genetic correlation of AD with attention deficithyperactivity
disorder, cigarette smoking, and cannabis use, may similarly reflect a
shared genetic factor for risk-taking and reduced impulse control.
Common genetic liability to early, risky behaviors is characteristic
of both AD and age of first birth. The observed negative genetic
correlation with age of first birth is consistent both with
risk-taking and with the significant genetic correlations of AD with
lower socioeconomic status, as indexed by higher neighborhood Townsend
deprivation score and lower educational attainment. Lower
socioeconomic status is correlated with both AD and age of first
birth, and the current study suggests that shared genetic liabilities
may be one potential mechanism for their observed relationship.
However, the question of whether these genetic correlations represent
causal processes, horizontal pleiotropy, or the impact of unmeasured
confounders should be explored in the future.
"Lower genetic correlations were observed for most biomedical and
anthropometric outcomes. Liver enzymes GGT and ALT, once proposed as
possible biomarkers for alcohol abuse, showed only nominal evidence
for genetic correlation with AD, and neither survived multiple-testing
correction. Notably, we did not find any association between AD and
body-mass index (BMI). Negative genetic correlations with BMI were
previously reported for both alcohol consumption and AUDIT scores, but
there is prior evidence that BMI has differing underlying genetic
architectures in the context of AD and outside of that context. The
negative genetic correlations observed in those studies are consistent
with studies of light to moderate drinking, which is also associated
with healthier lifestyle behaviors, while heavy and problematic
drinking is typically associated with weight gain."
https://helda.helsinki.fi/bitstream/10138/307699/1/s41593_018_0275_1.pdf
[1904]
Philip C Haycock thinks the concept of a fetal alcohol spectrum
should be expanded to include preconceptional effects. Writing in
2009, he references not the latest research, but some animal
experiments published in 1913 which are very germane to this
preconceptual effect theory. The fetus is not directly exposed to the
toxin at all,
Dr Stockard's paper "The Effect on the Offspring of Intoxicating the
Male Parent and the Transmission of the Defects to Subsequent
Generations" is still widely cited today:
"In one extensive series of experiments, guinea pigs were treated by
the inhalation method to the point of intoxication every day, except
Sundays, for approximately 3 yr. 'From time to time,' treated animals
(males and females) were mated with untreated control. Various
experimental conditions were tested, such as 'alcoholized females'
'normal males' 'alcoholized females' 'alcoholized males,' and
'alcoholized males' 'normal females.'
"It was found that after 34 successful crossings between alcoholized
males and normal females, 24% of litters were stillborn. The remaining
litters produced 54 offspring, 39% of which died soon after birth. In
comparison, a normal male normal female crossing resulted in 33
litters, of which 1 (3%) was stillborn, and of the 60 live offspring,
4 (7%) died soon after birth. In addition, the untreated offspring of
parents from alcoholized conditions tended to have fewer surviving
offspring than controls (54% vs. 93%). In sum, these results suggest
that alcohol administered to males during the preconceptional period
resulted in high rates of perinatal mortality in offspring, and that
these effects persisted into the F(2) generation."
https://www.journals.uchicago.edu/doi/epdf/10.1086/279379
[1905]
After summarising various unpleasant physiological preconceptual
effects, upon the offspring, of alcohol administered to daddy rats
prior to conception, Haycock turns to behaviour.
"Studies employing chronic dosage regimens have also uncovered
behavioral effects of paternal alcohol exposure. For example, in one
study, 18-day-old offspring of male rats intubated with 3 or 2 g/kg
ethanol twice a day for 7 mo were more active in the open field
compared with controls, and they took a greater number of trials to
complete a passive avoidance learning task.
"In another study, male mice were maintained on a liquid diet for
5661 days in which alcohol provided 0%, 10%, or 20% of their calories.
Organ weights (except for thymus), litter size, and weights at birth
and at ages 21 and 55 days were not affected. However, a
dose-dependent decrease in physical activity at 20 and 24 days of age,
as well as decreases in serum testosterone at 55 days of age, were
observed in offspring derived from the alcohol treatment groups. In
addition, offspring of fathers receiving 20% of their calories from
alcohol performed better on a passive avoidance task but more poorly
in a T-maze task.
"In a study of both mice and rats, males received 0%, 10%, or 25% of
the calories from ethanol during 714 wk. It was observed that mice
from the alcohol-exposed group were relatively more immobile in a
swimming behavioral task. In contrast, rats from the alcohol-exposed
group displayed an opposite effect, being less immobile in the same
task.
"In a separate study, male rats receiving 17.5% or 35% of their
dietary calories from alcohol sired female offspring who performed
worse in a two-way shock avoidance learning task. However, no effects
on birth weight, spontaneous alternation, or passive avoidance
learning were observed.
"Studies employing acute dosage regimens have also reported effects
of paternal alcohol exposure on offspring development. In one study,
in which male rats were intubated with a once-off dose of either 6, 4,
2, or 0 g/kg ethanol, there was a significant dose-response effect on
the frequency of runts (<5.5 g at birth) and the number of
malformations. However, no differences in mating, fecundity, or litter
size were reported. In a separate study, a once-off dose of 5 g/kg
administered by intraperitoneal injection to male rats 24 h prior to
mating resulted in fewer matings, smaller litter sizes, and higher
fetal mortality."
Much more in the article about the possible mechanisms. He
concludes:
"In sum, alterations in epigenetic programming may underlie the
teratogenic consequences of ethanol exposure prior to conception, as
well as after conception, during preimplantation and gastrulation. One
of the main implications of an epigenetic perspective is that the FASD
spectrum is not limited to clinical defects arising from in utero
ethanol exposure, suggesting that the concept of a fetal alcohol
spectrum should be expanded to include preconceptional effects."
and
"Finally, an epigenetic perspective suggests that alcohol exposure
outside of the organogenic period (e.g., during preimplantation or
prior to conception) might have teratogenic consequences for the CNS.
Indeed, the association of paternal alcohol consumption with
behavioral and cognitive abnormalities in offspring in some animal and
human studies (discussed above) supports this view. Because such cases
are unlikely to receive a diagnosis within the FASD spectrum
(gestational alcohol exposure being a requirement for diagnosis), this
raises the possibility that transgenerational responses to alcohol
might account for a significant proportion of idiopathic
neurodevelopmental disorders (e.g., idiopathic autism) in humans."
https://academic.oup.com/biolreprod/article/81/4/607/2557677
[1906]
Burdinski et al (2024) longitudinally measured medical cannabis
users' task abilities and brain volumes using fMRI.
"No statistically significant difference in brain activation between
the 2 time points (baseline and 1 year) in those with medical cannabis
cards and no associations between changes in cannabis use frequency
and brain activation after 1 year were found."
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2823671
[3550]
In the years since the ZPPPD preconceptual epigenetic effects on
offspring have become a hot topic. In 2009 Ouko et al at the
University of Witwaterstrand reported on "Effect of alcohol
consumption on CpG methylation in the differentially methylated
regions of H19 and IG-DMR in male gametes: implications for fetal
alcohol spectrum disorders":
"Background: Exposure to alcohol in utero is the main attributable
cause of fetal alcohol spectrum disorders (FASD) which in its most
severe form is characterized by irreversible behavioral and cognitive
disability. Paternal preconception drinking is not considered to be a
significant risk factor, even though animal studies have demonstrated
that chronic paternal alcohol consumption has a detrimental effect on
the physical and mental development of offspring even in the absence
of in utero alcohol exposure. It has been documented that alcohol can
reduce the levels and activity of DNA methyltransferases resulting in
DNA hypomethylation and that reduced methyltransferase activity can
cause activation of normally silenced genes. The aim of this study was
to establish a link between alcohol use in men and hypomethylation of
paternally imprinted loci in sperm DNA in genomic regions critical for
embryonic development, thus providing a mechanism for paternal effects
in the aetiology of FASD.
"Methods: Sperm DNA from male volunteers was bisulfite treated and
the methylation patterns of 2 differentially methylated regions
(DMRs), H19 and IG-DMR, analyzed following sequencing of individual
clones. The methylation patterns were correlated with the alcohol
consumption levels of the volunteer males.
"Results: There was a pattern of increased demethylation with alcohol
consumption at the 2 imprinted loci with a significant difference
observed at the IG-DMR between the nondrinking and heavy alcohol
consuming groups. Greater inter-individual variation in average
methylation was observed at the H19 DMR and individual clones were
more extensively demethylated than those of the IG-DMR. CpG site #4 in
the IG-DMR was preferentially demethylated among all individuals and
along with the H19 DMR CpG site #7 located within the CTCF binding
site 6 showed significant demethylation in the alcohol consuming
groups compared with the control group.
"Conclusion: This study demonstrates a correlation between chronic
alcohol use and demethylation of normally hypermethylated imprinted
regions in sperm DNA. We hypothesize that, should these epigenetic
changes in imprinted genes be transmitted through fertilization, they
would alter the critical gene expression dosages required for normal
prenatal development resulting in offspring with features of
FASD."
https://pubmed.ncbi.nlm.nih.gov/19519716/
[3331]
Day et al in "Influence of paternal preconception exposures on their
offspring: through epigenetics to phenotype" (2016) discuss paternal
age (the Defence asserts genetic age supervenes calendar age),
paternal diet (the Defence asserts cannabis and psychedelics improve
dietary choices and that cannabis assists digestive metabolism),
environmental toxicants and psychosocial stressors (the Defence
asserts the Town Smell falls into both categories), and particularly
alcohol (the Defence evidence shows cannabis and psychedelics are
associated with reduced alcohol consumption):
"FASDs are a broad array of congenital disorders with major symptoms
including reduced birth weight, impaired cognitive function and
behavior, and neuropsychological deficits in visual-spatial learning.
Studies have shown that paternal alcohol consumption has epigenetic
effects on sperm DNA, suggesting a role in the development of
congenital disorders in offspring. Up to 75% of children with FASD
have biological fathers who are alcoholics, suggesting that
preconceptional paternal alcohol consumption negatively impacts their
offspring. It has been shown that teratogens such as alcohol
significantly reduce the activity of DNA methyltransferases, leading
to increased CG hypomethylation and subsequent activation of normally
silenced genes. Chronic paternal alcohol consumption alone
hypomethylates his offsprings genes even in the absence of maternal
alcohol consumption before or during pregnancy. This epigenetic
hypomethylation alters gene expression dosages required for normal
prenatal development, resulting in offspring with characteristic
symptoms of FASDs. Here we examine the effects of paternal alcohol
consumption on the prevalence and symptoms of FASDs and related
congenital defects.
"Effects on birthweight and individual organ weights
A hallmark symptom of FASD is decreased newborn birth weight. Murine
studies have shown that offspring from alcohol-treated fathers have a
higher prevalence of low birth weights. A study in rats has shown that
offspring from alcohol-treated fathers decreased in weight by two or
more standard deviations when compared to the average weight of
offspring born from controls. This effect was observed in offspring of
both acute and long-term alcohol-treated fathers, which suggests that
epigenetic modifications are sensitive to even small amounts of
paternal alcohol consumption. In addition to marked decreases in birth
weight, studies have shown that alcohol consumption can alter the
weight of individual organs. For example, fathers treated with alcohol
for several weeks prior to breeding were more likely to produce
offspring with increased adrenal weights and decreased spleen weights.
This suggests that paternal alcohol consumption may also have an
epigenetic impact on the gene expression governing individual organ
development. Furthermore, autopsy and brain imaging studies have shown
marked reductions in overall brain size, specifically in the
cerebellum, basal ganglia, and corpus callosum. This observed
physiological effect on brain structures can explain impaired
cognitive function displayed by offspring sired by alcohol-treated
fathers.
"Effects on cognitive behavior and motor ability
Studies have demonstrated the adverse effects of paternal alcohol
consumption on the cognitive and motor ability of offspring. For
example, one study involved feeding male mice varied liquid alcohol
diets containing 25%, 10%, or 0% ethanol-derived calories (EDC). After
7 to 14 weeks of diet treatment, the males were bred to non-treated
females. Offspring were then subjected to a forced swim test, in which
offspring of alcohol-sired fathers were more immobile than offspring
of fathers receiving 0% EDC. While this may suggest decreased motor
ability due to paternal alcohol consumption, this seems to also be a
species-specific effect. The same study was conducted on rats, showing
opposite results with offspring of alcohol-sired fathers exhibiting
increased mobility.
"One possible explanation for this discrepancy could be the species
specific response to stressful situations. In humans, it is known that
children with fetal alcohol syndrome cope poorly with stressful
situations, and therefore display hyperresponsiveness to stress. In
these situations, stressors cause an increased corticosterone
response, resulting in exaggerated reactions to stressful situations.
This could explain why the rat offspring of alcohol-treated fathers
exhibited increased mobility when forced to swim; the
hyperresponsiveness to stress may override the impaired motor function
that is normally seen in affected offspring. While these results in
mice and rats may seem paradoxical, the mechanisms being affected need
to be isolated and examined separately to determine causation.
"In addition to this hyperresponsiveness seen in rats, similar
studies have also shown that rats sired by alcohol-treated fathers
have greater difficulty learning new tasks and have impaired spatial
learning skills when subjected to maze tests. Studies also suggest
that epigenetic modifications occur in sperm DNA, which may be passed
onto offspring. Further studies need to be conducted in order to
determine the specific mechanism by which these modifications are
passed from father to offspring. Understanding these mechanisms would
provide more insight into preventative measures against FASDs and
similar congenital defects.
"Other epigenetic effects of paternal alcohol consumption
Paternal alcohol consumption has been implicated in additional
congenital disorders, presumably via epigenetic mechanisms. In an
epidemiological study by the Kaiser Foundation, the frequency and
severity of certain congenital abnormalities were correlated with
paternal alcohol consumption. For example, paternal alcohol
consumption was found to be positively associated with ventricular
septal defects in newborn children. Separate animal studies have also
shown that paternal alcohol consumption can lead to increased
susceptibility to Pseudomonas infection. The severity of this
increased susceptibility was found to be identical to that of animals
whose mothers consumed alcohol during pregnancy, suggesting that
paternal epigenetic alterations are as crucial to the development of
offspring as maternal ones. Overall, these studies imply that early
changes in a fathers lifestyle can decrease prevalence of congenital
disorders in his offspring."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4913293/
[3332]
Chang et al (2019) continued this interesting assault on male
exceptionalism with "Preconception paternal alcohol exposure exerts
sex-specific effects on offspring growth and long-term metabolic
programming" in which daddy mice were given 70-days of preconception
treatment with alcohol. Exposed males were then mated to six- to
eight-week-old females. At no point during these experiments were the
females ever exposed to the preconception treatments.
The difficulties of detecting such an effect in humans are all but
insurmountable. Where do you find a sufficient number of children of
sober mothers whose alcoholic father is no longer on the scene,
confounding the nature/nurture analysis? How much did the father drink
before the pregnancy? The Texas A&M University researchers list
the references:
"For example, clinical data can correlate paternal alcoholism with
negative impacts on child behavior and cognitive development. In
addition, clinical associations between paternal drinking and
increased rates of congenital abnormalities, as well as decreases in
infant birth weight and head circumference, have been reported.
However, in these studies, additional and often uncontrolled factors
such as nutrition, poor housing conditions, maternal stress, smoking,
and parental alcohol use all exert independent effects on child growth
and development. In this setting, it is virtually impossible to
identify a direct link between preconception paternal alcohol use and
child development."
However in the mice, with controlled conditions, the picture was
clear:
"Preconception paternal alcohol exposure induced a prolonged period
of fetal gestation and an increased incidence of intrauterine growth
restriction, which affected the male offspring to a greater extent
than the females. While the female offspring of ethanol-exposed males
were able to match the body weights of the controls within the first 2
weeks of postnatal life, male offspring continued to display an 11%
reduction in weight at 5 weeks of age and a 6% reduction at 8 weeks of
age. The observed growth deficits associated with insulin
hypersensitivity in the male offspring, while in contrast, females
displayed a modest lag in their glucose tolerance test. These
metabolic defects were associated with an up-regulation of genes
within the pro-fibrotic TGF-β signaling pathway and increased
levels of cellular hydroxyproline within the livers of the male
offspring. We observed suppressed cytokine profiles within the liver
and pancreas of both the male and female offspring, which correlated
with the up-regulation of genes in the LiverX/RetinoidX/FarnesoidX
receptor pathways. However, patterns of gene expression were highly
variable between the offspring of alcohol-exposed sires. In the adult
offspring of alcohol-exposed males, we did not observe any differences
in the allelic expression of Igf2 or any other imprinted genes.
"Conclusions
The impact of paternal alcohol use on child development is poorly
explored and represents a significant gap in our understanding of the
teratogenic effects of ethanol. Our studies implicate paternal
exposure history as an additional and important modifier of
alcohol-induced growth phenotypes and challenge the current
maternal-centric exposure paradigm."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6341619/
[3328]
2019 continued with "Parental alcohol consumption and the risk of
congenital heart diseases in offspring: An updated systematic review
and meta-analysis" from the Xiangya School of Public Health, Hunan, in
which paternal alcohol was associated with a nearly threefold greater
risk than maternal consumption:
"A total of 55 studies involving 41,747 CHD cases and 297,587
controls were identified. Overall, both maternal (odds ratio (OR) =
1.16; 95% confidence interval (CI): 1.05-1.27) and paternal (OR =
1.44; 95% CI: 1.19-1.74) alcohol exposures were significantly
associated with risk of total CHDs in offspring. Additionally, a
nonlinear dose-response relationship between parental alcohol exposure
and risk of total CHDs was observed. With an increase in parental
alcohol consumption, the risk of total CHDs in offspring also
gradually increases. For specific CHD phenotypes, a statistically
significant association was found between maternal alcohol consumption
and risk of tetralogy of fallot (OR = 1.20; 95% CI: 1.08-1.33).
Relevant heterogeneity moderators have been identified by subgroup
analysis, and sensitivity analysis yielded consistent results."
https://academic.oup.com/eurjpc/article-pdf/27/4/410/34258325/eurjpc0410.pdf
[3229]
This was duly reported by the European Society of Cardiology, who
write:
"Drinking alcohol three months before pregnancy (and during the first
trimester for mothers) was associated with a 44% raised risk of
congenital heart disease for fathers and 16% for mothers, compared to
not drinking. Binge drinking, defined as five or more drinks per
sitting, was related to a 52% higher likelihood of these birth defects
for men and 16% for women.
"Binge drinking by would-be parents is a high risk and dangerous
behaviour that not only may increase the chance of their baby being
born with a heart defect, but also greatly damages their own health,
said study author Dr Jiabi Qin, of Xiangya School of Public Health,
Central South University, Changsha, China.
"Dr Qin said the results suggest that when couples are trying for a
baby, men should not consume alcohol for at least six months before
fertilisation while women should stop alcohol one year before and
avoid it while pregnant.
"Congenital heart diseases are the most common birth defects, with
approximately 1.35 million babies affected every year. These
conditions can increase the likelihood of cardiovascular disease later
life, even after surgical treatment, and are the main cause of
perinatal death. Alcohol is a known teratogen and has been connected
with foetal alcohol spectrum disorder (FASD). Around one in four
children with FASD have congenital heart disease, indicating that
alcohol might also be implicated in these disorders.
"Previous studies investigating the link between alcohol and
congenital heart disease have focused on prospective mothers, with
inconclusive results. This is the first meta-analysis to examine the
role of paternal alcohol drinking."
https://www.escardio.org/The-ESC/Press-Office/Press-releases/Fathers-to-be-should-avoid-alcohol-six-months-before-conception
[3330]
Back with the maternal alcohol Flentke et al bring us up to 2024 with
"Alcohol exposure suppresses ribosome biogenesis and causes nucleolar
stress in cranial neural crest cells", in which the progeny of drunk
mummy zebra fish were examined in search of a mechanism involving
ribosome biogenesis, which turned out to be a successful
endeavour:
"Prenatal alcohol exposure (PAE) causes cognitive impairment and a
distinctive craniofacial dysmorphology, due in part to apoptotic
losses of the pluripotent cranial neural crest cells (CNCs) that form
facial bones and cartilage. We previously reported that PAE rapidly
represses expression of >70 ribosomal proteins (padj = 10-E47).
Ribosome dysbiogenesis causes nucleolar stress and activates
p53-MDM2-mediated apoptosis. Using primary avian CNCs and the murine
CNC line O9-1, we tested whether nucleolar stress and p53-MDM2
signaling mediates this apoptosis. We further tested whether
haploinsufficiency in genes that govern ribosome biogenesis, using a
blocking morpholino approach, synergizes with alcohol to worsen
craniofacial outcomes in a zebrafish model. In both avian and murine
CNCs, pharmacologically relevant alcohol exposure (20mM, 2hr) causes
the dissolution of nucleolar structures and the loss of rRNA
synthesis; this nucleolar stress persisted for 18-24hr. This was
followed by reduced proliferation, stabilization of nuclear p53, and
apoptosis that was prevented by overexpression of MDM2 or
dominant-negative p53. In zebrafish embryos, low-dose alcohol or
morpholinos directed against ribosomal proteins Rpl5a, Rpl11, and
Rps3a, the Tcof homolog Nolc1, or mdm2 separately caused modest
craniofacial malformations, whereas these blocking morpholinos
synergized with low-dose alcohol to reduce and even eliminate facial
elements. Similar results were obtained using a small molecule
inhibitor of RNA Polymerase 1, CX5461, whereas p53-blocking
morpholinos normalized craniofacial outcomes under high-dose alcohol.
Transcriptome analysis affirmed that alcohol suppressed the expression
of >150 genes essential for ribosome biogenesis. We conclude that
alcohol causes the apoptosis of CNCs, at least in part, by suppressing
ribosome biogenesis and invoking a nucleolar stress that initiates
their p53-MDM2 mediated apoptosis. We further note that the facial
deficits that typify PAE and some ribosomopathies share features
including reduced philtrum, upper lip, and epicanthal distance,
suggesting the facial deficits of PAE represent, in part, a
ribosomopathy."
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0304557
[3333]
2024 also saw a quantification of a threshold dose for paternal
alcohol use in F1 FASD, by Higgins et al at Texas A&M, in "Chronic
paternal alcohol exposures induce dose-dependent changes in offspring
craniofacial shape and symmetry":
"Procrustes ANOVA followed by canonical variant analysis of geometric
facial relationships revealed that Low-, Medium-, and High-dose
treatments each induced distinct changes in craniofacial shape and
symmetry. Our analyses identified a dose threshold between 1.543 and
2.321 g/kg/day. Below this threshold, preconception paternal alcohol
exposure induced changes in facial shape, including a right shift in
facial features. In contrast, above this threshold, paternal exposures
caused shifts in both shape and center, disrupting facial symmetry.
Consistent with previous clinical studies, changes in craniofacial
shape predominantly mapped to regions in the lower portion of the
face, including the mandible (lower jaw) and maxilla (upper jaw).
Notably, high-dose exposures also impacted the positioning of the
right eye. Our studies reveal that paternal alcohol use may be an
unrecognized factor contributing to the incidence and severity of
alcohol-related craniofacial defects, complicating diagnostics of
fetal alcohol spectrum disorders."
https://www.frontiersin.org/journals/cell-and-developmental-biology/articles/10.3389/fcell.2024.1415653/full
[3334]
To put this into context the following represent 10 grams of
alcohol.

https://responsibledrinking.eu/what-is-a-standard-drink-of-alcohol/
[3335]
For a 70kg man the threshold for more serious craniofacial effects in
his child would be 108.01 to 162.47 g/day, so this is between 11 and
16 standard European units.
Alcohol-related epigenetic effects do not stop with the next
generation, as explained in "Epigenetic mechanisms in alcohol- and
adversity-induced
developmental origins of neurobehavioral functioning" by Boschen et
al (2018):
Under "DNA methylation of neurodevelopmental and plasticity-related
genes" we learn:
"Genes related to neurodevelopment and HPA axis regulation are
commonly altered in both developmental stress and alcohol
models."
Under "Expression of epigenetic regulators":
"Another commonality between the consequences of early-life stress
and alcohol are the observed alterations in levels of epigenetic
regulators throughout the brain."
And under "DNA Methylation":
"Brain-derived neurotrophic factor (BDNF) is another growth factor
important for cell proliferation, dendritic outgrowth, and synapse
formation, particularly in the adult brain. Numerous studies have
demonstrated that development alcohol exposure causes long-term
changes to functional and anatomical measures linked to BDNF
signaling, including long-term potentiation (Puglia and Valenzuela,
2010), adult neurogenesis (Boehme et al., 2011; GilMohapel et al.,
2010; Hamilton et al., 2011; Klintsova et al., 2007), and dendritic
morphology (Berman et al., 1996; Boschen et al., 2016; Hamilton et
al., 2015; Hamilton et al., 2010; Redila and Christie, 2006; Whitcher
and Klintsova, 2008). Studies have demonstrated that Bdnf gene
expression is altered following developmental alcohol exposure in a
timing and region-specific manner (Caldwell et al., 2008; Feng et al.,
2005; Heaton et al., 2000; Heaton et al., 2003), though the diverse
models and methods of analysis used in these studies makes it
difficult to draw definitive conclusions. Epigenetic modification of
Bdnf has not been well studied in alcohol exposure models, despite
being a significant target of interest in prenatal stress research.
Bdnf exon I hypomethylation was reported 24 h following PD49 alcohol
exposure in the male rat hippocampus; this reduction in methylation
was correlated with increased exon I-driven Bdnf gene expression
(Boschen et al., 2015). However, by PD72, methylation status had
returned to control levels (Boschen et al., 2016). Bdnf and other
growth factors that could contribute to either delayed embryonic
growth or long-term deficits in neuroplasticity need to be further
investigated from an epigenetic perspective."
Under "Non-coding RNAs":
"Disruption of noncoding RNAs, such as miRNAs, can cause a wide range
of cellular or DNA damage, contributing to long-term deficits (Figure
1). miRNAs affect the production of protein products through
translational repression or degradation of the mRNA. In vivo and in
vitro models of FASD have identified numerous miRNAs that are impacted
by developmental alcohol exposure, including miR-9, miR-20a, miR-21,
miR-30, miR-103, miR-151, miR-153, miR-335, and miR-140-3p (Balaraman
et al., 2014; Balaraman et al., 2012; Guo et al., 2012; Ignacio et
al., 2014; Pappalardo-Carter et al., 2013; Pietrzykowski et al., 2008;
Sathyan et al., 2007; Soares et al., 2012; Tal et al., 2012; Wang et
al., 2009). In a study that examined the effects of prenatal stress on
miRNA expression, dams were administered daily restraint stress and
forced swimming from days 1218 of gestation (Zucchi et al., 2013).
This stressor disrupted maternal behavior, as reduced tail chasing
behavior was exhibited by dams exposed to stress. In the whole brains
of their newborn male offspring, 336 miRNAs were differentially
expressed. Notably, some of the same miRNAs were altered by prenatal
stress as have been mentioned in the developmental alcohol literature,
including miR-9, miR-20a, miR-103, and miR-151."
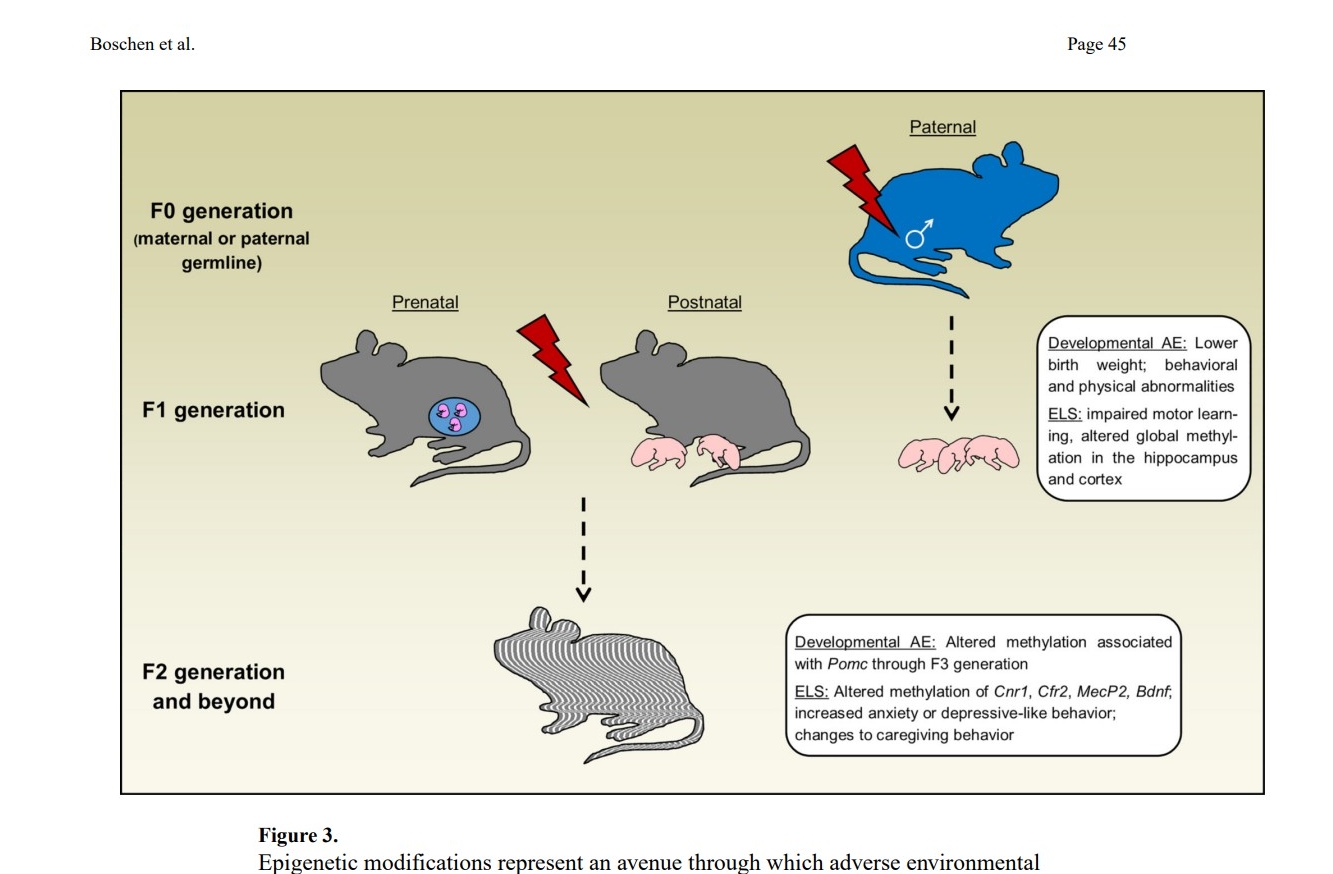
"Epigenetic modifications represent an avenue through which adverse
environmental conditions can affect generations beyond the animals
that were directly exposed via intergenerational and transgenerational
transmission. Epigenetic marks can be passed through the paternal
germline (F0) following preconception exposure to stress or alcohol,
resulting in physiological, behavioral, or altered levels of global
methylation in the offspring (F1). Exposure of a fetus (via exposure
of the F0 pregnant dam) or neonate (F1) to alcohol or stress affects
not only the directly exposed animal but also the developing germline.
Altered epigenetic marks can then be transmitted to animals that were
never exposed to the stressor or alcohol in the F2 generation and
beyond, resulting in changes to methylation associated with multiple
genes and epigenetic regulators and ppersistent behavioral
perturbations. AE: Alcohol exposure; ELS: Early life stress."
https://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC5856624&blobtype=pdf
[3337]
Portugalov and Akirav (2024) have the latest on the FAAH blocking
approach with "FAAH Inhibition Reverses Depressive-like Behavior and
Sex-Specific Neuroinflammatory Alterations Induced by Early Life
Stress":
"Early life stress (ELS) increases predisposition to major depressive
disorder (MDD), with neuroinflammation playing a crucial role. This
study investigated the long-term effects of the fatty acid amide
hydrolase (FAAH) inhibitor URB597 on ELS-induced depressive-like
behavior and messenger RNA (mRNA) of pro-inflammatory cytokines in the
medial prefrontal cortex (mPFC) and CA1 regions. We also assessed
whether these gene expression alterations were present at the onset of
URB597 treatment during late adolescence. ELS induced a
depressive-like phenotype in adult male and female rats, which was
reversed by URB597. In the mPFC, ELS downregulated nuclear factor
kappa B1 (nfκb1) in both sexes, while URB597 normalized this
expression exclusively in males. In females, ELS downregulated
interleukin (il) 6 and tumor necrosis factor alpha (tnfα) but
upregulated il1β and corticotropin-releasing factor (crf); URB597
normalized il6, il1β, and crf. In the CA1, ELS downregulated
il1β and tnfα in males and upregulated il1β expression
in females, which was reversed by URB597. Some of these effects began
in late adolescence, including mPFC-nfκb1 expression in both
sexes, mPFC-il6 and mPFC-il1β in females, CA1-il1β and
CA1-tnfα in males, and CA1-il1β in females. These findings
highlight URB597 as a therapeutic approach for reversing ELS-induced
depressive-like behavior by associating with changes in the gene
expression of neuroinflammatory cytokines, with notable sex
differences."
https://www.mdpi.com/2073-4409/13/22/1881
[3993]
The discrimination of the ZPPPD against subjects of early life stress
as overproducers of FAAH is further demonstrated by Demaili et al
(2023) in "Epigenetic (re)programming of gene expression changes of
CB1R and FAAH in the medial prefrontal cortex in response to early
life and adolescence stress exposure":
"Thus, the present study addressed the hypotheses that ELS and
adolescent stress differentially affect the expression of regulatory
elements of the endocannabinoid system, cannabinoid receptor 1 (CB1R)
and fatty acid amide hydrolase (FAAH) in the medial prefrontal cortex
(mPFC) of adult female rats. We also tested the hypothesis that the
proposed gene expression changes are epigenetically modulated via
altered DNA-methylation. The specific aims were to investigate if (i)
ELS and adolescent stress as single stressors induce changes in CB1R
and FAAH expression (ii) ELS exposure influences the effect of
adolescent stress on CB1R and FAAH expression, and (iii) if the
proposed gene expression changes are paralleled by changes of DNA
methylation. The following experimental groups were investigated: (1)
non-stressed controls (CON), (2) ELS exposure (ELS), (3) adolescent
stress exposure (forced swimming; FS), (4) ELS + FS exposure. We found
an up-regulation of CB1R expression in both single-stressor groups and
a reduction back to control levels in the ELS + FS group. An
up-regulation of FAAH expression was found only in the FS group. The
data indicate that ELS, i.e., stress during a very immature stage of
brain development, exerts a buffering programming effect on gene
expression changes induced by adolescent stress. The detected gene
expression changes were accompanied by altered DNA methylation
patterns in the promoter region of these genes, specifically, a
negative correlation of mean CB1R DNA methylation with gene expression
was found. Our results also indicate that ELS induces a long-term
(re)programming effect, characterized by CpG-site specific changes
within the promoter regions of the two genes that influence gene
expression changes in response to FS at adolescence."
https://www.frontiersin.org/journals/cellular-neuroscience/articles/10.3389/fncel.2023.1129946/full
[3994]
Meanwhile, according to Astley et al (1992):
"The association between fetal marijuana and/or alcohol exposure and
facial features resembling fetal alcohol syndrome was investigated in
a sample of 80 children. Standardized lateral and frontal facial
photographs were taken of 40 children, 5 to 7 years of age, whose
mothers reported frequent use of marijuana during the first trimester
of pregnancy and 40 children whose mothers reported no use of
marijuana during pregnancy. The marijuana-exposed and unexposed
children were group-matched on alcohol exposure prior to and during
pregnancy, sex, race, and age at the time of assessment. The
photographs were assessed clinically by a study staff dysmorphologist
and morphometrically by computerized landmark analysis. Fetal alcohol
syndrome-like facial features were not associated with prenatal
marijuana exposure in this study sample."
https://depts.washington.edu/fasdpn/pdfs/astley-1992.pdf
[3336]
No rescheduling of alcohol or changes have been made to the ZPPPD in
the light of these findings about ugliness.
I am obliged to the 28 February 2024 BBC article "Why alcohol is so
dangerous for young adults' brains":
"In the past, neural development was thought to stop in our early
teens, but a swathe of recent research shows that the adolescent brain
undergoes a complex rewiring that does not end until at least the age
of 25.
"The most important changes include a decline in 'grey matter' as the
brain prunes away the synapses that allow one cell to communicate with
another. At the same time, white matter long-distance connections
known as axons covered with an insulating fatty sheath tends to
proliferate. 'They are like the brain's super-highways,' says Lindsay
Squeglia, a neuropsychologist at the Medical University of South
Carolina. The result is a more efficient neural network that can
process information more quickly.
"The limbic system, involved with pleasure and reward, is the first
to mature. 'These areas are fully adult-like during adolescence,'
Squeglia explains. The prefrontal cortex, which is located behind the
forehead, is slower to ripen. This region is responsible for
higher-order thinking which includes emotional regulation,
decision-making, and self-control.
"The relative imbalance of these two regions' development can explain
why adolescents and young adults tend to be more risk-taking than
adults. 'A lot of people describe the adolescent brain as having a
fully developed gas pedal without brakes,' says Squeglia. And bathing
our neurons in alcohol which is known to release inhibition may only
amplify this thrill chasing. For particularly impetuous teenagers,
alcohol can create a vicious cycle of bad behaviour and delinquency.
'The more impulsive kids tend to drink more, and then drinking causes
more impulsivity,' says Squeglia.
"At high enough frequencies and volumes, adolescent drinking could
impair the brain's long-term development. Longitudinal studies show
that early drinking is associated with a more rapid decline in grey
matter, while the growth of the white matter is stunted. 'Those
super-highways aren't getting paved as much in kids who start
drinking,' says Squeglia.
"The consequences may not be immediately evident in cognitive tests;
in a young brain, the regions responsible for problem solving can work
a little bit harder to make up for the deficits. It cannot keep this
up forever, however. 'After multiple years of drinking, we see less
activation in the brain and poorer performance on these tests,' says
Squeglia.
"Early drinking can also take its toll on mental health, and
heightens the risk of alcohol abuse later in life. This is
particularly true for people who have a family history of alcoholism
the earlier they start, the greater their chances of developing a
drinking problem themselves. The genes associated with an advanced
risk of alcohol abuse seem to be most influential during this critical
period of brain development. 'And the longer that someone is able to
wait, the less likely these genes are going to come into play,' says
Squeglia."
https://www.bbc.com/future/article/20240228-how-alcohol-affects-teens-and-young-adults-brains
[4474]
But how many schizophrenics have a concrete reason to suspect their
genetic susceptibility?
It's not as if doctors in Slovenia are offering genetic screening to
see whether patients are likely to benefit or otherwise from THC.
For as the authors say,
"The widespread use of cannabis calls for a concerted effort into
increased understanding of both the positive and negative effects of
the drug."
But it seems they do not agree with themselves, for when it comes to
Figure 3
https://www.nature.com/articles/s41398-018-0137-3
[1899]
In 2010 it emerged from a study of brain volumes in schizophrenics
and non-schizophrenics tagged for the common functional polymorphism,
Val108/158Met:
"Across patients and controls, each copy of the COMT met allele was
associated on average with a 2.6% increase in right amygdala volume, a
3.8% increase in left amygdala volume and a 2.2% increase in right
hippocampus volume. There were no effects of COMT genotype on volumes
of the whole brain and prefrontal regions.
"Thus, the COMT Val108/158Met polymorphism was shown to influence
medial temporal lobe volumes in a linear-additive manner, mirroring
its effect on dopamine catabolism."
https://www.sciencedirect.com/science/article/abs/pii/S1053811909013354
[213]
However a 2018 attempt to link COMT variability to cannabis use in
psychotic cases was "unconvincing".
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5812637/
[214]
The results of Cobb Scott et al (2019) were fairly uneventful, even
in a sample with higher than usual levels of alcohol use and
psychopathology:
"Frequent cannabis use during adolescence has been associated with
alterations in brain structure. However, studies have featured
relatively inconsistent results, predominantly from small samples, and
few studies have examined less frequent users to shed light on
potential brain structure differences across levels of cannabis use.
In this study, high-resolution T1-weighted MRIs were obtained from 781
youth aged 1422 years who were studied as part of the Philadelphia
Neurodevelopmental Cohort. This sample included 147 cannabis users
(109 occasional [≤12 times per week] and 38 frequent [≥3 times
per week] users) and 634 cannabis non-users. Several structural
neuroimaging measures were examined in whole brain analyses, including
gray and white matter volumes, cortical thickness, and gray matter
density. Established procedures for stringent quality control were
conducted, and two automated neuroimaging software processing packages
were used to ensure robustness of results. There were no significant
differences by cannabis group in global or regional brain volumes,
cortical thickness, or gray matter density, and no significant group
by age interactions were found. Follow-up analyses indicated that
values of structural neuroimaging measures by cannabis group were
similar across regions, and any differences among groups were likely
of a small magnitude. In sum, structural brain metrics were largely
similar among adolescent and young adult cannabis users and non-users.
Our data converge with prior large-scale studies suggesting small or
limited associations between cannabis use and structural brain
measures in youth. Detailed studies of vulnerability to structural
brain alterations and longitudinal studies examining long-term risk
are clearly indicated."
But noting that:
"Previous studies with small samples were likely underpowered to
detect small magnitude effects, which could partially explain
variability in the literature. Our results converge with data from
larger samples of cannabis-using youth, which have found more limited
brain structural differences associated with cannabis than smaller
studies. For example, Weiland and colleagues compared 50 adolescent
daily users of cannabis to 50 demographically matched non-users,
replicating methods from an earlier study, and found non-significant
differences in volume, surface-based morphometry, and shape.
Similarly, in a sample of 439 adolescents, Thayer and colleagues found
no significant associations of past month cannabis use with brain
volume or measures of diffusivity after covarying for alcohol use
disorder symptoms. Our results extend these studies by probing effects
across levels of cannabis use and examining measures of cortical
thickness and gray matter density."
https://www.nature.com/articles/s41386-019-0347-2
[5401]
In the worrying-sounding "Grey Matter Volume Differences Associated
with Extremely Low Levels of Cannabis Use in Adolescence" from Orr et
al (2019) it turns out that:
"Preclinical evidence has consistently demonstrated a causal
relationship between cannabis exposure and changes to brain morphology
(for review, see Panlilio and Justinova, 2018). The human evidence,
however, has been variable reporting both increases and decreases in
brain volumes (Ashtari et al., 2011; Cousijn et al., 2012; Gilman et
al., 2014), no volume differences (Jager et al., 2007; Weiland et al.,
2015; Gillespie et al., 2018), and modest effect sizes (Weiland et
al., 2015). Factors including the age of cannabis use initiation,
comorbid substance use, and levels of use are believed to contribute
to variability in the human findings (Curran et al., 2016)."
...
"One study has reported differences in gray-matter density and shape
of the amygdala and nucleus accumbens in recreational cannabis users
(Gilman et al., 2014), but subsequent research has suggested that
these findings may be associated with alcohol (Weiland et al., 2015)
and nicotine (Gillespie et al., 2018) exposure in the cannabis
users."
...
"The eCB system mediates maturation-related neural reorganization
(Fernndez-Ruiz et al., 2000), which may place adolescents at
heightened vulnerability to structural brain effects of cannabis
exposure as adolescence is a time of rapid neural maturation (Rubino
and Parolaro, 2008). Consistent with this suggestion, those who
commenced cannabis use in adolescence typically show greater
structural brain differences than those who initiated use in adulthood
(Battistella et al., 2014; Lubman et al., 2015). These findings may
also have been influenced by the effects of other substances, however,
as one study comparing adolescent daily cannabis users with controls
matched for alcohol and nicotine use found no differences in
subcortical gray-matter density or morphology (Weiland et al.,
2015)."
...
"It is possible that cannabis, alcohol, and nicotine have
differential effects on brain morphometry; specifically, recreational
cannabis use has been associated with volume increases, whereas
alcohol has been associated with volume reductions. In the current
study, we matched the groups on alcohol and nicotine use and, within
the cannabis using group, neither alcohol nor nicotine use was
associated with individual differences in GMV, suggesting that the GMV
differences we report are associated with cannabis use."
https://www.jneurosci.org/content/39/10/1817
[3721]
Slovenia has not proposed banning alcohol on the grounds of reduced
brain volume. Of course it may be that Slovenians have a religious
belief in alcohol and reduced brain volume. So they consider
brain-expanding cannabis, even at extremely low levels, to be
heretical and a sin, considering their prior inaccurate impression
that cannabis was more, and not 114 times less [852], harmful than alcohol, if we exclude prohibition effects and the
sin. The Court is invited to compare the constitutionality of
exercising these opposing beliefs.
Even one or two units of alcohol per day reduce brain volume, isn't
that true?
"...the associations between alcohol intake and brain structure using
multimodal imaging data from 36,678 generally healthy middle-aged and
older adults from the UK Biobank, controlling for numerous potential
confounds. Consistent with prior literature, we find negative
associations between alcohol intake and brain macrostructure and
microstructure. Specifically, alcohol intake is negatively associated
with global brain volume measures, regional gray matter volumes, and
white matter microstructure. Here, we show that the negative
associations between alcohol intake and brain macrostructure and
microstructure are already apparent in individuals consuming an
average of only one to two daily alcohol units, and become stronger as
alcohol intake increases."
Reagan Wetherill, PhD, of the University of Pennsylvania Perelman
School of Medicine in Philadelphia and co-authors report an increase
from two alcohol units to three showed changes equivalent to aging 3.5
years, and
"A recent meta-analysis of individuals with AUD
(n = 433) showed lower gray matter volume (GMV) in the
corticostriatal-limbic circuits, including regions of the prefrontal
cortex, insula, superior temporal gyrus, striatum, thalamus, and
hippocampus compared to healthy controls (n = 498).
Notably, lower GMV in striatal, frontal, and thalamic regions was
associated with AUD duration or lifetime alcohol consumption. Although
alcohol consumption can produce global and regional tissue volume
changes, frontal regions are particularly associated with these
effects. Further, research suggests that the effects of alcohol
consumption on brain volume interact with the effects of aging."
https://www.nature.com/articles/s41467-022-28735-5
[1049]
On the other hand "Cannabis dose and age of onset of cannabis use did
not affect hippocampal volumes", according to a 2017 study of 20
"heavy cannbis users" by Koenders et al with an average 39 month
follow-up.
https://pmc.ncbi.nlm.nih.gov/articles/PMC5544121/
[3724]
Any study of brain volume which disregards the major confounder
tobacco is seriously compromised. Daniju et al (2022) found:
"Regular cannabis users who also smoked tobacco cigarettes showed
altered GMV patterns relative to controls. However, a similar pattern
of GMV differences was also seen between regular tobacco users that
did not use cannabis. Further research is needed to disentangle the
effects of cannabis and tobacco use on brain structure."
In other words, they didn't get the anti-cannabis result they were
hoping for, but they managed not to look at any cannabis users who did
not use tobacco.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9716493/
[3725]
When Snoop Dogg posted this photo comparison with tragic drunk
English footballer Paul Gascoigne...
...Gascoigne responded by challenging the rapper to a 12-round boxing
match. So this is not a scientific debate.
Another cause of brain shrinkage you won't hear much about is
antipsychotics.
In 2015 Vita et al reported:
"Longitudinal magnetic resonance imaging studies comparing changes in
the volume of cortical GM over time between patients with
schizophrenia and healthy control subjects published between January
1, 1983, and March 31, 2014, were analyzed. Hedges' g was calculated
for each study and volume changes from baseline to follow-up were
analyzed. Meta-regression statistics were applied to investigate the
role of potential moderators of the effect sizes.
"Results: Eighteen studies involving 1155 patients with schizophrenia
and 911 healthy control subjects were included. Over time, patients
with schizophrenia showed a significantly higher loss of total
cortical GM volume. This was related to cumulative antipsychotic
intake during the interval between scans in the whole study sample.
Subgroup meta-analyses of studies on patients treated with
second-generation antipsychotics and first-generation antipsychotics
revealed a different and contrasting moderating role of medication
intake on cortical GM changes: more progressive GM loss correlated
with higher mean daily antipsychotic intake in patients treated with
at least one first-generation antipsychotic and less progressive GM
loss with higher mean daily antipsychotic intake in patients treated
only with second-generation antipsychotics."
https://pubmed.ncbi.nlm.nih.gov/25802081/
[2161]
There are no laws against coffee are there?
You don't need a prescription to buy coffee?
There are no legal controls on how much coffee you can drink, are
there?
There are no roadside caffeine tests, are there?
And yet too much coffee is bad for you, would you agree?
According to the Independent March 3 2022:
"A father died after accidentally downing caffeine powder as strong
as 200 cups of coffee, an inquest heard.
"Personal trainer Thomas Mansfield, 29, ordered a 100g packet of
caffeine powder to make supplement drinks at his family home.
"But he accidentally made a mixture containing seven times the
recommended dose before he "necked" it.
and
"A post mortem found the caffeine per litre of blood in his system
was the equivalent of up to 200 cups of coffee.
"The inquest heard that death could be caused by significantly lower
levels than the amount he consumed."
His medical cause of death was given as caffeine toxicity.
https://www.independent.co.uk/news/uk/home-news/personal-trainer-dead-caffeine-drink-b2026650.html
[1056]
So with this limited human sample of 1 that puts caffeine in the
vicinity of nitrous oxide and at least five times more dangerous than
psilocybin, LSD and marijuana, referring to:
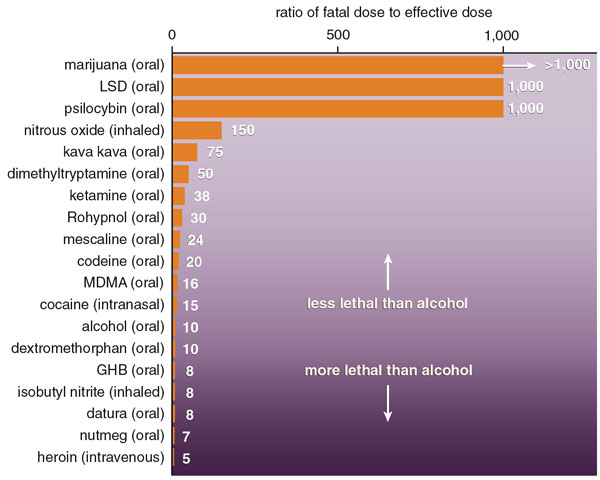
There were no calls for this product to be banned. There were no
murder or manslaughter charges to anyone who supplied or assisted
him?
Because we know that makes no sense, and would only makes things
worse.
But this case did not concern actual coffee, and we can barely
imagine consuming 200 cups of coffee.
What about chronic use?
There were inverse linear associations between habitual coffee
consumption and total brain (fully adjusted β per cup
−1.42, 95% CI −1.89, −0.94), grey matter (β
−0.91, 95% CI −1.20, −0.62), white matter (β
−0.51, 95% CI −0.83, −0.19) and hippocampal volumes
(β −0.01, 95% CI −0.02, −0.003), but no
evidence to support an association with white matter hyperintensity
(WMH) volume (β −0.01, 95% CI −0.07, 0.05). The
association between coffee consumption and dementia was non-linear
(Pnon-linearity = 0.0001), with evidence for higher odds
for non-coffee and decaffeinated coffee drinkers and those drinking
>6 cups/day, compared to light coffee drinkers. After full
covariate adjustment, consumption of >6 cups/day was associated
with 53% higher odds of dementia compared to consumption of 12
cups/day (fully adjusted OR 1.53, 95% CI 1.28, 1.83), with less
evidence for an association with stroke (OR 1.17, 95% CI 1.00, 1.37,
p = 0.055).
https://www.tandfonline.com/doi/abs/10.1080/1028415X.2021.1945858
[215]
[1-β = probability of a "true positive", i.e., correctly
rejecting the null hypothesis]
Do you think a campaign to ban coffee in Slovenia on health grounds
would have much public support or political traction?
You would probably agree that coffee brought from the Near East was
already established in eastern Europe by the 17th century?
Let's go back as far as we can in the drug war over coffee to see
what parallels we can find.
"The Greeks claim that a Greek opened the first coffeehouse in
Constantinople in 1475 at a place called Kiva Han, possibly in today's
Tahtakale district, although Turkish sources suggest coffee was only
brought to the city in 1517 after Sultan Selim I (r. 1512-1520)
conquered Egypt. Yet another story relates how the Ottoman governor of
Yemen, zdemir Paşa, had learned to love coffee while there and brought
coffee beans with him when he was called to Constantinople where he
introduced coffee drinking to Kanuni Sultan Sleyman (r.
1520-1566)."
Prohibition had little effect: the only trouble seemed to come from
religious people:
"A dispute broke out in Constantinople, as it had earlier in Cairo,
about drinking coffee. Purist Muslims wanted it banned because of its
stimulating nature and because it was an innovation. The chief
religious authority among the Ottomans during the reign of Sleyman and
his successor, Şeyhlislam Ebussuud issued a fatwa, or decree, against
drinking coffee. The year was 1543, according to Refik Ahmet Sevengil,
and ships had arrived bearing cargo of coffee beans. As a result of
the fatwa, the bags of beans were dumped in the sea. Over the years,
however, the prohibition was mostly ignored and the first coffeehouse
opened in Istanbul in 1555, according to Ottoman sources. And when
Bostanzade Mehmed Efendi became şeyhlislam toward the end of the 16th
century, he issued another fatwa, in poetic form no less, indicating
that suspicions about coffee were groundless."
https://www.hurriyetdailynews.com/coffee-and-coffeehouses-among-the-ottomans-76123
[892]
According to "Coffee and the Ottoman Social Sphere" by Marita Ervin
(2014):
"The most common and perhaps most accurate explanation accepted by
historians today is that coffee originated from the Sufi orders of
Yemen where caffeine was essential to religious practice. Sufis were
an untraditional sect of Islam whose methods were seen as erratic and
profane to both the Sunnis and Shiites. As opposed to practicing the
structured prayer indicative of traditional Islamic sects, the Sufis
consumed narcotics and danced fitfully to demonstrate their devotion
to Allah. Such a practice required the consumption of a drug that
could sustain them for many days. The Sufis lived on the fringes of
Ottoman society and coffee's connection to their orders stirred
speculation. Ktib Celebi, the famous Ottoman historian, described
coffee's first users as 'Certain sheiks, who lived with their
dervishes in the mountains of Yemen, used to crush and eat their
berries, which they called qalb wabūn, [] a cold dry food, suited to
the ascetic life and sedative of lust.' Celebi noted coffee's
connection with social outcasts and the need to repress the desire to
sin. Although Ottoman coffee struggled with its Sufi association, the
Sufi concept of developing a bond over a cup of coffee remained an
inherent quality of the beverage. Two men recognized the commercial
potential of coffee's cohesive abilities and harnessed it into the
development of the coffeehouse. After the coffee plant was extracted
from the Sufi lodges and brought to Istanbul by traders, two Syrians
merchants named Hakam and Shams opened the first coffeehouse in the
Ottoman capital in 1555."
For a time things were a roaring success:
"Swedish traveler Mouradgea D'Ohsson described over six-hundred
coffeehouses existing in Istanbul in the 1570s, only fifteen years
after coffee first arrived in Istanbul."
"Englishman George Sandys explained that the Turks enjoyed their
coffee 'as hot as they can
suffer it: black as soote, and tasting not much unlike it.'"
"Within the coffeehouse patrons were immersed in a safe atmosphere
that allowed them to engage in a means of creative self expression
through poetry. When poetry was not being recited urban storytellers
recounted traditional Ottoman tales and sophisticated stories that
catered to an academic audience. Customers were able to play games
such as chess and backgammon that involved strategy without the haram
gabling component. This wide range of stimulating coffeehouse
activities were not confined to a specific class. Ottoman historian
Ibramhimi Pechevi reported that there was no typical coffeehouse
customer outside of the fact that they were only Muslims and
predominantly male. He explained:
"'It reached such a point that all kinds of unemployed officers,
judges and professors all seeking preferment, and corner-sitters with
nothing to do proclaimed that there was no place like [the
coffeehouse] for pleasure and relaxation, and filled it until there
was no room to sit or stand. It became so famous that, besides the
holders of high offices, even great men could not refrain from coming
there.'"
https://soundideas.pugetsound.edu/cgi/viewcontent.cgi?article=1007&context=history_theses
[891]
The Coffea arabica plant is native to the Caffa region, in Abyssinia,
from which it arrived in Yemen and subsequently to Mecca and Medina,
where it took the name of Qahva.
In the Middle Ages, almost nothing was known about coffee in the
West; this aroma made its appearance in Europe in the sixteenth
century, and its widespread diffusion dates back to the defeat of the
Turkish troops, in siege of Vienna in 1683, followed in 1700 by its
introduction into South America.
People liked it.
But you'll know that some reacted with suspicion and fear, calling
the black beverage "amara invenzione di Satana"?
You'll know that they kicked up a religious debate about the
sinfulness of coffee users or, as we would characterise it today,
"coffee use disorder" and "coffee trafficking" were "crimes against
society".
Coffee, we could point out, can make certain susceptible groups
anxious or jittery?
We could say it increases heart rate?
And it is diuretic?
We could warn the public that caffeine blocks adenosine
receptors?
We could warn the public that caffeine interferes with sleep
cycles?
Could we reasonably say coffee is a drug which creates a
tolerance?
Would we be lying if we said there are some withdrawal
symptoms?
And yet we can find both responsible and irresponsible users?
And do we say coffee is like heroin.
So coffee, which we have decided is not a drug in legal parlance, is
a two-edged sword according to these drug criteria. If we care about
addiction, health effects and moral character coffee is both good and
bad. It is hard to draw a line.
And we assume we have a situation where the law reflects what we know
about such dangers.
Perhaps you know how this legal situation came to a head?
Do you happen to now which Pope was asked to decide on this
question?
Clement VIII.
And do you know the outcome?
He liked it, so it was alright for everyone to like it. Besides which
his friends was a-gonna make a lorra lorra money!
No fan of clemency, Clement executed and plundered from the get-go.
Menocchio, a miller who had found time to come up with the idea that
God was not eternal but had Himself once been created out of chaos,
and of panpsychist Giordano Bruno, a wandering intellectual (and whose
cosmopolitan views had taken him to London and Paris at a dangerous
time for nonconformists.
In England Bruno was liked by Henry VIII, may have spied on the
Catholic conspirators for Walsingham, and was mocked by the Archbishop
of Canterbury-to-be George Abbot for supporting "the opinion of
Copernicus that the earth did go round, and the heavens did stand
still; whereas in truth it was his own head which rather did run
round, and his brains did not stand still".
Bruno was imprisoned in Rome for a trial lasting seven years as the
charges were extended to include:
"holding opinions contrary to the Catholic faith and speaking against
it and its ministers;
holding opinions contrary to the Catholic faith about the Trinity,
divinity of Christ, and Incarnation;
holding opinions contrary to the Catholic faith pertaining to Jesus
as the Christ;
holding opinions contrary to the Catholic faith regarding the
virginity of Mary, mother of Jesus;
holding opinions contrary to the Catholic faith about both
Transubstantiation and the Mass;
claiming the existence of a plurality of worlds and their
eternity;
believing in metempsychosis and in the transmigration of the human
soul into brutes;
dealing in magics and divination" (Bruno was an expert in mnemonics
and did memory tricks).
Pope Clement took part in the trial personally. Bruno's parting shot
to the judges:
"Maiori forsan cum timore sententiam in me fertis quam ego accipiam
("Perhaps you pronounce this sentence against me with greater fear
than I receive it").
"He was turned over to the secular authorities. On 17 February 1600,
in the Campo de' Fiori (a central Roman market square), with his
'tongue imprisoned because of his wicked words', he was hung upside
down naked before finally being burned at the stake."
You might think that in an atmosphere like this coffee, from the
Muslim Arab world, would stand little chance. There may even be people
in Ptuj today who don't drink coffee because it is too foreign and
Islamic.
"When coffee first reached Rome, Christian priests believed that
Satan had invented coffee as a substitute for wine which Muslims were
not allowed to drink. Since wine was used in Christian practices such
as Holy Communion, priests thought that coffee must then be from the
Anti-Christ. Faced with strong beliefs that coffee was the drink of
Satan, Pope Clement VIII asked to try a cup before making a decision.
When he did, he blessed the drink as a Christian beverage, resulting
in massive imports of coffee to Italy and the Western world."
https://web.archive.org/web/20100601194012/http://www.professorshouse.com/food-beverage/beverages/coffee-facts-statistics.aspx
[882]
What an excellent idea. We should get (head of UNODC) Ghada Fathi
Waly to smoke some weed, maybe on a different day take a trip, so we
can all receive her seal of approval and relax.
And yet over in Constantinople, forty years after Bruno's execution
in 1600, with the accession of Ibrahim I the Ottoman attitudes to
coffee were softened slightly, but you were still at risk of execution
if caught drinking coffee. His Duterte-like predecessor Marud IV would
stalk the lowest taverns with a hundred pound broadsword and
decapitate offenders on the spot, besides using random people for
target practice with his bow and arrow. Ibrahim was more of a bag in
the river man, with 280 concubines drowned, besides the drug users.
Eventually he made such a mess of things the regime was in trouble,
and even his own mother approved his execution, the Ottomans' second
regicide.
https://en.wikipedia.org/wiki/Ibrahim_of_the_Ottoman_Empire#Deposition_and_execution
[883]
"According to one story, an Ottoman Grand Vizier [believed to be
Kprl, 892] secretly visited a coffeehouse in Istanbul.
"He observed that the people drinking alcohol would just get drunk
and sing and be jolly, whereas the people drinking coffee remained
sober and plotted against the government," says [author of The Devil's
Cup: Coffee, the Driving Force in History, Stewart] Allen."
https://www.npr.org/sections/thesalt/2012/01/10/144988133/drink-coffee-off-with-your-head
[884]
According to the French orientalist Antoine Galland,
"to his great dismay, 'he heard grave people discoursing seriously on
the affairs of the empire, blaming the ministry, and deciding matters
of the utmost importance. He likewise went into the taverns, where he
saw people singing, or talking only of their amours or exploits in
battle, being for the most part soldiers, whom he did not think it
convenient to deprive of this amusement.'' But he had the coffeehouses
closed for a time.'" [892]
All of which brings us to the germane question in this trial, which
is whether there is any difference between the sixteenth and
twenty-first century legal doctrine and procedure on the question of
principle whether the formulation of philosophical or religious or
political opinions supposedly contrary to orthodoxy provides
sufficient basis for the prosecution, trial, sentencing or execution
of a thinker.
It's not the what, but the why. Over and over we see the same pattern
repeated: an establishment looking for enemies, a novel drug culture
with anti-establishment ideas, a prohibition widely ignored, jealous
rivals e.g. mosques where "imams and expounders of the law were left
to keep company with their beards" [892], a disproportionate crackdown with opportunities for plunder, and
the risk of potentially fatal consequences from the authorities.
For would the public health have been improved if Pope Clement had
hated coffee, or refused to experience it or listen to its supporters?
He did not know what he did not know. The situation for coffee users
ever since would be analogous to the situation of the Defendant, while
a certain proportion of the population would be deprived of legal
access to life-extending goods, as described in
"The impact of coffee subtypes on incident cardiovascular disease,
arrhythmias, and mortality: long-term outcomes from the UK
Biobank"
by
Chieng et al (2022):
"Coffee subtypes were defined as decaffeinated, ground, and instant,
then divided into 0, <1, 1, 23, 45, and >5 cups/day, and
compared with non-drinkers. Cardiovascular disease included coronary
heart disease, cardiac failure, and ischaemic stroke. Cox regression
modelling with hazard ratios (HRs) assessed associations with incident
arrhythmia, CVD, and mortality. Outcomes were determined through ICD
codes and death records. A total of 449 563 participants (median 58
years, 55.3% females) were followed over 12.5 0.7 years. Ground and
instant coffee consumption was associated with a significant reduction
in arrhythmia at 15 cups/day but not for decaffeinated coffee. The
lowest risk was 45 cups/day for ground coffee [HR 0.83, confidence
interval (CI) 0.760.91, P < 0.0001] and 23 cups/day for instant
coffee (HR 0.88, CI 0.850.92, P < 0.0001). All coffee subtypes were
associated with a reduction in incident CVD (the lowest risk was
23 cups/day for decaffeinated, P = 0.0093; ground, P < 0.0001; and
instant coffee, P < 0.0001) vs. non-drinkers. All-cause mortality
was significantly reduced for all coffee subtypes, with the greatest
risk reduction seen with 23 cups/day for decaffeinated (HR 0.86, CI
0.810.91, P < 0.0001); ground (HR 0.73, CI 0.690.78, P <
0.0001); and instant coffee (HR 0.89, CI 0.860.93, P < 0.0001).
"Conclusion
Decaffeinated, ground, and instant coffee, particularly at
23 cups/day, were associated with significant reductions in incident
CVD and mortality. Ground and instant but not decaffeinated coffee was
associated with reduced arrhythmia."
https://academic.oup.com/eurjpc/article/29/17/2240/6704995?login=false
[5043]
Drug interdiction is one method by which rule by strength in a
chaotic society comes to be legally somatized. But even incomplete,
the cure for a largely imaginary disease is more immoral than the
morally neutral problem, hellishly portrayed by supporters of
prohibition.
The source of the word "addiction" comes from the Latin addictus: in
Roman society you could be assigned to someone as a slave if you could
not pay a debt. America's jails have sent marijuana prisoners by the
thousand to the chicken factory. What morality is this?
Being black and disproportionately arrested already, the American
prisoner is no less a slave than his Roman forbear, and this poultry
slavery is the successor to cotton slavery:
"Cotton production dominated the [Georgia] region up until the
postwar period. During this time, poultry production remained small
scale, localized, and was considered "women's work," a common practice
among white and Black households. Yet, in the crisis of the Great
Depression, white landowning farmers and merchants in Northeast
Georgia took over the industry and its profits. This takeover was
structured along the preexisting crop lien system used in the
overproduction of cotton that previously dominated the region.
Racially discriminatory state interventions under the Agricultural
Adjustment Act worked together with an agricultural credit system and
the consolidation of white-only farmer cooperatives to create
structural barriers to commercial poultry production for Black and
poor white sharecroppers and tenant farmers. These programs subsidized
cotton farmers to idle land and displace farm labor. In some cases,
this quite literally meant replacing the tenant house with the chicken
house.
"Cotton capital, built on the labor of enslaved people in the South,
was mobilized directly and indirectly into the growing poultry
industry, with cotton farmer cooperatives collectively shifting to
poultry production. After this initial takeoff, the Second World War
offered up a second major boost in 1944 when the War Food
Administration reserved all the chicken produced from seven counties
in north Georgia. This guaranteed capital allowed new forms of
vertical integration, led by poultry industry innovators John W.
Tyson, Jesse Jewell, and D. W. Brooks. This model of ownership,
reliant on bigger farms and highly industrialized agriculture,
restructured the rural South for the creation of cheap food. Cotton's
transformation, coupled with poultry's takeoff, enabled the 'selling
of the South' primed for low-wage, antilabor industrial growth. The
poultry industry thrived off the movement of farmworkers into
processing plants. Organized abandonment produced the poultry capital
of the world through racialized forms of dispossession and
displacement, exclusionary federal loans, purchasing guarantees, and
private industry integration at home, bolstered through war
imperialism abroad."
https://monthlyreview.org/2020/07/01/poultry-and-prisons/
[886]
Agro-slavery had continued after the Civil War in America:
"While the 13th Amendment abolished slavery and involuntary
servitude, it carved out a loophole that allowed for the exploitation
of incarcerated people, who were then and now, disproportionately
Black.
"The amendment abolished slavery and involuntary, 'except as
punishment for crime whereof the party shall have been duly
convicted.' Prisoners men, women, and hundreds of children as young as
6 or 7 were then leased to private farmers and business owners who'd
previously depended on cheap labor supplied by slaves."
"The 13th Amendment continues to permit the enslavement of prisoners,
who are still required to work for little or no pay in various public
and private industries. In 2010, a federal court held that 'prisoners
have no enforceable right to be paid for their work under the
Constitution.' Yet, across the country, prison labor remains essential
to running prisons and services beyond prison walls. They cook and
clean, work in fields, manufacturing warehouses, and call centers,
fight wildfires, do commercial laundry, make masks and hand sanitizer,
sometimes for as little as two cents an hour if anything often under
threat of punishment."
https://innocenceproject.org/parchman-farm-prison-mississippi-history/
[889]
In these historical encounters between hardline rulers and the bete
noir substances of their time, we perceive the successful leaders
psychotic, and/or needed to be perceived as psychotic, to instil fear
in the greatest number for reasons which make no sense today, and
probably didn't then.
Unlike their papal counterparts, Sultans Mehmet III, Marud IV and
Ibrahim I certainly didn't believe coffee was Satan's drink.
Clement, whose influence on coffee is debated, was typically
motivated by greed and profit. But heresy, not drug use, was the
expedient and well-understood target for the prohibition of the era.
With no antipopes to deal with and a big tourism jubilee to do, coffee
got the official western European theological thumbs up. And the rest
is history.
Marijuana convictions, fuelled by the propaganda of a xenophobic and
war-drum-beating media, supply an economical workforce to the poultry
industry.
Is this a credible problem or an appropriate approach to its
solution?
Like Nixon according to Erlichman, it wasn't reallly about drugs at
all.
"In Murad's Istanbul, religious leaders preached on street corners
that coffee would inspire indecent behavior, paralleling the ZPPPD's
blanket appeal to "appropriateness". As the bean moved west into
Europe, physicians rallied against it, claiming that coffee would 'dry
up the cerebrospinal fluid' and cause paralysis."
Thus in England in 1674, The Womens [sic] Petition Against Coffee
spoke of their horror:
"... the Excessive use of that Newfangled, Abominable, Heathenish
Liquor called COFFEE, which Riffling Nature of her Choicest Treasures,
and Drying up the Radical Moisture, has so Eunucht our Husbands that
they are become as unfruitful as those Desarts whence that unhappy
Berry is said to be brought."
This has been debunked as recently as 2018. In 21,403 men aged
40-75:
"No significant differences were identified for patients with
incident ED after comparing highest (≥4 cups/day) with lowest (0
cups/day) categories of total (hazard ratio (HR) = 1.00, 95%
confidence interval (CI): 0.90, 1.11) and regular coffee intakes (HR =
1.00, 95% CI: 0.89, 1.13)."
https://pubmed.ncbi.nlm.nih.gov/29020139/
[887]
But the real concern in the reign of Charles II was not
physiological, but political. And so it did not sound much like
impotence was the problem when a year later, in 1675, a royal edict
stated that coffeehouses "have produced very evil and dangerous
effects," and were also a "disturbance of the peace and quiet
realm."
"King Charles II issued an order to shut down all coffeehouses after
he traced some clever but seditious poetry to them. The backlash was
throne-shaking. In just 11 days, Charles reversed his ruling."
"'I think maybe he recalled that they had beheaded his father,'
[author of Uncommon Grounds: The History of Coffee and How It
Transformed Our World, Mark] Pendergrast says. "He didn't want to stir
up too much trouble."
England's newly-restored monarch faced a balancing act:
"On the one hand, by 1685, the duties collected on the goods sold by
coffee houses amounted to four percent of all of England's neat excise
produce, proving incredibly profitable to the crown. One the other
hand, however, Charles' throne still remained on slippery grounds, and
the threat that the coffeehouses posed was impossible to ignore.
Charles was very much aware that dissenting groups such as Thomas
Harrington's republican Rota Club was meeting a Mile' Coffeehouse in
London. There was also a belief among the elite of London that
dissenters were just plain associated with coffeehouse culture in
general, which made them want to squash the threat to the Restoration.
Coffeehouses were thus sometimes suppressed, and duties on the goods
they sold were increased."
However:
"Charles II failure to disrput the coffeehouse culture of free
converse and ideas was an indication of England's ability to progress
out of the shadow of its despotic monarchs and claim civil liberties
for the common person."

Here's a reproduction of a letterbox used at
"Button's Coffee House: Located on Russell Street in Covent Garden.
Also known as The Lion's Head Letter Box because patrons could drop of
pieces of their writing there to be published in the local newspaper
The Guardian."
https://sites.udel.edu/britlitwiki/the-coffeehouse-culture/
[885]
Well we all know how the story ended. Mormons don't drink coffee.
Everyone else can buy coffee, at any age, in any quantity, and the
Guardian still causes trouble occasionally.
Do you think if cannabis had arrived in Slovenia before other
now-legal drugs, the situation might now be reversed?
Which foods and medicines arrive where first is a matter of a mixture
of climatic, evolutionary, historical and geographical circumstances,
would you agree?
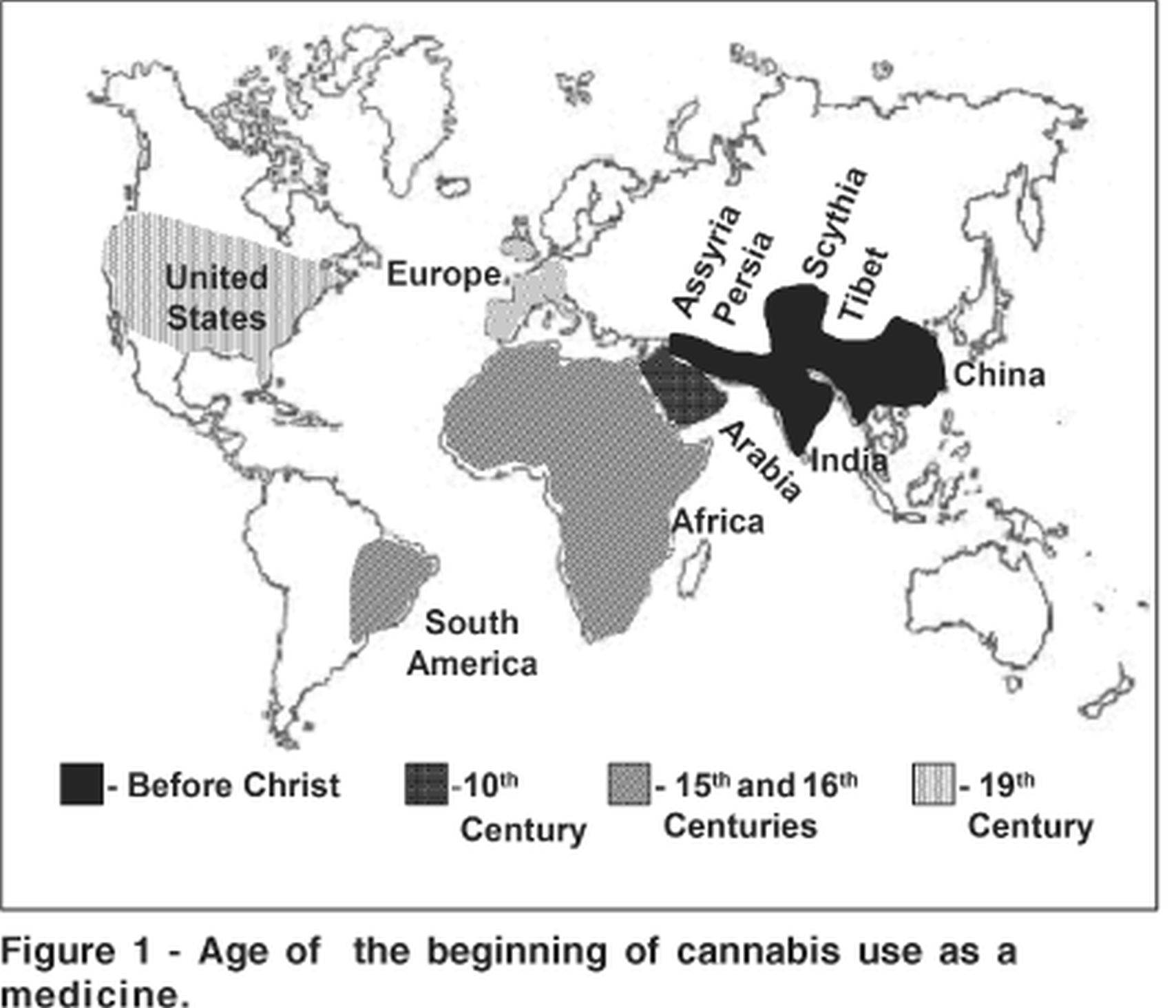
Let's just cannabis had arrived before coffee or alcohol. Would the
authorities today be saying, well, just because we made this mistake
legalising cannabis, it was a very long time ago, and we all use
cannabis now and banning it would be too unpopular?
In this scenario where cannabis came first, wouldn't the authorities
conclude that allowing the newcomers coffee or alcohol would only be
adding to our morbidity, and these should remain illegal and
prosecution used as a source of income for the judiciary and
government?
If you knew back then that 40 cups of coffee would stand a 50% chance
of killing you, that would finish legalisation of coffee
completely?
Gang wars might ensue. In 1777, Frederick the Great of Prussia issued
a manifesto claiming beer's superiority over coffee. He argued that
coffee interfered with the country's beer consumption, and royally
urged Prussians to begin the day properly. "His Majesty was brought up
on beer," he proclamation read. Sniffer troops were deployed across
Prussia.
"The Kingdom of Yugoslavia ratified the International Opium
Convention on 4 September 1929. The first law to sanction drug abuse
was the Criminal Code of the Kingdom of Serbs, Croats and Slovenes
passed on 27 January 1929 and which entered into force on 1 January
1930."
However Wikipedia also advises that King Alexander I renamed the
Kingdom of Serbs, Croats and Slovenes to the Kingdom of Yugoslavia on
6 January 1929.
So cannabis was first swept into this phoney "narcotics" grouping
11411 days before the UN Single Convention, and you could get '"a
prison sentence of up to 6 months for "serving" narcotic drugs in the
section "Crimes against Public Health"'
https://en.wikipedia.org/wiki/Cannabis_in_Kosovo
[216]
What the law was in the intervening years between 1 January 1930 and
1 January 2000 is somewhat of a mystery to this Defendant. However it
is surely undisputed that continuity existed in some form up to and
after the SCND.
Some of the effects of psychedelics are a kind of opposite to ADHD,
as they enhance traits such as mindfulness and empathy. Therefore
psychedelics like LSD tend to reduce crime because they increase
awareness of the victim, where there is one. In support of these
assertions are examinations of LSD effects in ADHD individuals.
Haijen et al at the Department of Neuropsychology and
Psychopharmacology, Faculty of Psychology and Neuroscience, Maastricht
University, studied "Trait mindfulness and personality characteristics
in a microdosing ADHD sample: a naturalistic prospective survey study"
(2023):
"Background: Microdosing (MD), repeatedly taking psychedelics in
small, non-hallucinogenic amounts, has been practiced by individuals
to relieve attention deficit hyperactivity disorder (ADHD) symptoms.
Generally, adults diagnosed with ADHD have lower levels of mindfulness
and differ in personality structure from non-ADHD adults. How MD
affects mindfulness and personality in adults with ADHD remains
unexplored.
"Aim: This study aimed to investigate the effects of 4 weeks
of MD on mindfulness and personality traits in adults diagnosed with
ADHD and those experiencing severe ADHD symptoms. It was expected that
mindfulness and the personality traits conscientiousness,
extraversion, agreeableness, and openness would increase and
neuroticism would decrease after 4 weeks of MD compared to
baseline. It was explored if using conventional ADHD medication
alongside MD and/or having comorbidities influenced MD-induced
effects.
"Methods: An online prospective naturalistic design was used to
measure participants before MD initiation and 2 and 4 weeks
later. Validated self-report measures were used assessing mindfulness
(15-item Five Facet Mindfulness Questionnaire) and personality traits
(10-item version of the Big Five Inventory) at three time
points.
"Results: The sample included n = 233,
n = 66, and n = 44 participants at the
three time points, respectively. Trait mindfulness, specifically
description and non-judging of inner experience, was increased, and
neuroticism was decreased after 4 weeks of MD compared to
baseline. The remaining personality traits remained unchanged. Using
conventional medication and/or having comorbid diagnoses did not
change the MD-induced effects on mindfulness and personality traits
after 4 weeks.
"Conclusion: MD induced changes in otherwise stable traits. Future
placebo-controlled studies are warranted to confirm whether these
changes occur in a controlled setting."
They explain:
"Mindfulness can broadly be divided into two dimensions:
self-regulation of attention and acceptance. First, self-regulation of
attention is characterized by attending, observing, and becoming aware
of ones thoughts, feelings, and sensations without getting caught in
ruminative thought streams. Mindfulness facets that belong to this
domain include observation, description, and acting with awareness.
Second, the acceptance domain involves taking an open, and accepting
stance toward ones observed experience, thereby inhibiting emotional
impulsive responses to whatever is observed. Mindfulness facets that
belong to this domain include non-judging of inner experience and
non-reactivity to inner experience. Generally, individuals diagnosed
with ADHD scored on average lower on trait mindfulness compared to
individuals without an ADHD diagnosis. Interestingly, enhanced levels
of mindfulness have been reported after MD and mindfulness scores were
higher in current and former microdosers compared to MD-nave controls.
Though one prospective (survey) study investigating adults (excluding
individuals with mood, anxiety, substance use, psychotic or
dissociative disorders) did not find a change in mindfulness scores
after MD, and another prospective study investigating a general
population sample could not attribute changes to MD solely. However,
the effects of MD on mindfulness in individuals diagnosed with ADHD,
or individuals experiencing severe ADHD symptoms, have not been
investigated yet."
A bit more about the parameters:
"Mindfulness was strongly and positively related to conscientiousness
(i.e., being well-organized, responsible, and efficient) and
negatively related to neuroticism (i.e., negative affectivity and
emotionally unstable). While the relationships between mindfulness and
conscientiousness and neuroticism have been a consistent finding, the
relationships between mindfulness and the other personality traits
agreeableness (i.e., compromising with, and trusting others),
extraversion (i.e., positive emotionality and socially engaged), and
openness (i.e., curious and willing to explore new experiences) were
overall positive, yet less strong. Individuals diagnosed with ADHD
score generally lower on conscientiousness and higher on neuroticism
compared to controls. Though the associations between ADHD and
extraversion and agreeableness are less strong, both traits tend to be
lower in ADHD. Openness is generally unrelated to ADHD. Interestingly,
openmindesness (i.e., openness) was higher and negative emotionality
(i.e., neuroticism) was lower in current and former microdosers
compared to MD-nave controls. Also, a qualitative interview study
reported that participants experienced increases in openness and
extraversion following MD, although no explicit mention of other
personality traits was made."
https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1233585/full
[4249]
However inconclusive researchers would like their results to be, they
do not support a hypothesis that microdosing, or normal doses, of
classical psychedelics, reduce conscientiousness towards, or empathy
with, others.
Since these prosocial traits are evidently lacking in criminal
behaviour, the only criminality associated with psychedelics is the
criminality of their criminalization. In short, the ZPPPD is a
pro-crime law!
Anyway, the authorities cannot be as bothered about crime as they
claim. Although Spencer (1963) declared in the British Journal of
Psychiatry without further explanation his rather confused opinion
that sensory hyperacuity was of "no therapeutic value" he wrote that
LSD was able
"...to bring into consciousness repressed traumatic experiences and
relationships suffered by the patient during childhood, such as those
of parental rejection and hostility, sexual assaults, the sense of
loneliness and impending doom engendered by inhalant
anaesthetics."
The mysterious paradox of catharsis unconnected with consciousness
deepened as
"LSD appeared to be unique in the ease with which under its influence
these deeply repressed memories could be recovered, and analysts using
the drug in relatively small doses found that it would produce in one
or two sessions unconscious material which would normally only be
recovered after some months of analysis."
https://scispace.com/papers/permissive-group-therapy-with-lysergic-acid-diethylamide-39q8clxg7v
[5642]
They meant well, but the explanation may simply be that the
"therapists" weren't tripping themselves, with the failure to
communicate being the reason why they were still puzzling over why
higher doses "were also the only doses where a statistically
significant reduction in symptoms after four weeks was found" [5559,
5560] 73 years later.
This particular way of reducing crime soon became a crime. Possibly
psychologists were worried they wouldn't have enough to do, as the
effects on Slovenia's national religion were devastating. Hendricks et
al (2014) were able to find processes by which "Hallucinogen use
predicts reduced recidivism among substance-involved offenders under
community corrections supervision":
"In this longitudinal study, we examined the relationship between
naturalistic hallucinogen use and recidivism among individuals under
community corrections supervision with a history of substance
involvement (n=25,622). We found that hallucinogen use predicted a
reduced likelihood of supervision failure (e.g. noncompliance with
legal requirements including alcohol and other drug use) while
controlling for an array of potential confounding factors (odds ratio
(OR)=0.60 (0.46, 0.79)). Our results suggest that hallucinogens may
promote alcohol and other drug abstinence and prosocial behavior in a
population with high rates of recidivism."
https://www.ovid.com/journals/jpsyc/abstract/10.1177/0269881113513851~hallucinogen-use-predicts-reduced-recidivism-among?redirectionsource=fulltextview
[5643]
Worse yet, the patients were threatening to gang together and
dispense with the pointless psychotherapists altogether. According to
Trope et al (2019)
"...participants from recent psychedelic-assisted individual
psychotherapy trials have repeatedly requested to meet other
participants (Bossis 2015; Bradberry et al. 2017) and have attested to
the importance of these connections for corroborating often intense,
difficult-to-describe, psychedelic experiences and reinforcing their
beneficial effects (Bradberry et al. 2017). This echoes the clinical
impression of early researchers that group involvement, whether in
mutual aid groups like Alcoholics Anonymous or formal group therapy,
could help solidify therapeutic gains by extending the intrapsychic
experiences of high-dose psychedelic sessions into the interpersonal
relationships of the group setting (Osmond et al. 1967)."
Numerous pre-prohibition studies are cited, for example one by Sven E
Jensen in a Saskatchewan mental hospital based around Alcoholics
Anonymous in 1962, as if alcoholism and mental illness were somehow
connected:
"35 patients received the group therapy and AA components without the
LSD session, and 45 'controls' received only treatment-as-usual in the
hospital during the same time period. Follow-up data obtained 6-18
months after discharge revealed that in the LSD condition (n=58), 34
remained sober and 7 were considered improved ('drinking definitely
less than before'). Of those who received group components without LSD
(n=35), 4 were sober and 4 were improved. Of the controls (n=45), 7
were sober and 3 improved. The increased proportion of sobriety or
improvement in the LSD condition was reported as statistically
significant compared to the two control arms."
https://escholarship.org/content/qt90n3z820/qt90n3z820.pdf
[5644]
Another pre-prohibition study, by Mogar and Savage (1964), reported
"Personality change associated with psychedelic (LSD) therapy":
"MMPI data are presented which were obtained from 60 patients prior
to, 2 mo. after, and 6 mo. after a brief psychotherapeutic program
culminating in a single, large dose LSD session. While all sub-groups
show significant positive changes at 2 mo., some patients manifest a
tendency towards regression while others either consolidate initial
gains or display further improvement at 6 mo. The results indicated
that the nature, magnitude, and stability of changes following a
psychedelic experience were related to personality variables, severity
of illness and modal defense patterns."
https://psycnet.apa.org/buy/1966-01700-001
[5649]
Of course alcohol cannot cause crime because it is legal.
Conscientiousness was another threat to crime proliferation and
employment in the justice and analysis industries. Long-term
conscientiousness was elevated with 200 μg of LSD in a 2024 study
by Holze et al:
"This finding aligns with the high proportion of people in both
trials who rated the psychedelic experience as among the most
meaningful experiences in life and is consistent with studies in
healthy volunteers, which also consistently demonstrated enduring
positive effects. Healthy participants attributed positive life
changes to their psychedelic experiences, mirroring findings from
therapeutic studies. Notably, research in healthy participants reports
shifts in personality traits, particularly an increase in the trait
openness, but changes in agreeableness and conscientiousness have also
been observed." [3376]
Scientists have even discovered that tripping in prison might not be
the best venue for a transformational experience. Reporting on
psychedelic assisted therapy (PAT) - elsewhere found to be no more
effective than just plain old psychedelics without the kind of
observation through which the dull live vicariously through the more
exciting lives of the less innocent - Tereza Dlestikova (2025) advises
that:
"The paper contends that community-based, post-release settings are
more appropriate and ethically defensible for PAT delivery than
correctional institutions. "
https://www.sciencedirect.com/science/article/abs/pii/S0955395925003639
[5646]
Since ADHD often manifests itself in behaviour resembling an angry
toddler, it is pertinent to ask if age and experience, as a function
of heightened depth of awareness, really does bring wisdom. Those of
us who have survived to make such an assessment will be unsurprised to
see "Age increases brain complexity" was confirmed, by Anokhin et al
(1996).
"This study investigated age-related changes in the human brain
function using both traditional EEG analysis (power spectra) and the
correlation dimension, a measure reflecting the complexity of EEG
dynamics and, probably, the complexity of neurophysiological processes
generating the EEG. Assuming that the accumulation of individual
experience is determined by the formation of functionally related
groups of neurons showing a repetitive synchronous activation (cell
assemblies), an increase in the number of such independently
oscillating cortical cell assemblies can be expected, despite a
decline of some metabolic and memory functions with normal ageing.
Thus, the wisdom of old age may find its neurophysiological basis in
greater complexity of brain dynamics compared to young ages. The
experimental hypothesis was that EEG dimension steadily increases with
age. In order to test this hypothesis the resting EEGs of 5 age groups
from 7 to 60 were analysed. The results confirm the hypothesis: after
a jump in the brain dynamics complexity during puberty a linear
increase with age is observed. During maturation (725 years), the
maximum gain in complexity occurs over the frontal associative
cortex."
https://www.sciencedirect.com/science/article/abs/pii/0921884X96955733
[4250]
Martin and Nichols (2016) report "Psychedelics Recruit Multiple
Cellular Types and Produce Complex Transcriptional Responses Within
the Brain" and
"...provide evidence that a small subset of 5-HT2A-expressing
excitatory neurons is directly activated by psychedelics and
subsequently recruits other select cell types including subpopulations
of inhibitory somatostatin and parvalbumin GABAergic interneurons, as
well as astrocytes, to produce distinct and regional responses. To
gather data regarding the response of specific neuronal populations,
we developed methodology for fluorescence-activated cell sorting
(FACS) to segregate and enrich specific cellular subtypes in the
brain. These methods allow for robust neuronal sorting based on
cytoplasmic epitopes followed by downstream nucleic acid analysis,
expanding the utility of FACS in neuroscience research."
https://www.thelancet.com/article/S2352-3964(16)30406-6/fulltext
[3723]
"Can Synaptic Loss Explain Cortical Thinning in Schizophrenia?" ask
Sapienza et al (2025):
"Kassem and colleagues, by combining structural MRI and confocal
microscopy, demonstrated that stressed mice showed gray matter losses
of 10 and 15% in the anterior cingulate cortex (ACC) and hippocampus,
coupled with a loss of synaptic spine density of up to 60% but no
changes in the number or volumes of the somas of neurons, astrocytes,
or oligodendrocytes. Moreover, there was a strong linear relationship
between dendritic volume loss and MRI-estimated gray matter volume
loss. A similar technique was used by Keifer and colleagues in a study
on the auditory fear-conditioning paradigm in mice to investigate its
effects on different cortical areas. They found increased gray matter
voxel intensity in several brain regions compared to the controls.
Focusing on the auditory cortex, they described concurrent increases
in dendritic spine density with a positive correlation between
dendritic spine density and gray matter voxel intensity. Taken
together, these preclinical findings indicate that synaptic changes
could contribute at least partially to cortical thinning and
neurostructural alterations seen in schizophrenia, despite not proving
such a relationship."
https://pmc.ncbi.nlm.nih.gov/articles/PMC12469418/
[5561]
Even "Cannabidiol reverses microglia activation and loss of
parvalbumin
interneurons and perineuronal nets in a mouse model of schizophrenia".
Da Silva et al (2025) explain:
"Our group has reported that repeated CBD treatment prevented and
reversed the social and cognitive impairments in a mouse model of SCZ
based on chronic treatment with the [glutamate N-methyl-d-aspartate
receptor] NMDAR antagonist MK-801. Also, CBD, similar to the
second-generation antipsychotic clozapine, prevented the decrease in
the number of [parvalbumin-positive] PV+ interneurons in the PFC."
"Most of the PV+ interneurons in the brain are surrounded by the
perineuronal nets (PNNs), a specialized extracellular matrix that
aggregates around the neuronal soma and is directly involved in the
regulation of PV+ interneurons synaptic plasticity, as well as in
their protection against oxidative and metabolic damage. PNNs mature
gradually, in an experience-dependent manner, during the maturation of
neural circuits in early adulthood, coinciding with the age of SCZ
onset. Decreases in PNNs, including those surrounding PV+
interneurons, have also been observed in SCZ patients and animal
models of the disease. However, the mechanisms underlying PNN deficits
in SCZ, which may include the functional capacity of microglial cells
to remodel the brain extracellular matrix, are still unclear."
It does not sound as if the Universities of Sao Paulo and Saarland are
doing the sort of thing for which, in Hong Kong, they might be fined
HK$1 million and get seven years in jail. But challenges remain:
"The protective effect of CBD on PV+ interneurons seem to depend on
5-HT1A and CB2 receptors in the vHIP [ventral hippocampus] but not in
the prelimbic mPFC. At the moment, we have no explanation for this
difference. A study with local CBD microinjection into the prelimbic
cortex indicated that 5-HT1A receptors play a complex role in this
structure. CBD could produce anxiolytic or anxiogenic responses,
depending on previous exposure to restraint stress and glucocorticoid
levels. Both responses, however, were blocked by [5-HT1AR receptor
antagonist and potent dopamine 4 receptor (D4R) full agonist]
WAY100635. Further studies are needed to understand the role of these
receptors and the mechanisms of the PV+/PNNs CBD protective effect in
this region."
https://www.biorxiv.org/content/10.1101/2024.10.21.619352v1.full.pdf
[5339]
Returning to where we began in this section, the 2023 ADHD paper of
Ittiphakorn et al...
"Patients were identified from the UK Medical Cannabis Registry.
Primary outcomes were changes in the following patient-reported
outcome measures (PROMs) at 1, 3, 6, and 12 months from
baseline: EQ-5D-5L index value, generalized anxiety disorder-7 (GAD-7)
questionnaire, and the single-item sleep quality score (SQS).
Secondary outcomes assessed the incidence of adverse events.
Statistical significance was defined as
p < 0.050.
"Results
Sixty-eight patients met the inclusion criteria. Significant
improvements were identified in general HRQoL [health-related quality
of life] assessed by EQ-5D-5L index value at 1, 3, and 6 months
(p < 0.050). Improvements were also identified in
GAD-7 [generalized anxiety disorder-7 questionnaire] and SQS [sleep
quality score] scores at 1, 3, 6, and 12 months
(p < 0.010). 61 (89.71%) adverse events were recorded
by 11 (16.18%) participants, of which most were moderate
(n = 26, 38.24%)." [4264]
Another HRQoL-based study looked at medical cannabis patients with
primary and secondary diagnoses including agoraphobia, anxiety,
attention-deficit/hyperactivity disorder, autistic spectrum disorder,
cancer pain, chemotherapy-induced nausea and vomiting, chronic
non-cancer pain, cluster headaches, complex regional pain syndrome,
Crohn's disease, depression, eating disorder, Ehlers-Danlos Syndrome,
endometriosis, epilepsy adult, fibromyalgia, headache, inflammatory
arthritis, insomnia, migraine, multiple sclerosis, neuropathic pain,
obsessive-compulsive disorder, osteoarthritis, palliative care,
Parkinson's, post-traumatic stress disorder, rare and challenging skin
condition, Tourette's syndrome, trigeminal neuralgia, and ulcerative
colitis.
"Results: 1378 patients prescribed Adven CBMPs (Curaleaf
International, Guernsey, UK) were included in the final analysis. 581
(42.16%) participants were current users of cannabis at baseline. 641
(46.51%), 235 (17.05%), and 502 (36.43%) patients were treated with
oils, dried flowers, or a combination of the two, respectively.
Improvements were found in all PROMs in each route of administration
at 1, 3, 6, and 12 months from baseline (p < 0.010). Those
prescribed dried flower only or both oils and dried flower experienced
greater improvements in GAD-7, SQS, and EQ-5D-5L index values at 12
months (p < 0.050). There was no difference in outcomes between
those prescribed dried flower only or dried flower with oils (p >
0.050). 3663 (265.82%) adverse events were reported by 297 (21.55%)
patients.
"Conclusion: There was an associated improvement in self-reported
anxiety, sleep quality, and HRQoL in patients treated with the CBMPs.
Those prescribed treatment formulations including dried flower were
most likely to show a clinical improvement. However, these results
must be interpreted with caution given the limitations of study
design."
https://onlinelibrary.wiley.com/doi/pdfdirect/10.1002/npr2.12403
[4292]
Murphy et al in "A cohort study comparing the effects of medical
cannabis for anxiety patients with and without comorbid sleep
disturbance" (2023) continues with science's astounding
discoveries:
"Background: Research on cannabis- based medicinal products (CBMPs)
in anxiety remains inconclusive due to a paucity of high-quality
evidence. Studies indicate a bidirectional relationship between
generalized anxiety disorder (GAD) and sleep disruption, but it is
unclear how this affects CBMP treatment outcomes. This study aims to
compare the patient- reported outcome measures (PROMs) of patients
prescribed CBMPs for GAD, with and without impaired sleep.
"Methods: Changes in PROMs were recorded from baseline to 1, 3, 6,
and 12 months between those with impaired or unimpaired sleep.
Multivariate logistic regression was applied to compare factors
associated with a clinically significant improvement in GAD-7 at 12
months. Secondary outcomes included adverse event incidence and
frequency.
"Results: Of the 302 patients that fit the inclusion criteria, mean
GAD-7, single-item sleep quality, and EQ-5D-5L index values improved
at all time points (p< 0.001). A relationship between sleep
impairment and clinically significant changes in GAD-7 at 1 and 3
months was identified (p ≤ 0.01). On multivariate regression, only
baseline GAD severity was associated with an increased likelihood of
observing a clinically significant improvement in anxiety (p<
0.001). Seven hundred and seven (234%) adverse events were reported by
55 (18.21%) participants.
"Conclusions: This study observed an association between CBMP
treatment and improvements in anxiety in patients with GAD. While
patients with comorbid sleep dis-ruption had greater improvements in
anxiety, the differences were not maintained in a multivariate
analysis. Baseline anxiety severity may be a predictor for CBMP
treatment outcomes"
https://onlinelibrary.wiley.com/doi/epdf/10.1002/npr2.12407
[4301]
As for the role of NECUD in mental health, a 2024 study "Youth
cannabis use and subsequent health service use for mood and anxiety
disorders: A population-based cohort study" from Toronto
"This study found a modest association between less than weekly
cannabis use and subsequent MAD health service use during youth, but
no evidence of a linear dose-response relationship as weekly or more
cannabis use was not associated with MAD health service use.
Sensitivity analyses suggested that these findings were robust to
several different model conditions while interaction analyses did not
find any sex or age differences either on the multiplicative or
additive scale."
But of course the authors could easily have drawn a line between 1.48
(<weekly) and 0.92 (weekly+), illustrating a linear relationship
between more committed users, and NECUD-afflicted users of not enough
cannabis - consisting of the doubters, the people who only smoke when
they're drunk, the people who only smoke other people's, and whatever
is today's equivalent to what we once described as "weekend hippies".
The problem is not with the existence of a linear relationship, but
that the line is going in the opposite direction to the one McDonald
et al expected. Hence their claim there is no linear relationship at
all.
https://www.sciencedirect.com/science/article/abs/pii/S0165178123006443?dgcid=author
[4313]
What can we discover about the real world results of teenage drug use
on educational attainment? The findings of Levola et al from Helsinki,
in which "Adolescent alcohol and cannabis use and early adulthood
educational attainment in the 1986 Northern Finland birth cohort
study" were assessed in 15-16 year olds were rechecked at age 33, a 17
year follow-up.
"Using weighted multivariable models, we examined prospective
associations between age at first drink (AFD), age at first
intoxication (AFI), frequency of alcohol intoxication, as well as
self-reported alcohol tolerance (i.e., number of drinks needed for the
subjective experience of intoxication), and lifetime cannabis use at
age 15/16 years with subsequent educational attainment obtained from
comprehensive registers until age 33 in the Northern Finland Birth
Cohort 1986 (6,564 individuals, 49.1% male). Confounding variables
including sex, family structure (intact vs. non-intact), maternal and
paternal education level, behavioural/emotional problems in school at
age 7/8 years, having a history of illicit substance use in
adolescence, having any psychiatric diagnosis before age 16, and
parental psychiatric diagnoses, were adjusted for."
and
"Frequent alcohol intoxication (more than three times in past 30
days) at age 15/16 years (OR 2.00; 95% CI 1.15 3.48; p=0.014) and high
self-reported alcohol tolerance (<9 alcohol units for males, <7
for females; OR 2.10; 95% CI 1.213.65; p=0.009) were associated with
increased ORs of completing primary education only compared to
secondary education (Table 2; model 1, blocks 3c and 3d). AFI (OR
0.70; 95% CI 0.600.82; p<0.001), alcohol intoxication frequency
during the past month at age 15/16 (12 times OR 0.78; 95% CI 0.670.92;
p=0.002; 3 or more times OR 0.42; 95% CI 0.320.56; p<0.001) and
high self-reported alcohol tolerance (OR 0.40; 95% CI 0.300.52
p<0.001) were associated with decreased ORs for college/university
education compared to secondary education (Table 2; model 1, blocks
3b, 3c and 3d). Notably, also those reporting lower alcohol tolerance
were less likely to complete college/university education compared to
secondary education when compared to those with no alcohol use or
never been intoxicated (OR 0.85; 95% CI 0.730.99; p=0.038).
"Cannabis use by age 15/16 years was not associated with of
completing primary education only compared to secondary education.
Lifetime use of cannabis or other illicit substance use (yes/no) was
associated with lower odds of college/university education compared to
secondary education (OR 0.68; 95% CI 0.560.82; p<0.001) when sex,
behavioural/emtional problems at age 7/8 years and psychiatric
diagnoses by age 15/16 years were controlled for (Table 2: model 1,
block 1). However, when family-related variables and frequency of
alcohol intoxication at age 15/16 years were controlled for, cannabis
use was no longer statistically significantly associated with lower
odds of college/university education compared to secondary education
(14 times OR 1.03; 95% CI 0.711.50; p=0.871; 5 times or more OR 0.88;
95% CI 0.362.17; p=0.780). (Table 2: mode 2, block 3)."
So reading between the lines, while it looked like smoking in your
teens might have something to do with not going on to further
education, once the disruption caused by prohibition - arguing with
your parents and having to leave home because of the prejudices they
have been trained by society to have against their children - once
these factors were taken into account, the association disappeared,
coming nowhere near statistical significance in this large-scale, long
term analysis.
"Discussion: In this large birth cohort study with a 17-year
followup, younger age at first intoxication, higher frequency of
alcohol intoxication, and high self-reported alcohol tolerance at age
15/16 years were associated with poorer educational outcomes by the
age of 33 years. These adverse associations were evident regardless of
a range of potential confounders, such as behavioural/ emotional
problems at age 7/8 years and parental education level. The
association between adolescent lifetime cannabis use and educational
attainment in adulthood was no longer statistically significant after
adjusting for potential confounders including alcohol use."
https://bmcpublichealth.biomedcentral.com/counter/pdf/10.1186/s12889-024-17693-w.pdf
[4461]
It might not matter either way. Coley et al (2024) in JAMA
Pediatrics
"...drew from data in 47 states, looking at responses from 898,271
teens. 'With parent consent,' authors explained, 'students from ninth
to twelfth grade self-reported prior month use of cannabis, alcohol,
cigarettes, and e-cigarettes.'
"Passage of recreational cannabis laws (RCL) 'was not associated with
adolescents likelihood or frequency of cannabis use,' the analysis
found, 'although negative total effect estimates indicated
significantly lowered use following RCL.' Nor were increases
associated with the launch of recreational cannabis retail sales
(RCR)."
and
"this study is the first to evaluate associations between RCL and RCR
policies and adolescent substance use through 2021.
The results, say the Boston College and the University of Maryland at
College Park team
"...suggest that legalization and greater control over cannabis
markets have not facilitated adolescents entry into substance
use."
https://jamanetwork.com/journals/jamapediatrics/article-abstract/2817566
[4549]
So in case the Court was considering balancing the benefits to the
over 65s against the rather exaggerated risks of teenage use these are
some factors to take into account.
We show elsewhere that Covid is associated with gliosis and that
cannabis use reduces gliosis. Further evidence in support of the
Article 2 challenge includes "SARS-CoV-2 is associated with changes in
brain structure in UK Biobank" by Douaud et al (2022), who
"...investigated brain changes in 785 participants of UK Biobank
(aged 5181 years) who were imaged twice using magnetic resonance
imaging, including 401 cases who tested positive for infection with
SARS-CoV-2 between their two scanswith 141 days on average separating
their diagnosis and the second scanas well as 384 controls. The
availability of pre-infection imaging data reduces the likelihood of
pre-existing risk factors being misinterpreted as disease effects. We
identified significant longitudinal effects when comparing the two
groups, including (1) a greater reduction in grey matter thickness and
tissue contrast in the orbitofrontal cortex and parahippocampal gyrus;
(2) greater changes in markers of tissue damage in regions that are
functionally connected to the primary olfactory cortex; and (3) a
greater reduction in global brain size in the SARS-CoV-2 cases. The
participants who were infected with SARS-CoV-2 also showed on average
a greater cognitive decline between the two time points. Importantly,
these imaging and cognitive longitudinal effects were still observed
after excluding the 15 patients who had been hospitalised. These
mainly limbic brain imaging results may be the in vivo hallmarks of a
degenerative spread of the disease through olfactory pathways, of
neuroinflammatory events, or of the loss of sensory input due to
anosmia."
https://www.nature.com/articles/s41586-022-04569-5
[4544]
The infections which can lead to brain loss extend beyond Covid,
according to "Proteomics identifies potential immunological drivers of
postinfection brain atrophy and cognitive decline" by Duggan et al
(2024), who looked at "influenza, pneumonia, tuberculosis,
candidiasis/fungal, miscellaneous bacterial infections,
gastrointestinal infections, sexually transmitted infections, human
herpes virus (HHV) infections, viral hepatitis, miscellaneous viral
infections, upper respiratory tract infections (URTIs), lower
respiratory tract infections (LRTIs), skin and subcutaneous
infections, urinary tract infections, and other infections
(Supplementary Table 1)."
"Systemic infections may influence dementia risk and
neurodegeneration by triggering an acute inflammatory response or
reshaping the host immune system, as in the case of chronic
inflammation. In response to immune insults, such as pathogens and
tissue damage, changes in circulating inflammatory proteins can
influence brain health through a variety of mechanisms, including
their interactions with target cells in the central nervous system
(CNS). For example, elevated cytokine signaling after SARS-CoV-2
infection can result in neuroinflammation and post-acute sequelae
despite its low or absent copy numbers in the CNS. Increases in plasma
inflammatory markers among cognitively normal adults are associated
with reduced brain volumes and cognitive performance, and greater
dementia risk decades later. Although several studies have tied select
immune markers (for example, tumor necrosis factor (TNF), interleukin
(IL)-1β) to preceding inflammatory events and ensuing cognitive
performance, it remains unknown how infections relate to an array of
immunological proteins, and which of these proteins may predict
changes in brain regions vulnerable to infection-specific
atrophy."
In their sample:
"Less than half (42.9%; n = 421) of participants
exhibited a history of no infection diagnoses and 10.1%
(n = 108) exhibited a history of two or more infection
diagnoses. Primary regions of interest (ROIs) included total brain,
gray matter, white matter and lobar volumes, as well as an
AD-signature region volume. Follow-up analyses were performed on lobar
white/gray matter volumes if an infection was significantly associated
with a primary ROI."
And...
"Of the 15 infections examined, 6 were associated with accelerated
brain volume loss, predominantly in temporal gray and/or white matter
regions (Fig. 2 and Supplementary Table 4). Follow-up analyses
revealed that influenza-related volume loss was specific to temporal
and occipital lobe gray matter (Fig. 2a and Extended Data Fig. 1a).
Consistent with published findings, declines in white matter volumes
linked to herpetic infections (Fig. 2b) were localized to the temporal
lobe (Extended Data Fig. 1b). Accelerated atrophy in the temporal lobe
tied to miscellaneous viral infections was specific to gray matter
(Fig. 2c and Extended Data Fig. 1c). URTIs were similarly linked to
accelerated loss in total temporal lobe volume, but such decreases
were not specific to either white or gray matter (Fig. 2d and Extended
Data Fig. 1d). LRTI-related volume loss in the temporal lobe was
exclusive to white matter, whereas decreases in the occipital lobe
were evident in both white and gray matter (Fig. 2e and Extended Data
Fig. 1e). Along with reduced total brain volume, the gray matter
atrophy related to skin and subcutaneous infections was localized to
the temporal and occipital lobes (Fig. 2f and Extended Data Fig. 1f).
Although associations between infection history and brain volume
changes were no longer statically significant after false recovery
rate (FDR) correction, such correction may not be appropriate because
of the inherent interdependence of the outcomes (for example, total
gray matter loss is related to total brain volume loss). A history of
any of the examined infections and total frequency of infections were
not associated with volume changes. Despite limited power, sensitivity
analyses restricting the comparison group to participants with a
history of no infections (for example, influenza versus no history of
any infection) showed consistent atrophy linked to influenza, herpes
viruses, miscellaneous viral infections and LRTIs, with URTI- and skin
and subcutaneous infection-related atrophy remaining marginally
significant (P ≤ 0.10) (Supplementary Table 4). For
primary ROIs, we did not find differences at baseline and results were
similar after adjusting for total infection frequency (Supplementary
Tables 4 and 5). These findings suggest that specific infections may
be associated with accelerated brain volume loss, particularly in
temporal regions."
https://www.nature.com/articles/s43587-024-00682-4
[3379]
In 2025 Pitakbut and Kayser reported that:
"After cannabinoids exhibited promising inhibitory activity against
bacterial (C. perfringens) neuraminidase in a prior experiment, the
authors further evaluated the anti-neuraminidase activity against the
influenza A virus (IAV)....Here, the authors studied nine cannabinoid
derivatives. Figure 4 shows six active cannabinoids, THC, CBD, CBE,
CBG, CBL, and CBN, completely inhibiting IAV neuraminidase activity
(100% inhibition)." [4854]
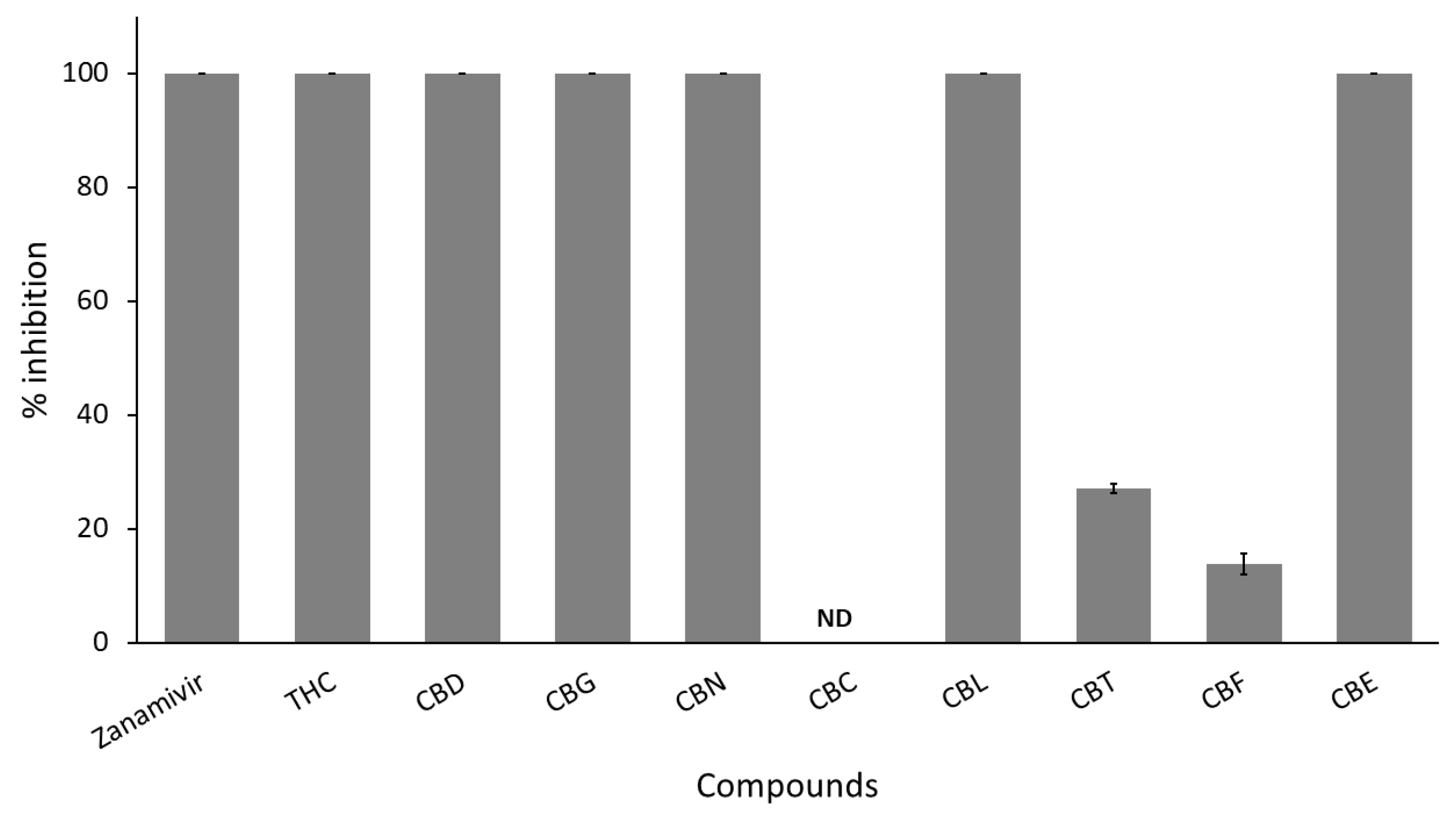
It does not seem likely, therefore, that taking cannabis away will
create an improved medical outcome for the future, present, or past
sufferer from a Covid infection. On the contrary, the evidence shows
the Police action at the time of the pandemic was an anti-health
manoeuvre.
"Lifetime Cannabis Use Is Associated with Brain Volume and Cognitive
Function in Middle-Aged and Older Adults", report Guha et al
(2025):
"Using data from the UK Biobank, which includes health information
from over 500,000 adults, associations between cannabis use, regional
brain volume, and cognition in participants aged 40-70 years (mean age
= 54.5) were evaluated.
Results: Lifetime cannabis use was positively associated with regional
brain volume in CB1-rich regions, including the caudate, putamen,
hippocampus, and amygdala. Greater lifetime use was also linked to
better performance in learning, processing speed, and short-term
memory. Individuals reporting use limited to adolescence also showed
larger regional volumes and better cognitive performance than
non-users. Sex differences in cannabis effects on brain volume and
cognition were also observed."
https://pmc.ncbi.nlm.nih.gov/articles/PMC12889878/
[5718]
Is replacing the low level of alcohol use in pregnancy (we are not
necessarily referring to Slovenia here) with a low level of cannabis
use going to be a disaster for the offspring? Isn't this just
replacing one error with another? Paige et al (2026) reveal:
"No studies have examined the differential and combined effects of
prenatal alcohol and cannabis exposure (PAE/PCE) on longitudinal
trajectories of adolescent cognitive development."
And set out to do just that, with a sample of 11029.
"Most mothers reported no prenatal alcohol (n = 8257;
74%) or cannabis (n = 10,812; 94%) use. Overall, use was
low: across pregnancy, women reporting any alcohol use averaged 33.31
drinks, and those reporting any cannabis use averaged 33.00 use
occasions. Before including covariates, there were negative main
effects of PCE and positive main effects of PAE on intercepts for all
five cognitive domains. There was little evidence for PCE/PAE effects
on slopes for cognition. After adding covariates, no negative effects
of PCE remained. Small positive PAE effects on intercepts for multiple
domains persisted. Cross‐product terms for combined exposure were not
significant.
"Conclusions
Little evidence emerged for negative effects of low PAE, PCE, or
combined exposure on adolescents' cognitive development after
accounting for sociodemographic factors. Light drinking in families
with social features positively associated with cognitive ability may
result in few negative consequences. This study is the first to
demonstrate weak evidence for adverse differential and combined
low‐level PAE and PCE effects on the development of adolescent
cognition."
https://pmc.ncbi.nlm.nih.gov/articles/PMC13058172/
[6147]
This study did not assess paternal pre-conception alcohol use.
----------------------------------------------------------------------------
The Englishman stands for the rights of everyone disadvantaged,
discriminated against, persecuted, and prosecuted on the false or
absent bases of prohibition, and also believes the victims of these
officially-sanctioned prejudices have been appallingly treated and
should be pardoned and compensated.
The Englishman requests the return of his CaPs and other rightful
property, for whose distraint Slovenia has proffered no credible
excuse or cause.
The Benedictions represent both empirical entities as well as beliefs.
Beliefs which the Defence evidence shows may be reasonably and
earnestly held about the positive benefits of CaPs at the population
level, in which the good overwhelmingly outweighs the bad. Below, the
latest version of this dynamic list.
THE BENEDICTIONS
REFERENCES
TIMELINE OF DRUG LAW v. SCIENCE