LEPTIN, STAT3, AND CANCER
In 2015 State Key Laboratory of
Oncogenes and Related Genes, Shanghai Cancer Institute, Renji Hospital, Shanghai
Jiao Tong University School of Medicine, Shanghai, China were able to us that:
"Emerging evidence has suggested that
leptin, an adipokine related to energy homeostasis, plays a role in cancer
growth and metastasis."
They explain that "Leptin
up-regulated the expression of matrix metalloproteinase-13 (MMP-13) via the
JAK2/STAT3 signaling pathway. The overexpression of leptin was shown to
significantly promote tumor growth and lymph node metastasis in a subcutaneous
model and an orthotopic model of human pancreatic cancer, respectively.
Furthermore, in human pancreatic cancer tissues, the expression of [leptin's
functional receptor] Ob-Rb was positively correlated with the MMP-13 level."
Leptin up means metastasis up:
"Consistently, we also found the
association of MMP-13 expression with lymph node metastasis and the pathological
stage"
and
"Human MMP-13, also known as
collagenase-3, is a matrix metalloproteinase originally identified in breast
carcinomas. Recent studies have revealed that this enzyme is also produced by a
variety of malignant tumors, including head and neck, breast and colorectal
cancer. In all of the cases, the expression of MMP-13 is associated with
aggressive tumors."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4599260/ [426]
Obviously I do not want leptin to be
too high or too low. But people have been regulating leptin with and without
marijuana for thousands of years before 1994.
Its novelty means the current idea of
a "normal" range has been obtained entirely during last 27 years of the
unusually wealthy recent anthropocene.
It is increased by the carbohydrates
which have replaced the hunter-gatherer diets with which early homo sapiens
evolved. This trend is discussed in considerable detail here:
https://bmcendocrdisord.biomedcentral.com/articles/10.1186/1472-6823-5-10#Sec9
[427]
Hugh J Freeman of Vancouver
University:
"Celiac disease may have developed as
a distinct disorder with the transition of hunter-gatherer groups into human
workforces capable of agriculture. This "Neolithic revolution" is believed to
have permitted competitive survival over other hunter-gatherer groups owing to
more secure food supplies. Over time, celiac disease has emerged as a major
clinical disorder, currently thought on the basis of serological studies to
affect up to about 2% of most genetically-predisposed human populations."
Celiac keeps popping up in areas of
wheat consumption, faster than could be accounted for by genetic factors.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4282854/ [428]
Battista et al, in their paper
"Altered Expression of Type-1 and Type-2 Cannabinoid Receptors in Celiac
Disease" (2013) investigated CBR mRNA and protein as well as functional activity
levels in the duodenal mucosa of UCD and TCD patients, and CS, and say:
"Our in vivo data showed that mRNA
and protein levels of both CB1 and CB2 receptors are remarkably increased in UCD
mucosa compared to TCD mucosa and normal mucosa. It is noteworthy that in TCD
patients CB2, but not CB1, levels were reverted to normal values, pointing to
CB2 rather than CB1 as main molecular target in celiac disease. Moreover, ex
vivo experiments on organ culture confirmed that gluten-induced damage is
responsible for this increase, at least at the protein level."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3631143/ [429]
It became clear by 2010 that The
endocannabinoid system links gut microbiota to adipogenesis, and "that
macrophage infiltration is not only dependent on the activation of the receptor
CD14 by lipopolysaccharide, but is also dependent on the gut microbiota
composition and the gut barrier function (gut permeability). Moreover, LPS
controls the synthesis of eCBs both in vivo and in vitro through mechanisms
dependent of the LPS receptor signalling pathway. Thus, obesity is nowadays
associated with changes in gut microbiota and a higher endocannabinoid system
tone, both having a function in the disease's pathophysiology." [Fig. 2, see ecb
controls gut]
"in vivo experiments strongly suggest
that an overactive eCB system increases gut permeability."
"we measured AEA levels and FAAH
[Fatty acid amide hydrolase, an enzyme that breaks down anandamide] mRNA
expression in adipose tissue. Prebiotics strongly decreased AEA levels and
tended to increase FAAH mRNA levels (Figure 6C), further supporting the link
between changes in gut microbiota and modulation of the eCB system."
"Blocking the CB1 receptor in obese
mice also ameliorated gut barrier function as shown by improved
distribution....CB1 activation increased gut permeability markers in vivo and in
vitro. This demonstration that CB1 receptors control gut permeability suggests a
new eCB system-dependent mechanism in the pathogenesis of obesity-associated
inflammation (systemic and hepatic)."
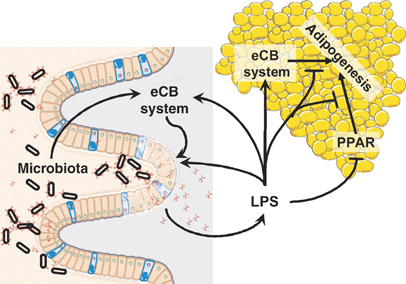
"eCB system-LPS crosstalk
participates in the regulation of adipogenesis by gut microbiota. Activation of
the eCB system in the intestine (e.g. through gut microbiota) increases gut
permeability, which enhances plasma LPS levels. This exacerbates gut barrier
disruption and peripheral eCB system tone in both the intestine and adipose
tissues. Increased fat mass results in enhanced eCB system tone. LPS inhibits
both PPAR-induced and cannabinoid ligand-induced adipogenesis. Overall, the
impairment of these regulatory loops within colon and adipose tissues found in
obesity perpetuates the initial disequilibrium, leading to a vicious cycle. This
cycle maintains the increased gut permeability, eCB system tone, adipogenesis
and fat mass development that characterise obesity."
"it is clear that genetic or
pharmacological blockade of the CB1 cannabinoid receptor protects against the
development of obesity"
https://www.embopress.org/doi/full/10.1038/msb.2010.46 [430]
A paper about allosteric as opposed
to orthosteric binding to CB receptors.
https://molpharm.aspetjournals.org/content/94/1/743 [1943]
"Studies have emphasized that gut
microbiota modulates the intestinal eCB system tone, which, in turn, regulates
gut permeability and plasma LPS, and is able to stimulate peripheral
endocannabinoids in the gut and adipose tissue. This hyperactivity of the CB1
receptor increases the permeability of the gut barrier, favoring the
translocation of more LPS into the bloodstream, which will further stimulate the
eCB system, generating a cycle in which both remain altered. In adipose tissue,
eCB disturbance leads to adipogenesis, contributing to the accumulation of body
fat and, consequently, obesity. LPS and eCB regulate, in different ways, the
apelinergic system in adipose tissue, reducing the secretion of apelin and the
expression of its AP1 receptor. The apelinergic system plays a role in energy
and glycemic homeostasis. Thus, gut microbiota seems to play a significant role
in controlling the endocannabinoid system and, consequently, as modulators of
obesity and energy homeostasis."
"In a mice model, it was observed
that increasing the percentage of linoleic acid (18:2 n-6) in the diet led to
increased levels of 2-AG and AEA, which are derived from arachidonic acid (20:4
n-6), which, in turn, is formed from linoleic acid in the body."
"dietary lipids can modulate eCB
system tone."
https://www.intechopen.com/chapters/63663 [431]
Yap et al (2026) add some "In silico insights on the binding site and function
of cannabinoids and cannabinoid acids on human 5-HT1A receptor", finding that
"CBD, CBG and CBGa are potential partial agonists of 5-HT1A receptor.
CBD, CBG and CBGa may compete with orthosteric ligand for binding.
CBDa, THCV and THCVa are potential allosteric modulators of 5-HT1A receptor.
CBDa, THCV and THCVa can block the exit of orthosteric ligand from its binding
site.
MD + 7TM Open IC can accurately predict the activity of 5-HT1A binding ligands."
https://www.sciencedirect.com/science/article/pii/S1093326325002463 [5469]
However, and since we must allow
alcoholics their freedom to drink, excess gut permeability may be undesirable in
the progression of liver disease:
"Liver disease is often times
associated with increased intestinal permeability. A disruption of the gut
barrier allows microbial products and viable bacteria to translocate from the
intestinal lumen to extraintestinal organs. The majority of the venous blood
from the intestinal tract is drained into the portal circulation, which is part
of the dual hepatic blood supply. The liver is therefore the first organ in the
body to encounter not only absorbed nutrients, but also gut-derived bacteria and
pathogen associated molecular patterns (PAMPs). Chronic exposure to increased
levels of PAMPs has been linked to disease progression during early stages and
to infectious complications during late stages of liver disease (cirrhosis)."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4451427/ [432]
As, in the seventeenth year of the ZPPPD, Slovenia
went from pretending cannabinoids had no medical uses to pretending only one
cannabinoid had only one medical use, to carry on generating excuses to
confiscate people's money, protect big pharma, and churn profits for its law
businesses at the expense of drinkers' lives, Wang et al (2017) showed in binge
drinking mice that "Cannabidiol attenuates alcohol-induced liver steatosis,
metabolic dysregulation, inflammation and neutrophil-mediated injury",
explaining that:
"Herein, we investigated the effects of CBD on liver
injury induced by chronic plus binge alcohol feeding in mice. CBD or vehicle was
administered daily throughout the alcohol feeding study. At the conclusion of
the feeding protocol, serums samples, livers or isolated neutrophils were
utilized for molecular biology, biochemistry and pathology analysis. CBD
significantly attenuated the alcohol feeding-induced serum transaminase
elevations, hepatic inflammation (mRNA expressions of TNFα, MCP1, IL1β, MIP2 and
E-Selectin, and neutrophil accumulation), oxidative/nitrative stress (lipid
peroxidation, 3-nitrotyrosine formation, and expression of reactive oxygen
species generating enzyme NOX2). CBD treatment also attenuated the respiratory
burst of neutrophils isolated from chronic plus binge alcohol fed mice or from
human blood, and decreased the alcohol-induced increased liver triglyceride and
fat droplet accumulation. Furthermore, CBD improved alcohol-induced hepatic
metabolic dysregulation and steatosis by restoring changes in hepatic mRNA or
protein expression of ACC-1, FASN, PPARα, MCAD, ADIPOR-1, and mCPT-1."
Note: mast cell protease 1 has no direct homolog in
humans.
https://pmc.ncbi.nlm.nih.gov/articles/PMC6554654/ [5735]
De Ternay et al (2019) agreed CBD reduces hepatic
alcohol damage:
"CBD modulated the ethanol-induced dysregulation of
numerous genes and proteins involved in metabolism and liver steatosis, such as
key genes of fatty acid biosynthetic and oxidation pathway, mitochondrial
pathway, and transcription factor PPAR-α. Furthermore, in the ethanol-fed mice
group, CBD attenuated hepatic neutrophils infiltration, oxidative and nitrative
stress, decreased several markers of liver inflammation such as TNF-α, the
expression of adhesion molecule E-selectin, proinflammatory chemokine and
cytokines, and thus, attenuated liver injury induced by chronic plus binge
ethanol exposure."
De Ternay et al review evidence in three areas of CBD
benefit in AUD: reduction of drinking, modulation the inflammatory processes in
the liver, and reduction of alcohol-related brain injury [ARBI]. Additionally,
they say, CBD can reduce alcohol-related seizures, anxiety, and chronic pain. [1921]
Erukainure et al (2021) stirred up further evidence by
using whole plant extracts to produce "Cannabis sativa L. (var. indica) Exhibits
Hepatoprotective Effects by Modulating Hepatic Lipid Profile and Mitigating
Gluconeogenesis and Cholinergic Dysfunction in Oxidative Hepatic Injury":
"This study sought to investigate the hepatoprotective effect of C. sativa on
iron-mediated oxidative hepatic injury. Hepatic injury was induced ex vivo by
incubating hepatic tissues with Fe2+, which led to depleted levels of reduced
glutathione, superoxide dismutase, catalase and ENTPDase [ecto-nucleoside
triphosphate diphosphohydrolase] activities, triglyceride, and high-density
lipoprotein–cholesterol (HDL-C). Induction of hepatic injury also caused
significant elevation of malondialdehyde, nitric oxide, cholesterol, and
low-density lipoprotein–cholesterol (LDL-C) levels while concomitantly elevating
the activities of ATPase, glycogen phosphorylase, glucose-6-phosphatase,
fructose-1,6-bisphosphatase, amylase, and lipase. Treatment with the hexane,
dichloromethane (DCM), and ethanol extracts of C. sativa leaves significantly (p
< 0.05) reversed these levels and activities to almost near normal. However,
there was no significant effect on the HDL-C level. The extracts also improved
the utilization of glucose in Chang liver cells. High-performance liquid
chromatography (HPLC) analysis showed the presence of phenolics in all extracts,
with the ethanol extract having the highest constituents. Cannabidiol (CBD) was
identified in all the extracts, while Δ-9-tetrahydrocannabinol (Δ-9-THC) was
identified in the hexane and DCM extracts only. Molecular docking studies
revealed strong interactions between CBD and Δ-9-THC with the β2 adrenergic
receptor of the adrenergic system. The results demonstrate the potential of C.
sativa to protect against oxidative-mediated hepatic injury by stalling
oxidative stress, gluconeogenesis, and hepatic lipid accumulation while
modulating cholinergic and purinergic activities. These activities may be
associated with the synergistic effect of the compounds identified and possible
interactions with the adrenergic system."
https://pmc.ncbi.nlm.nih.gov/articles/PMC8724532/ [5737]
Gojani et al (2023) on the other hand took a reductive approach, examining
specific CCx:
"Our findings indicate that all five phytocannabinoids reduce HG-HL-induced
-cell loss likely through reducing apoptosis and pyroptosis. The protective
effects of CBD, THCV, CBC, and CBN were seen in the GSIS impairment by HG-HL.
Although all five phytocannabinoids tested in this research demonstrated the
capability to inhibit β-cell dedifferentiation induced by HG-HL, CBD seems to be
more effective compared to the other phytocannabinoids, as indicated by the
specific biomarker responses of β-cells and progenitor cells to CBD."
https://www.preprints.org/manuscript/202309.0973 [5736]
Walsh et al (2021) would like us to know that:
"Unlike the continuous
cellular synthesis and storage of neurotransmitters and neuropeptides, AEA and
2-AG are produced through 'on demand' cleavage of NAPE and PIP2. This provides
for a temporal- and localization-dependent release of the endocannabinoids (Lu
and Mackie, 2016). The actions of AEA and 2-AG are terminated following their
cellular uptake and degradation by intracellular hydroxylase [fatty acid amide
hydrolase (FAAH)] (for AEA) and lipase enzymes (monoacylglycerol lipase) (for
2-AG). Therefore, drugs that inhibit the cellular uptake of AEA and 2-AG or
prevent their enzymatic degradation should result in a potentiation of
endocannabinoid action."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8669157/
[854]
"Chemopreventive effect of the
non-psychotropic phytocannabinoid cannabidiol on experimental colon cancer" is
the subject of a 2012 paper by Aviello et al when
"...we investigated its possible
chemopreventive effect in the model of colon cancer induced by azoxymethane
(AOM) in mice. AOM treatment was associated with aberrant crypt foci (ACF,
preneoplastic lesions), polyps, and tumour formation, up-regulation of
phospho-Akt, iNOS and COX-2 and down-regulation of caspase-3.
Cannabidiol-reduced ACF, polyps and tumours and counteracted AOM-induced
phospho-Akt and caspase-3 changes. In colorectal carcinoma cell lines,
cannabidiol protected DNA from oxidative damage, increased endocannabinoid
levels and reduced cell proliferation in a CB(1)-, TRPV1- and PPARγ-antagonists
sensitive manner. It is concluded that cannabidiol exerts chemopreventive effect
in vivo and reduces cell proliferation through multiple mechanisms."
https://pubmed.ncbi.nlm.nih.gov/22231745/ [3685]
"Cannabidiol Targets Colorectal
Cancer Cells via Cannabinoid Receptor 2, Independent of Common Mutations" say
Moniruzzaman et al (2025):
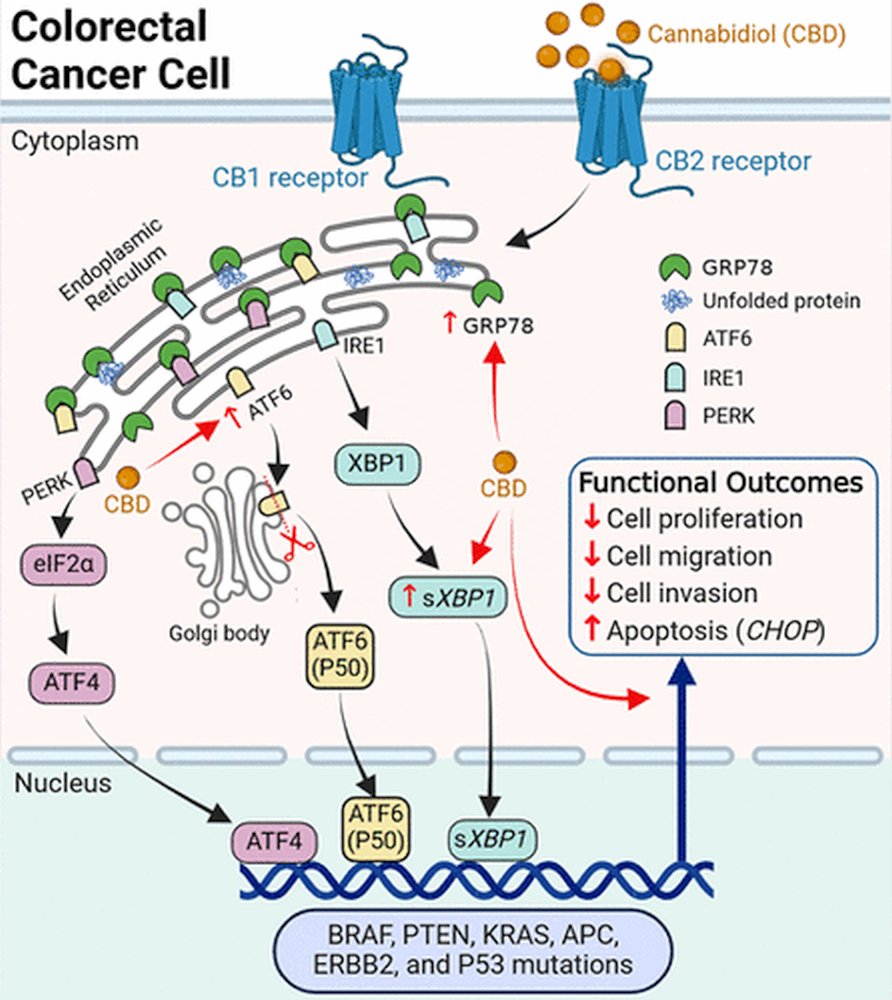
"Our results demonstrate that CBD
induces apoptosis and halts proliferation, migration, and invasion of CRC cell
lines in a concentration-dependent manner. CBD showed potent antitumor effects
in the tested cell lines with no obvious effect from different mutations such as
KRAS, BRAF, APC, PTEN, etc. CBD also induced ER stress in CRC cells but not in
healthy intestinal organoids. Cotreatment with SR144528 inhibited the effects of
indicating involvement of CB2 receptor activation in the anticancer effects of
CBD. Together, these results demonstrated that CBD could be effective for CRC
regardless of the underlying mutation through CB2 receptor activation."
https://pubs.acs.org/doi/full/10.1021/acsptsci.4c00644 [3951]
Vago et al at the San Raffaele
Scientific Institute, Milan have a subheading in their paper entitled "The
Mediterranean Diet as a Source of Bioactive Molecules with Cannabinomimetic
Activity in Prevention and Therapy Strategy" (2022):
"Modulation of the ECS Alters the
Microbiota Composition
"Recent studies have proven that
targeting the ECS directly can lead to an alteration in the composition of the
gut microbiota in favor of species with a positive impact on health. It was seen
that the microbiota and the endocannabidiome cooperate in a series of
intertwined pathways, which, when disrupted, can worsen preexisting low-grade
inflammation and insulin resistance in obese patients. The involvement of CB1 in
intestinal and metabolic homeostasis has been studied in detail, identifying its
antagonism as a possible way to improve gut barrier function. A higher ECS tone
has been associated with an increase in gut permeability and treatment with a
CB1 agonist HU-210 induced, as a consequence, severe metabolic disturbances such
as glucose intolerance, lipid accumulation in the muscle and endotoxemia.
Bahrami et al. have proven for the first time that CB1 blockade improves colonic
inflammation, systemic inflammation and insulin resistance in diet-induced
obesity (DIO) mice fed with a high-fat diet and treated with Rimonabant
(SR141716A), a CB1 antagonist. Interestingly, CB1 antagonist administration also
altered the gut microbiota composition in favor of more protective species such
as Akkermansia muciniphila, which is known to ameliorate DIO and diabetes
parameters such as endotoxemia, adiposity, glucose metabolism and insulin
resistance when transferred live in mouse models. This species' abundance was
suggested to be restored as a consequence of increased expression of MUC2, a
transcription factor in charge of host mucin production regulation. Mucin is the
main nutrient source for A. muciniphila and is essential for its growth. These
outcomes were demonstrated to be rimonabant administration-dependent in obese
mice and were also proven to be independent from caloric restriction and weight
loss. In addition to increased abundance in A. muciniphila, the authors observed
a decrease in the Lachnospiraceae and Erysipelotrichaceae families. This is a
significant finding, as these two bacterial families belonging to the Firmicutes
phylum are thought to be involved in weight gain and metabolic syndrome
induction, but also in diabetes and inflammation-related GI disorders. What
appears to make the link between CB1 antagonism and gut microbiota even stronger
is the increased production of butyric and propionic acid evaluated by Bahrami
et al. by conducting gas chromatography on the mice's cecal material. This
increased production of short chain fatty acids can be explained by an increased
abundance of beneficial butyrogenic and propionogenic species following the
administration of Rimonabant. A. muciniphila is a prominent example of this
statement, as propionic acid is its main metabolite. This interpretation,
however, remains a hypothesis, as the authors believe the effects that
Rimonabant had on the composition of the gut microbial community in toto could
be secondary to its effect on the inflammatory state, which then led to a change
in the environmental characteristics of the intestine."
They add:
"Markey et al. explored the impact of
Candida albicans on the gut-brain axis and its ability to dysregulate the
balance of the ECS. It has been seen that C. albicans colonization, while
protecting the gut's health against pathobionts, induces an AEA-CB1 deficit
which increases both stress-induced and basal corticosterone production related
to anxiety-like behavior. By administering a FAAH blocker (URB597) to C.
albicans colonized mice, the trend was reversed, while no effect was noted in
mock-colonized mice. K-means cluster analysis supported the hypothesis that the
AEA deficit was responsible for the changes in behavior, which was further
proven by the increased abundance of two other NAEs (linoleoyl and linoleoyl
ethanolamine) in the cecum of C. albicans colonized mice. The authors explain
that the change in precursor abundance in the GI tract noticed through feeding
studies could contribute to the alterations in AEA levels that were observed in
this study. Despite not being involved in the lifestyle-related diseases that
are in study in this review, this is an example of how there could be
undiscovered links between certain species of the microbial community and a
healthier ECS equilibrium. While Markey et al. showed that Candida albicans
alone seems to have the ability to modulate the ECS, Lacroix et al. showed that
there is a strong time-dependent association between the abundance of several
bacterial genera of the intestinal microbiota and the concentration of AEA and
2-AG in the ileum and plasma of high-fat high sugar (HFHS) diet-fed mice. This
study also showed a decrease in CB2 expression in the early stages of the HFHS
diet, which could have shifted the ECS mediator profile to preferential binding
to CB1, which then increased intestinal permeability, inflammation, insulin
resistance and may have led to a subsequent change in the composition of the
microbiota. It is undeniable that there are numerous undiscovered details that
need to be clarified by future studies, but these observations confirm that
there is some kind of cooperation between single microorganism species that,
each with its own metabolism, can contribute to a healthy gut environment by
acting on the ECS."
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8839035/ [1014]
As Farooqi et al were to remind the medical profession in 2023 in the context of
endometriosis:
"Endocannabinoids and exogenous cannabinoids exert opposite effects on gut
permeability. For instance, when examining decreased permeability as a result of
inflammation, it was demonstrated that 2-AG and AEA increased permeability,
while THC and CBD decreased permeability." [5496]
Compare this to the state of knowledge fifteen years after General Smuts' gift
to the world, when there was no concept of lipids as messengers. Chapter 46 of
Bainbridge and Menzies' Essentials of Physiology 9th edition (1940) "Intestinal
Digestion and Absorption" makes no special mention of gut commensals and the
process is treated as if a machine, almost without life. The most that could be
discerned about drug influences on peristalsis was that:
"Peristalsis continues in a normal
fashion when all the nerves passing from the central nervous system have been
divided, but it is abolished by painting the wall of the intestine with cocaine
or nicotine, which puts the myoneural plexuses of Auerbach and Meissner out of
action."
Bainbridge and Menzies' Essentials of
Physiology 9th edition, 1940 [380]
But these were the Dark Ages of lipid
biochemistry. The lipid hypothesis became lost in the hedgerows:
"Nikolai Anitschkow that laid the
foundation of what would later be termed the “lipid hypothesis,” or the concept
that elevated blood cholesterol concentrations induced atherosclerosis. He
showed that feeding rabbits purified cholesterol raised blood cholesterol levels
and induced atherosclerotic lesion formation, and that the extent of
atherosclerosis was proportional to the absolute amount of and length of
exposure to high blood cholesterol. In contrast, similar experiments in dogs and
rats did not elicit a similar response, results that lent skepticism to the
lipid hypothesis. The inability to induce atherosclerosis in these species was
later found to be due to their relative resistance to diet-induced
hypercholesterolemia."
https://www.jlr.org/article/S0022-2275(20)35387-6/fulltext [1724]
Daniel Steinberg in a history of the
cholesterol controversy elaborates:
"Cholesterol feeding in these species
[dogs and rats] failed to induce lesions. So, understandably, these
investigators concluded that Anitschkow’s results must reflect some peculiarity
of the rabbit. After all, it is a strict herbivore that normally has zero
cholesterol intake and a very low fat intake. The rabbit model was dismissed as
irrelevant to human disease. What was not appreciated was the fact that rats and
dogs, unlike rabbits, are very efficient in converting cholesterol to bile
acids. Consequently, even on very high cholesterol intakes the blood cholesterol
in these species does not increase appreciably."
and
"During World War II, Cohn et al. and
Oncley, Scatchard, and Brown at Harvard developed elaborate largescale methods
for fractionating human serum to provide materials useful in treating the
wounded. In the course of those systematic studies, they found that the lipids
of serum were concentrated in two major fractions having α- and β-mobility,
respectively."
To help us position the state of
ignorance at this time in the context of the conquest of cannabis, Steinberg
goes on to explain that at this time (i.e. after the League's last health
investigation in 1935, after Reefer Madness came out (1936), after the Marijuana
Tax Act 1937, and after the war was over) as far as these major fractions were
concerned
"...nothing was known about their
origin, their fate, or their biological significance."
https://www.jlr.org/article/S0022-2275(20)31274-8/pdf [1725]
What did the authors of the 1925
treaty and the 1961 SCND know about the effects of cannabinoids on bile acids
and hypercholesteremia?
After some rather unpleasant
experiments in dogs, in 1922 G. H. Whipple of the School of Medicine and
Dentistry, University of Rochester, N. Y, writes:
"Evidently there is a mechanism in
the normal animal which controls the production and destruction of bile salts
within certain limits but this is a complete mystery."
https://journals.physiology.org/doi/pdf/10.1152/physrev.1922.2.3.440 [2045]
"In his seminal early paper
(published in Dutch), [Cornelis] de Langen described clinical relationships
among diet, serum cholesterol, and atherosclerosis: '. . . a cholesterol-rich
diet and severe metabolic diseases, such as diabetes, obesity, nephritis, and
arteriosclerosis, are associated with hypercholesterolemia.'"
de Langen (1916) is credited with the
first credible epidemiological investigation of the role of cholesterol in
atherosclerosis, although it went mostly unnoticed. Similar findings seemed to
confirm his Diet-Heart theory in 1940.
http://www.epi.umn.edu/cvdepi/essay/cornelis-de-langen-diet-heart-theory-1916/
[2955]
Ancel Keys took the anti-fat crusade
to town on behalf of the sugar and carbohydrate industries. But the debate rages
on, as experimental design improved. For example "The fallacies of the lipid
hypothesis" by Uffe Ravnskov in the Scandinavian Cardiovascular Journal, the
author found as many or more than 50% of the relevant studies showed:
"High cholesterol may be beneficial
By 1992, a meta-analysis of 19 cohort
studies including more than 600 000 men and women from many countries had found
that cholesterol was inversely associated with mortality from respiratory and
digestive diseases, most of which were of an infectious origin. The observation
was in line with a large number of epidemiological, laboratory and experimental
studies showing that high cholesterol protects against infections. The main
effect seems to be exerted by the LDL molecule."
https://www.tandfonline.com/doi/full/10.1080/14017430801983082 [2956]
In 2005 Mielke et al cast further
doubt on the alleged evils of cholesterol:
"Neuropsychiatric, anthropometric,
laboratory, and other assessments were conducted for 392 participants of a 1901
to 1902 birth cohort first examined at age 70. Follow-up examinations were at
ages 75, 79, 81, 83, 85, and 88. Information on those lost to follow-up was
collected from case records, hospital linkage system, and death certificates.
Cox proportional hazards regression examined lipid levels at ages 70, 75, and 79
and incident dementia between ages 70 and 88.
"Results: Increasing cholesterol
levels (per mmol/L) at ages 70 (hazard ratio [HR] 0.77, 95% CI: 0.61 to 0.96, p
= 0.02), 75 (HR 0.70, CI: 0.52 to 0.93, p = 0.01), and 79 (HR 0.73, CI: 0.55 to
0.98, p = 0.04) were associated with a reduced risk of dementia between ages 79
and 88. Examination of cholesterol levels in quartiles showed that the risk
reduction was apparent only among the highest quartile at ages 70 (8.03 to 11.44
mmol/L [311 to 442 mg/dL]; HR 0.31, CI: 0.11 to 0.85, p = 0.03), 75 (7.03 to
9.29 mmol/L [272 to 359 mg/dL]; HR 0.20, CI: 0.05 to 0.75, p = 0.02), and 79
(6.82 to 9.10 mmol/L [264 to 352 mg/dL]; HR 0.45, CI: 0.17 to 1.23, p = 0.12).
Triglyceride levels were not associated with dementia."
https://www.neurology.org/doi/10.1212/01.WNL.0000161870.78572.A5?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
[4788]
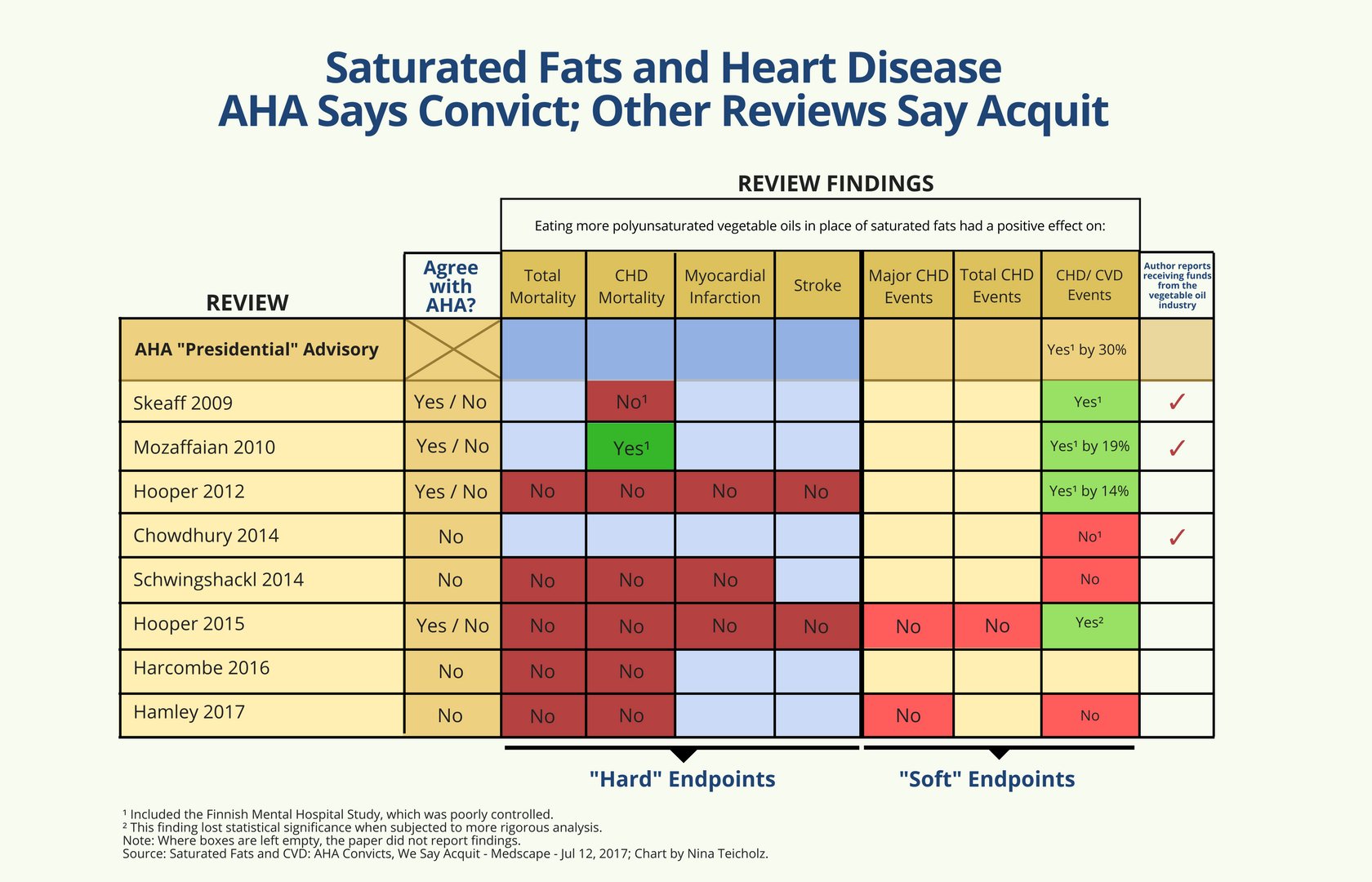
By 2023 the certainties of the
previous century were undone. The title "A short history of saturated fat: the
making and unmaking of a scientific consensus" speaks for itself.
Ignoring de Langen, it claims
"The diet-heart hypothesis was first
proposed in the 1950s by Ancel Keys".
and says
"The idea that saturated fats cause
heart disease, called the diet-heart hypothesis, was introduced in the 1950s,
based on weak, associational evidence. Subsequent clinical trials attempting to
substantiate this hypothesis could never establish a causal link. However, these
clinical-trial data were largely ignored for decades, until journalists brought
them to light about a decade ago. Subsequent reexaminations of this evidence by
nutrition experts have now been published in >20 review papers, which have
largely concluded that saturated fats have no effect on cardiovascular disease,
cardiovascular mortality or total mortality. The current challenge is for this
new consensus on saturated fats to be recognized by policy makers, who, in the
United States, have shown marked resistance to the introduction of the new
evidence. In the case of the 2020 Dietary Guidelines, experts have been found
even to deny their own evidence. The global re-evaluation of saturated fats that
has occurred over the past decade implies that caps on these fats are not
warranted and should no longer be part of national dietary guidelines. Conflicts
of interest and longstanding biases stand in the way of updating dietary policy
to reflect the current evidence."
Among the revelations by The
Nutrition Coalition founder Nina Teicholz:
"By the late 1960s, a bias in favor
of the diet-heart hypothesis was strong enough that researchers with contrary
results found themselves unable or unwilling to publish their results. For
instance, the largest test of the diet-heart hypothesis, the Minnesota Coronary
Survey, involving 9057 men and women over 4.5 years, tested a diet of 18%
saturated fat against controls eating 9%, yet did not find any reduction in
cardiovascular events, cardiovascular deaths, or total mortality. Although the
study had been funded by the NIH, the results were not published for 16 years,
after the principal investigator, Ivan Frantz, had retired. Frantz is reported
to have said that there was nothing wrong with the study; ‘We were just
disappointed in the way it came out’. Frantz's decision not to publish his
results in a timely manner resulted in these contradictory data not being
considered for another 40 years."
and concludes
"Until the recent science on
saturated fats is incorporated into the U.S. Dietary Guidelines, the policy on
this topic cannot be seen as evidence-based."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9794145/ [2957]
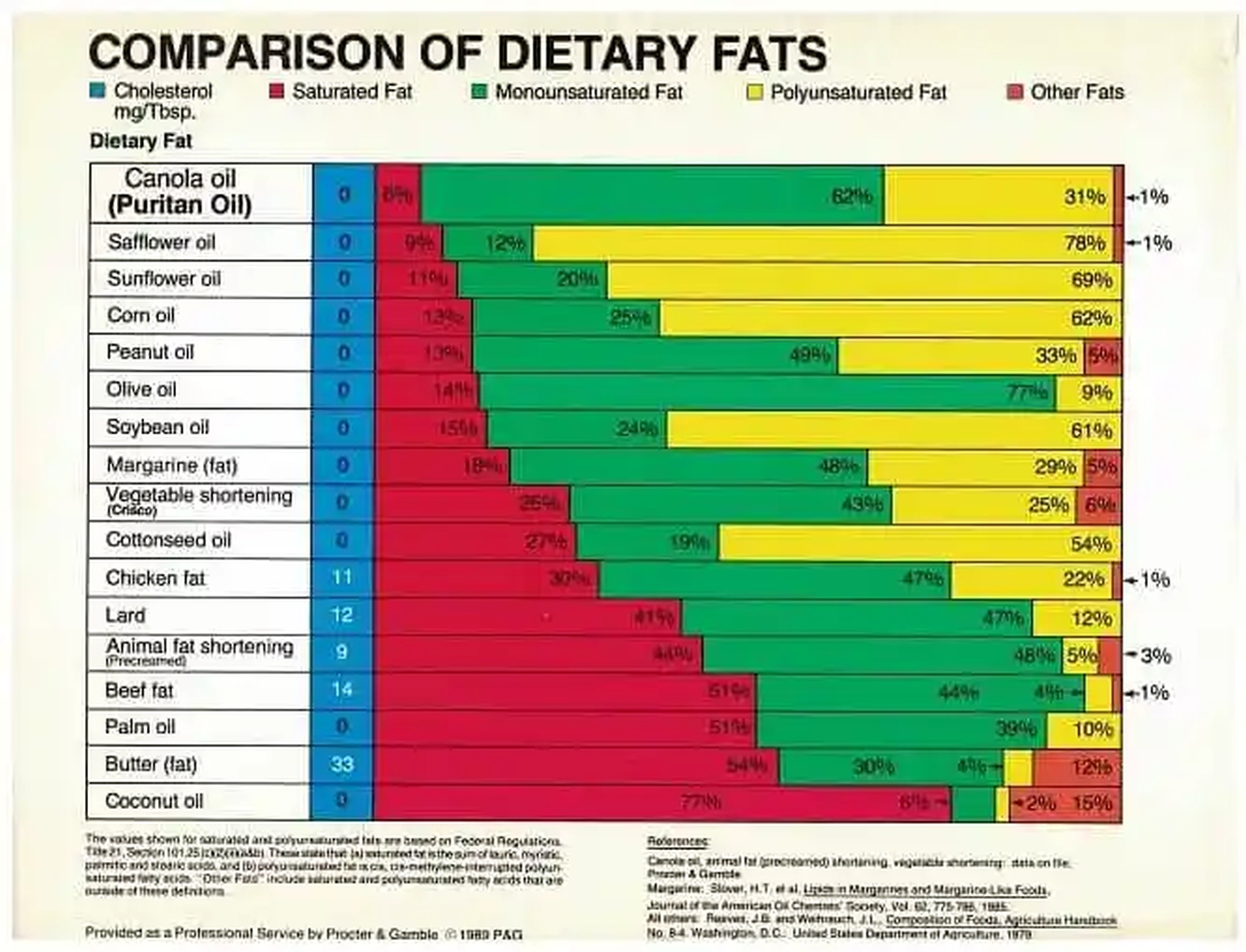
Another revelation concerns the AHA:
"'The 1961 AHA advice to limit
saturated fat is arguably the single-most influential nutrition policy ever
published, as it came to be adopted first by the U.S. government, as official
policy for all Americans, in 1980, and then by governments around the world as
well as the World Health Organization.'"
...
"However, they were paid off to
distribute this information. The AHA accepted $20 million (in today's dollars)
in funding from Procter & Gamble, a corporation that conveniently makes and
sells Crisco Oil. The AHA recommended that everyone replace butter with 'heart
healthy' alternatives like vegetable oil or Crisco Oil."
...
"It's no wonder more people than ever
are skeptical of public health organizations and mainstream experts who claim to
possess the final word on health and nutrition, when there is so much proof that
information has been censored and even doctored in order to push a certain
message that will help corporations like Procter & Gamble become richer and
richer."
https://www.eviemagazine.com/post/american-heart-association-was-paid-procter-gamble-heart-disease-saturated-fat-seed-oils-sugar
[4490]
Joy Y Kiddie MSc, RD shared some 1976
handouts from Procter and Gamble, who had tried to invent soap using waste
cottonseed oil and ended up inventing Crisco shortening, in 1911.
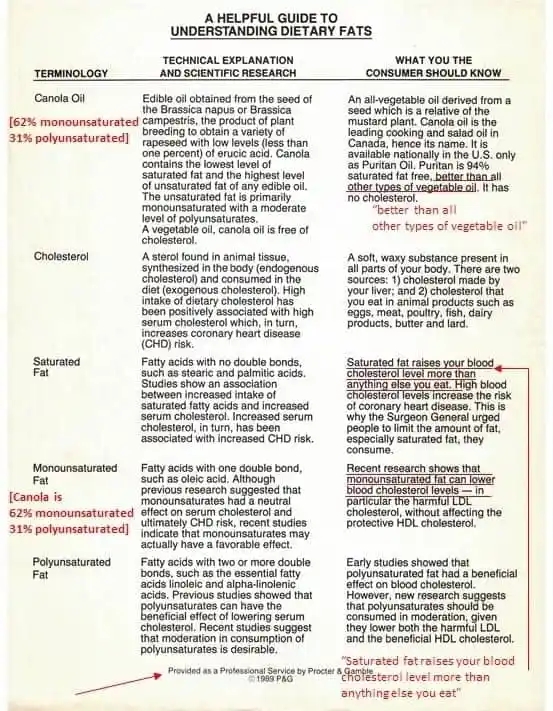
"Looking back on the role of fat
manufacturers and the sugar industry (outlined in the preceding article) on
which foods were recommended and promoted, it makes me question what I was
taught and who affected what I was taught. Given that it was known at the time
the sugar industry funded the researchers that implicated saturated fat as the
alleged cause of heart disease, I wonder what we don’t know about which industry
funded which research. After all, the knowledge about the sugar industry having
funded the researchers that implicated saturated fat only ‘came out’ in November
2016 when it had occurred decades earlier."
https://www.lchf-rd.com/2018/03/15/the-marketing-of-vegetable-oil-to-an-unsuspecting-public/
[4482]
The predilection amongst scientists
to sail with the current was prevalent.
Says Teicholz in a 2024 Medscape
article:
"Recognizing the need for rigorous
data, governments around the world, including our own National Institutes of
Health (NIH), spent billions of dollars in the ensuing decades on some of the
largest and longest human clinical trials ever conducted. Somewhere between
10,000 and 53,000 people were tested on diets in which saturated fats were
replaced by unsaturated vegetable oils (the tally depends on which trials are
counted). However, the results did not turn out as hoped, and so researchers,
either unable or unwilling to believe the outcomes, largely buried the data. For
instance, the leaders of one large NIH-funded study with findings unfavorable to
the diet-heart hypothesis did not publish them for 16 years. When asked why, one
reportedly replied that there was nothing wrong with the study; 'We were just
disappointed in the way it turned out.'"
https://www.medscape.com/viewarticle/882564?form=fpf#vp_5 [4481]
We are left wondering why, after
decades of Proctor and Gamble's advice via the auspices of the American Heart
Association, to avoid or reduce saturated fat, the average person is fatter than
ever before.
Yet for the Huntley College of
Agriculture, California State Polytechnic University, Pomona, "cholesterol is
bad" was still an article of faith in 2020.
https://www.mdpi.com/2072-6643/12/8/2329/pdf?version=1596540267 [2958]
While in 2021 the e-Journal of
Cardiology Practice does not question Ancel Keys' work, and takes a pretty
uncritical view of the missteps of the past. But does provide details of other
contributors to the discovery timeline, dietary debates and drug treatments.
Several iterations of lipid profile modelling culminated in the US 1998
guidelines which became the "gold standard" for diagnosis.
https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-19/history-in-medicine-the-story-of-cholesterol-lipids-and-cardiology
[2960]
Does it sound to you as if the role
of cholesterol in atherosclerosis was settled at the time of the 1924/25
Conference?
How about by the time of the 1961
SCND?
And by the time of the 1971 Protocol,
was it settled?
And when Slovenia inherited what it
believed to be the drug treaty obligations of the former Yugoslavia (however
translated) in 1991, was the cholesterol question satisfactorily resolved?
When the ZPPPD was enacted in 2000,
was it settled then? For your information, "The fallacies of the lipid
hypothesis" was published in 2009.
The attendees at these various
measures wouldn't have known if cannabis contributed in any way, perhaps
positively, to the regulation of bile salts?
Do you expect there is any evidence
the Plenipotentiaries considered that at all?
By the time cannabis was dropped from
the British Pharmacopoeia in 1932, work was afoot to find out what these bile
acids were. In 1934 Rosenheim and King applied the studies of Bernal (1932) to
elucidation of the structure of bile acids. Bile acids contribute to the
digestion of exogenous fats, e.g. triglycerides. With Wieland and Windaus'
formula of 1928
"...it seemed as if the last chapters
in the story of one of the most brilliant researches of organic chemistry had
been written. The ring system of an important group of natural subsyances had
been established with a degree of certainty which seemed to be final."
But two carbon atoms remained
"homeless" and
"It soon became apparent that the
C2H5 group was not in Ring IV, and in spite of four years' systematic effort it
proved to be impossible to place the two carbon atoms elsewhere in the ring
system. The old formula thus became untenable."
https://www.annualreviews.org/doi/pdf/10.1146/annurev.bi.03.070134.000511
[2044]
So could the authors of the Opium
Treaty known anything about cannabis and bile acids in 1925? Could the Kingdom
of Yugoslavia have known on the 6 January 1929?
Clearly if they did not know what the
bile acids were, what their structure was, and did not know what the active
principles of cannabis were, they could not have predicted the results of their
interaction, could they?
Once cannabis was banned, it couldn't
be the object of respectable research, could it?
In 1956 J B Carey
"...identified chenodeoxycholic acid
(CDCA) as a major biliary bile acid and proposed that lithocholic acid, its
bacterial metabolite, caused liver injury in man."
"When a meal is ingested, the hormone
cholecystokinin is released from the small intestine. Cholecystokinin induces
gallbladder contraction as well as relaxation of the valve (sphincter of Oddi)
at the end of the common bile duct where it empties into the small intestine.
Bile then enters the duodenum. Some of the bile acids are absorbed in the
jejunum, but most are transported by intestinal peristalsis to the distal ileum
where they are efficiently absorbed. The bile acid molecules pass through ileal
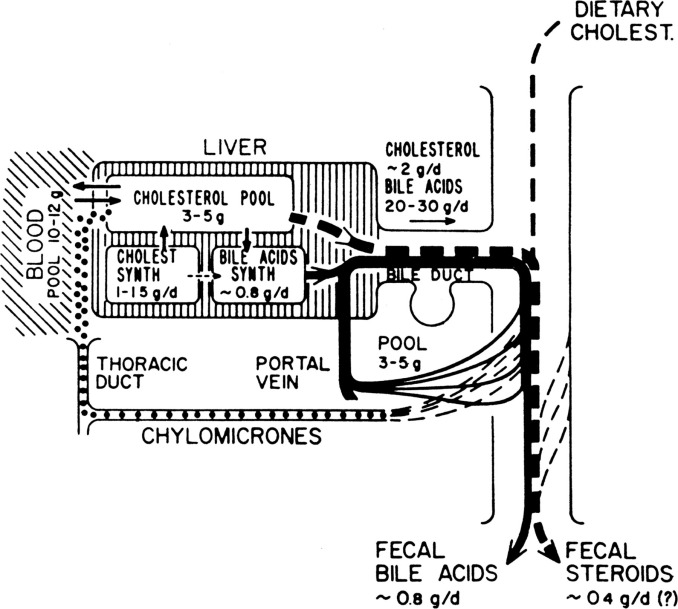
enterocytes and enter portal venous blood to return to the liver. One of the
early illustrations of the enterohepatic circulation of bile acids with values
for man was presented by Sune Bergström in 1959 and is shown in Fig. 8."
Now we've seen cannabis was widely
used for antiemesis and digestive assistance in the UK from its arrival with
O'Shaughnessy in the 1840s until its banishment after WW1.
Is there any way, in 1925, that the
authors of the first international drug treaty to include cannabis, knew
anything about the values for man for enterohepatic circulation of bile acids
first revealed by Bergström in 1959?
In his "Key discoveries in bile acid
chemistry and biology and their clinical applications: history of the last eight
decades" (2014) Hofmann and Hagey of the Department of Medicine, University of
California, San Diego, San Diego, CA reveal that
"The first symposium devoted solely
to bile acids was organized by Leon Schiff, a clinical hepatologist, who was one
of the founders of the American Association for the Study of Liver Diseases.
This symposium, held in 1967, was quite exciting for its participants who are
shown in Fig. 1."

"However, it is safe to say that the
study of bile acids was pursued by only a small number of laboratories, some in
Departments of Biochemistry and some in Departments of Medicine. Erwin Mosbach,
one of the early workers in bile acid metabolism, once stated to his wife,
'Whenever I go to the podium to give a paper on bile acids, everyone leaves the
room'.
"In 1965, the senior author, working
in the laboratory of E. H. Ahrens, began feeding studies with cholic acid in a
patient with severe hypercholesterolemia, and showed that cholic acid feeding
was a potent suppressor of bile acid and cholesterol biosynthesis, based on
measurement of fecal bile acids and sterols, using the newly developed gas
chromatographic method for fecal bile acids that had been developed in this
laboratory. It was logical to test CDCA, the other primary bile acid, but at
that time, the world's supply of pure CDCA was thought to be less than 10 g, and
the synthesis from cholic acid was difficult. However, in the 1960s, a small
English pharmaceutical company (Weddell Pharmaceuticals) began the manufacture
of CDCA for unknown reasons. A kilogram was purchased for the senior author by
the Mayo Clinic in 1967. Leslie Schoenfield returned to the Mayo Clinic in 1966
after having spent a year in the laboratory of Sjövall, and initiated a clinical
trial with his fellow, Johnson Thistle, to test whether oral cholic acid or
hyodeoxycholic acid would lower cholesterol in bile and ultimately induce
cholesterol gallstone dissolution. The senior author persuaded Schoenfield to
add CDCA to his protocol, and this study of Thistle and Schoenfield showed that
CDCA feeding decreased biliary cholesterol saturation, whereas neither cholic
acid nor hyodeoxycholic acid had any effect. In 1972, the first gallstone
dissolution induced by the ingestion of CDCA was observed, initially at the Mayo
Clinic, and later in London by a group led by Hermon Dowling. [This was not the
first time that the efficacy of oral bile acids had been tested at the Mayo
Clinic. In 1938, Philip Hench had fed a mixture of conjugated bile salts in an
unsuccessful attempt to treat rheumatoid arthritis.]
"The discovery that CDCA
[chenodeoxycholic acid] would induce gradual dissolution of cholesterol
gallstones led to the next resurgence of interest in bile acids. For the very
first time, CDCA was made in kilogram quantities by several manufacturers, and
became the third bile acid available as a fine chemical."
https://www.sciencedirect.com/science/article/pii/S0022227520353232#bib34
[2042]
So would you agree that the authors
of the international treaties of 1925 and 1961 did not know anything at those
times about interactions between cannabis and bile acids?
We can observe, in fact, that the
human diet has undergone its most dramatic modifications in the last 80 years.
Ultraprocessed food, starting in the nineteenth century, developed further after
the war with the wider entry of women into the workplace and the availability of
home refrigeration and, later, microwaves.
Some say ultra-processed food - this
does have a strict scientific definition - overtook smoking as the world's
leading cause of death in 2019.
"The food system we live within is
incredibly violent to our bodies," says Chris van Tulleken, "and it desperately
needs changing. And people can't make choices that are healthy, many people are
incredibly constrained by the world around them."
And the doctor says:
"Food made by massive companies with
obligations to pension funds affects your body differently to food made at home
by someone that loves you. It's what we've all believed for decades, now we have
very robust evidence that proves it."
https://www.youtube.com/watch?v=l3U_xd5-SA8 [2668]
A prospective study with 105 159
participants examined "Ultra-processed food intake and risk of cardiovascular
disease: prospective cohort study (NutriNet-Santé)" (2019) and here is the
graphical version of their findings.
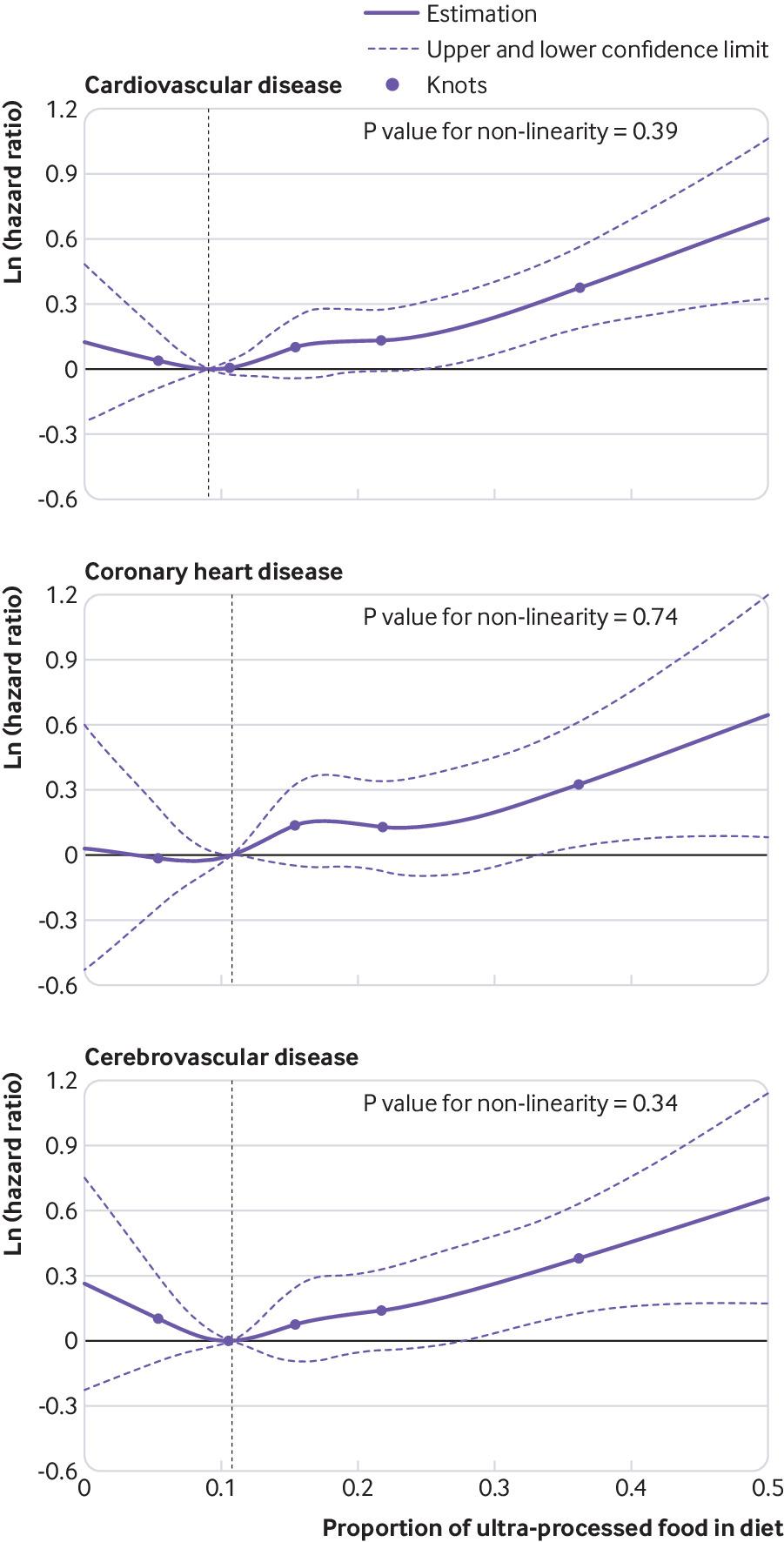
"In this large observational
prospective study, higher consumption of ultra-processed foods was associated
with higher risks of cardiovascular, coronary heart, and cerebrovascular
diseases."
https://www.bmj.com/content/365/bmj.l1451 [2669]
"Ultra-processed food consumption,
cancer risk and cancer mortality: a large-scale prospective analysis within the
UK Biobank" in the Lancet (2023) found similar results.:
"The mean UPF consumption was 22.9%
(SD 13.3%) in the total diet. During a median follow-up time of 9.8 years,
15,921 individuals developed cancer and 4009 cancer-related deaths occurred.
Every 10 percentage points increment in UPF consumption was associated with an
increased incidence of overall (hazard ratio, 1.02; 95% CI, 1.01–1.04) and
specifically ovarian (1.19; 1.08–1.30) cancer. Furthermore, every 10 percentage
points increment in UPF consumption was associated with an increased risk of
overall (1.06; 1.03–1.09), ovarian (1.30; 1.13–1.50), and breast (1.16;
1.02–1.32) cancer-related mortality."
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(23)00017-2/fulltext
[2667]
In a cohort study of 10,775
individuals followed for a median of 8 years, Goncalves et al (2022) found that
consumption of UPF greater than 19.9% of total daily calories was associated
with a faster decline in global cognitive performance and executive function.
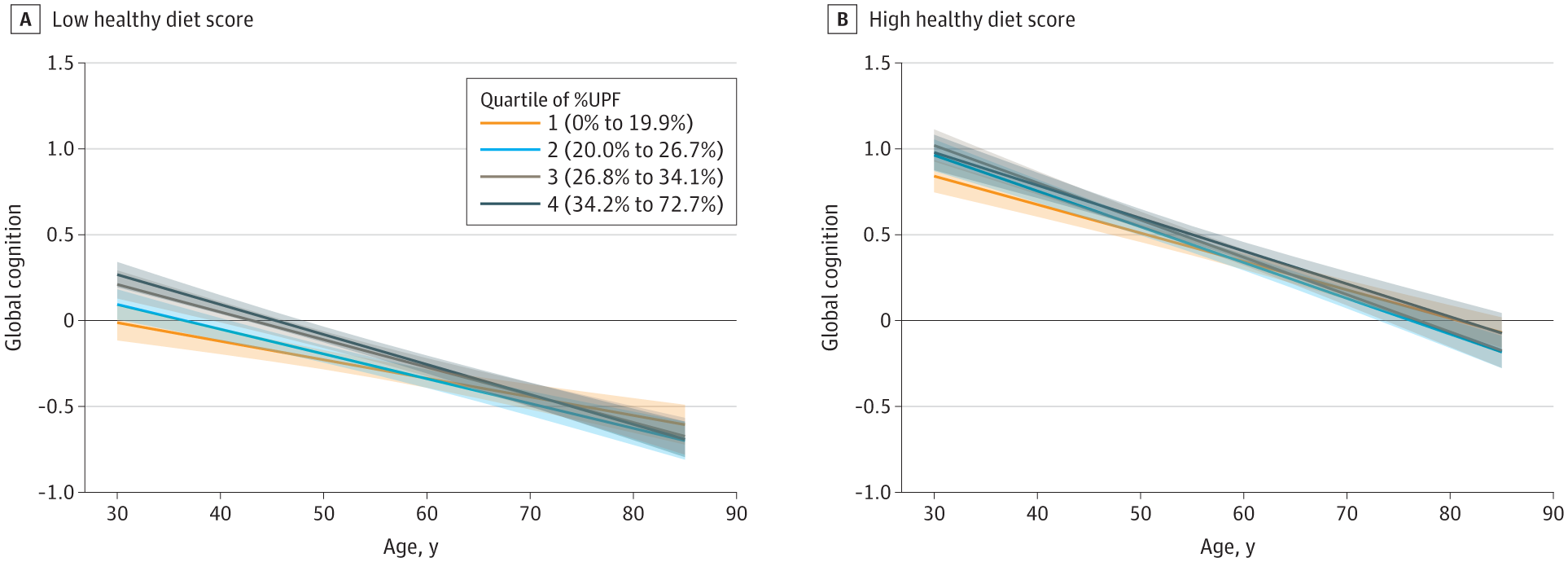
In particular, individuals with
ultraprocessed food consumption above the first quartile showed a 28% faster
rate of global cognitive decline and a 25% faster rate of executive function
decline compared with those in the first quartile.
https://jamanetwork.com/journals/jamaneurology/fullarticle/2799140 [5136]
Fructose is a cornerstone of the
ultra-processed food industry and humans have never consumed so much fructose
throughout human evolutionary history as they do today.
In 2009 Ross et al showed such a diet
produces impairments in a rat water maze model, revealing one possible reason
Americans elected Donald Trump twice:
"Over the past three decades there
has been a substantial increase in the amount of fructose consumed by North
Americans. Recent evidence from rodents indicates that hippocampal insulin
signaling facilitates memory and excessive fructose consumption produces
hippocampal insulin resistance. Based on this evidence, the present study tested
the hypothesis that a high fructose diet would impair hippocampal-dependent
memory. Adult male Sprague-Dawley rats (postnatal day 61) were fed either a
control (0 % fructose) or high fructose diet (60 % of calories). Food intake and
body mass were measured regularly. After 19 weeks, the rats were given 3 days of
training (8 trials/day) in a spatial version of the water maze task, and
retention performance was probed 48 h later. The high fructose diet did not
affect acquisition of the task, but did impair performance on the retention
test. Specifically, rats fed a high fructose diet displayed significantly longer
latencies to reach the area where the platform had been located, made
significantly fewer approaches to that area, and spent significantly less time
in the target quadrant than did control diet rats. There was no difference in
swim speed between the two groups. The retention deficits correlated
significantly with fructoseinduced elevations of plasma triglyceride
concentrations. Consequently, the impaired spatial water maze retention
performance seen with the high fructose diet may have been attributable, at
least in part, to fructose-induced increases in plasma triglycerides."
Some background:
"A high fructose diet causes numerous
pathological changes, including oxidative stress, glucose intolerance, insulin
resistance, type 2 diabetes, liver disease, hypertension, and cardiovascular
disease (Busserolles, Gueux, Rock, Mazur, and Rayssiguier, 2002; Elliott, Keim,
Stern, Teff, and Havel, 2002; Hwang, Ho, Hoffman, and Reaven, 1987; Montonen,
Jarvinen, Knekt, Heliovaara, and Reunanen, 2007; Nandhini, Thirunavukkarasu,
Ravichandran, and Anuradha, 2005; Zavaroni, Sander, Scott, and Reaven, 1980).
Furthermore, a study from one of the present investigators showed that the
damaging effects of a high fructose diet extend directly to the brain (Mielke,
Taghibiglou, Liu, Zhang, Jia, Adeli, and Wang, 2005). Specifically, placing male
Syrian hamsters on a 60 % fructose diet for 6 weeks produced hippocampal insulin
resistance. This finding is particularly significant given that the hippocampus
is integral to many forms of learning and memory (Ergorul and Eichenbaum, 2004)
and that converging lines of evidence indicate that neural insulin signaling
facilitates hippocampal-dependent memory (Park, 2001). For instance, extensive
evidence suggests that peripheral insulin resistance and type 2 diabetes are
associated with deficits in hippocampal-dependent declarative memory (Convit,
2005; Messier, 2005; Stewart and Liolitsa, 1999; Strachan, Deary, Ewing, and
Frier, 1997; Zhao, Chen, Xu, Moore, Meiri, Quon, and Alkon, 1999). Moreover,
learning and memory of a spatial water maze experience are correlated with
activation of the hippocampal insulin signaling pathway (Dou, Chen, Dufour,
Alkon, and Zhao, 2005; Zhao et al., 1999). Most importantly, direct infusions of
insulin into the hippocampus enhance performance in a variety of memory tasks,
and the memory-enhancing effects of hippocampal insulin administration are not
observed in diabetic rats (Babri, Gholamipour, Rad, and Khameneh, 2006; McNay,
Herzog, McCrimmon, and Sherwin, 2005; Moosavi, Naghdi, Maghsoudi, and Zahedi
Asl, 2006).
"Given that fructose is
preferentially metabolized by the liver into lipids (Havel, 2005; Topping and
Mayes, 1971) and produces large increases in plasma triglyceride (TG)
concentrations (Basciano, Federico, and Adeli, 2005; Havel, 2005; Kelley, Allan,
and Azhar, 2004; Le, Faeh, Stettler, Ith, Kreis, Vermathen, Boesch, Ravussin,
and Tappy, 2006; Park, Cesar, Faix, Wu, Shackleton, and Hellerstein, 1992), a
high fructose diet is analogous to a high fat diet in many metabolic ways.
Importantly, rats fed a diet high in saturated fatty acids exhibit impaired
performance on a number of hippocampal-dependent memory tasks (Greenwood and
Winocur, 1990; 1996; McNay et al., 2005). Moreover, high fat diets produce
insulin resistance in the brain (Banas, Rouch, Kassis, Markaki, and Gerozissis,
2008), and injecting TGs directly into the brain ventricles impairs memory
(Farr, Yamada, Butterfield, Abdul, Xu, Miller, Banks, and Morley, 2008).
Collectively, the reviewed evidence led us to hypothesize that a high fructose
diet would impair hippocampal-dependent memory, and that the deficits would be
attributable, at least in part, to fructose-induced increases in plasma TGs.
Consequently, the present experiment tested the effects of feeding rats a high
fructose diet on hippocampaldependent spatial water maze learning and memory,
and sought to determine whether any deficits would be correlated with
fructose-induced increases in plasma TGs."
https://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC2737072&blobtype=pdf
[3667]
Such ingredients are all but
impossible to avoid in today's society if you want to live a more-or less normal
life. More efficient use of food value may be one of the most valuable
(subliminal) positive outcomes, since food availability has grown immensely
during the last century, but nutritional content has fallen just as
dramatically.
According to Workinger et al in
"Challenges in the Diagnosis of Magnesium Status" (2018)
"Many fruits and vegetables have lost
large amounts of minerals and nutrients in the past 100 years with estimates
that vegetables have dropped magnesium levels by 80–90% in the U.S. (Figure 2)
and the UK [cited include USDA ]. It is important to note that the USDA mineral
content of vegetables and fruits has not been updated since 2000, and perhaps
even longer, given that the data for 1992 was not able to be definitively
confirmed for this review. The veracity of the mineral content to support the
claim of demineralization of our food sources should be verified, particularly
since farming methods and nutrient fertilization has undoubtedly advanced in the
last 50 years."
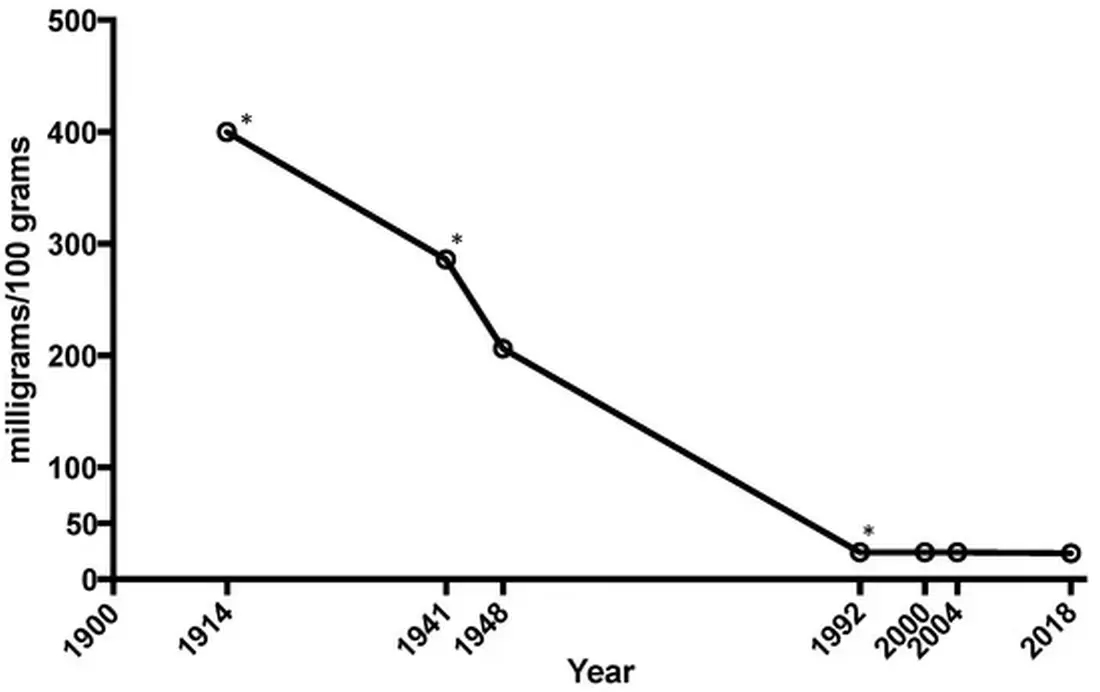
https://www.mdpi.com/2072-6643/10/9/1202 [2795]
"Magnesium is a cofactor in >300
enzymatic reactions. Magnesium critically stabilizes enzymes, including many
ATP-generating reactions. ATP is required universally for glucose utilization,
synthesis of fat, proteins, nucleic acids and coenzymes, muscle contraction,
methyl group transfer and many other processes, and interference with magnesium
metabolism also influences these functions. Thus, one should keep in mind that
ATP metabolism, muscle contraction and relaxation, normal neurological function
and release of neurotransmitters are all magnesium dependent. It is also
important to note that magnesium contributes to the regulation of vascular tone,
heart rhythm, platelet-activated thrombosis and bone formation."
And their Table 3 lists a few of the
enzyme functions...
Kinases B
Hexokinase
Creatine kinase
Protein kinase
ATPases or GTPases
Na+ /K+-ATPase
Ca2+-ATPase
Cyclases
Adenylate cyclase
Guanylate cyclase
Direct enzyme activation
Phosphofructokinase
Creatine kinase
5-Phosphoribosyl-pyrophosphate
synthetase
Adenylate cyclase
Na+/ K+-ATPase
...membrane functions...
Cell adhesion
Transmembrane electrolyte flux
...as a calcium antagonist...
Muscle contraction/relaxation
Neurotransmitter release
Action potential conduction in nodal
tissue
...and with structural functions
in...
Proteins
Polyribosomes
Nucleic acids
Multiple enzyme complexes
Mitochondria
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4455825/ [2796]
The Defendant therefore believes that
the nutritional quality of mass-produced foods has declined as the quantity has
increased, and that this is not against the interests of the producers. Indeed
isn't the western deity of all our beverages full of empty calories?
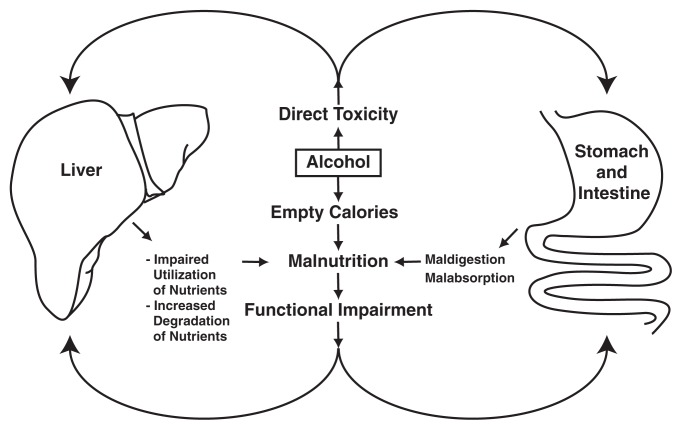
As Lieber points out:
"Nutritional approaches can help
prevent or ameliorate alcoholic liver disease. For example, a complete balanced
diet can compensate for general malnutrition."
and
"Pure alcohol provides approximately
7.1 kilocalories per gram (kcal/g), compared with 4 kcal/g for carbohydrates.
Thus, a 12-oz can of beer contains approximately 100 calories.
"At least under certain conditions,
however, alcohol-derived calories when consumed in substantial amounts can have
less biologic value than carbohydrate-derived calories, as shown in a study in
which Pirola and Lieber (1972) compared the weights of two groups of
participants who received balanced diets containing equal numbers of calories.
In one of the groups, 50 percent of total calories was derived from
carbohydrates, whereas in the other group the calories were derived from
alcohol.
"Although all participants received
the same number of calories, those in the alcohol group exhibited a decline in
body weight compared with those in the carbohydrate group. Moreover, when the
participants received additional calories in the form of alcohol, they did not
experience any corresponding weight gain. This suggests that some of the energy
contained in alcohol is 'lost' or 'wasted'—that is, it is not available to the
body for producing or maintaining body mass. Under other conditions, however,
alcohol-derived calories have the same biologic value as calories derived from
other nutrients. The various mechanisms involved and the circumstances in which
alcohol calories fully count or do not count are described in detail elsewhere
(Lieber 1991a).
"Several mechanisms have been
implicated in the apparent loss of alcohol-derived energy (Feinman and Lieber
1998). For example, some of the energy may be used up (wasted) during the
breakdown of alcohol by a pathway known as the microsomal ethanol-oxidizing
system (MEOS). (For more information on this system, see the section
'Relationships Between Nutritional Factors and Alcohol Metabolism,' below.) As
described later in this article, alcohol may damage the liver cells’
mitochondria—small membrane-enclosed cell structures that serve as the cell’s
power plants—and these damaged mitochondria may waste energy during the
breakdown of fats." [787]
In fact
"Researchers worldwide published a
record 4,300+ scientific papers on the subject of cannabis, according to the
results of a keyword search of the National Library of Medicine/PubMed.gov
website.
"This exceeds the total number of
papers published during all of last year [i.e. 2021], when scientists published
over 4,200 papers. At the time, that total was the highest number of
cannabis-specific papers ever published in a single year.
"Since 2010, scientists have
published over 30,000 peer-reviewed papers specific to cannabis, with the annual
number of total papers increasing every year. By comparison, researchers
published fewer than 3,000 total papers about marijuana in the years between
1990 and 1999 and fewer than 2,000 total studies during the 1980s.
"'Despite claims by some that
marijuana has yet to be subject to adequate scientific scrutiny, scientists’
interest in studying cannabis has increased exponentially in recent years, as
has our understanding of the plant, its active constituents, their mechanisms of
action, and their effects on both the user and upon society,' NORML’s Deputy
Director Paul Armentano said. 'It is time for politicians and others to stop
assessing cannabis through the lens of "what we don’t know" and instead start
engaging in evidence-based discussions about marijuana and marijuana reform
policies that are indicative of all that we do know.'"
https://norml.org/blog/2022/12/27/record-number-of-science-papers-published-about-cannabis-in-2022/
[2064]
In 1991, what did the Slovenian
inheritors of the international drug treaties of 1925, 1961 and 1971 know about
the anti-emetic properties of cannabis?
Let us take a note of the dates of
some papers referred to "Regulation of nausea and vomiting by cannabinoids and
the endocannabinoid system" from North American authors Sharkey et al (2013):
"In clinical trials, cannabis-based
medicines have been found to be effective anti-emetics and even surpass some
modern treatments in their potential to alleviate nausea (Cotter, 2009; Tramèr
et al., 2001). However, it was not until the early 1990s that the mechanism of
action of cannabis was established following the cloning of the “cannabinoid”
(CB) receptors (Howlett et al., 2002; Pertwee et al., 2010). The significance of
this discovery was enhanced when it was realized that these receptors were part
of an endogenous cannabinoid (endocannabinoid) system in the brain and elsewhere
in the body (Di Marzo and De Petrocellis, 2012; Izzo and Sharkey, 2010;
Mechoulam and Parker 2013; Piomelli, 2003). The endocannabinoid system serves to
modulate the expression of nausea and vomiting when activated by central or
peripheral emetic stimuli (Darmani and Chebolu, 2013; Parker et al., 2011)."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3883513/ [2043]
Does the Town Smell make me nauseous?
I am not Slovenian, so yes.
If you had asked any of the authors
of these international drug treaties, or the authors of the ZPPPD, about the
effects of banning cannabis for people affected by Ptuj Town Smell or other
nauseating experiences such as imbalances in microbiota caused by alcohol
consumption or undesirable ratios of exogenous lipids in foodstuffs on the
marketplace, they wouldn't have been able to refer to any of these papers would
they?
But what do you think they would have
said if you had asked them?
If you had gone to them and said,
look, we've got people feeling queasy every time they go out of the house. We've
got this Town Smell in Ptuj and we just can't do without it. We just can't stop
it, they say, and you say why not. And they say "Because it's Ptuj."
So you say, well what about smoking
cannabis to reduce the nausea and also block out the smell seeping into your
home? What would they say?
When the ZPPPD was introduced, would
the authors have been able to take into account results showing
"...that perturbation of bile acid
homeostasis upon alcohol exposure is mediated by activation of Cb1r and its
downstream effectors like phosphorylation of JNK signaling pathway and
subsequent activation of Crebh."
or
" that under normal conditions
insulin plays a crucial role in maintaining bile acid homeostasis via regulation
of Crebh transcriptional activity."
https://www.researchgate.net/publication/253336408_Hepatic_Cannabinoid_Receptor_Type_1_Mediates_Alcohol-Induced_Regulation_of_Bile_Acid_Enzyme_Genes_Expression_Via_CREBH/link/00b7d5200f5e64016f000000/download
[2046]
That was 2013. The experts you
believe in already know about that in 1925, 1961 or 1971 or 1991 or when the
ZPPPD was written in 1999?
And they couldn't have known in 1999
that
"Clearly, low doses of CB1 agonists
(0.5 mg/kg Δ9-THC, Limebeer and Parker, 1999; 0.001–0.01 HU-210, Parker et al.,
2003) attenuate nausea in the conditioned gaping model, an effect that is
reversed by rimonabant (see Parker et al., 2011). At low doses (1–5 mg/kg, i.p.)
the nonpsychoactive phytocannabinoid, CBD, also reduces these nausea-induced
behaviors (without affecting any measures of motor activity) by its action as an
indirect agonist of 5-HT1A receptors in the dorsal raphe nucleus (Rock et al.,
2012; Parker et al., 2011). By acting as an agonist of the somatodendritic
5-HT1A autoreceptors located in the dorsal raphe, CBD would be expected to
reduce the release of 5-HT in forebrain regions (e.g. possibly the interoceptive
insular cortex, Tuerke et al., 2012a) to ultimately suppress toxin-induced
nausea." [2043]
As the authors explain:
"These contextually elicited
conditioned gaping or retching reactions represent animal models of anticipatory
nausea analogous to that experienced by human chemotherapy patients, which can
be produced following 3–4 conditioning trials. In human chemotherapy patients,
when anticipatory nausea develops, the classic anti-emetic agent ondansetron is
ineffective in reducing this symptom (Hickok et al., 2003); likewise rats and
shrews pretreated with ondansetron do not show a suppression of
contextually-elicited gaping and retching reactions, respectively (Limebeer et
al., 2006; Parker and Kemp, 2001; Parker et al., 2006; Rock et al., 2008). On
the other hand, Δ9- THC, URB597 and CBD all reduce these contextually-elicited
conditioned nausea reactions (Parker et al., 2011). More recently, it has been
shown that CBDA (Bolognini et al., 2012) were more potent than CBD and Δ9-THC
respectively in attenuation of contextually-elicited conditioned gaping in rats.
CBDA potently suppresses nausea and vomiting in a 5-HT1A receptor dependent
manner (Bolognini et al., 2012). Since these compounds are both
non-psychoactive, they are promising candidates for the treatment of
anticipatory nausea, as there is no current therapeutic available once
anticipatory nausea does develop. Currently, patients are given non-specific
anti-anxiety drugs."
The authors do not explain why they
think these psychoactive properties are unwanted. They may be unwanted. Or they
may be a bonus. People do have the right to buy decaf and alkoholfrei also. The
takeup is not great.
It's not up to these researchers to
decide people shouldn't be happy as well as enjoying these particular benefits
of, but not limited to, CBDA, which by the way is not available as an
anti-nausea drug in Slovenia anyway, except as one of many useful components of
cannabis.
The authors seem happy to have
discovered a component incapable of making the patient happy. And the experts
you believe in couldn't have known that as of 2016 that
"The integrity of the gastric mucosa
is maintained due to a balance between ‘mucosal aggressive factors’ and the so
called ‘gastric mucosal protective mechanisms’. The gastric mucosa is constantly
exposed to high concentrations of luminal acid. Other aggressive factors in the
lumen are pepsins, bile refluxed from incompetent pyloric sphincter, bacteria,
ethanol and drugs especially the non-steroidal anti-inflammatory drugs (NSAIDs)
capable of inhibiting the synthesis of cytoprotective prostaglandins. The
mucosa's ability to withstand acid and other injurious agents is due to several
mechanisms collectively is known as the gastric mucosal barrier. The
mucus-bicarbonate layer together with surface-active phospholipids barrier
constitute the first line of defence or the pre-epithelial barrier. The surface
epithelial cells capable of rapid turnover and migration (restitution) and
releasing mucins, bicarbonate, phospholipids, prostaglandins, trefoil peptides
form the second line of defence. Other important defence mechanisms of gastric
mucosa are cytoprotective prostaglandins, mucosal sulfhydryl content, adequate
mucosal blood flow, and sensory afferent innervations. The development of
gastric mucosa damage implies a breach in the balance between aggressive and
defencive factor."
They couldn't have known anything
about the mechanisms by which cannabis strengthens gastric mucosal defences?
"Several mechanisms are likely to
account for the ability of Cannabis or individual cannabinoid agonists to
protect the stomach against noxious injury. Cannabis and/or individual
cannabinoids inhibit gastric acid secretion, thereby, lessening the ability of
this most powerful aggressive factor to threaten the gastric mucosa. Studies
also indicated that Cannabis administration increases mucus secretion in the
gastric mucosa. Mucus is secreted by the mucous neck and surface epithelial
cells and plays an important role in protecting the surface epithelial cells
from luminal acid and other injurious agents. Mucus retards diffusion of luminal
acid into the mucosa and together with bicarbonate secreted by the epithelium
forms a pH gradient with near-neutral pH at the surface of the mucosa.
"Luminal pepsins constitute an
important aggressive factor capable of digesting mucus and thereby increasing
the susceptibility of gastric mucosa to other injurious factors. Studies in
pylorus-ligated rats treated with Cannabis extract for 4 weeks indicated that
Cannabis did not affect basal pepsin secretion. Cannabis, however, decreased
pepsin secretion when the stomach is stimulated with pentagastrin and carbachol.
Cannabis also decreased pepsin secretion following ethanol administration in
rats.
"Reactive oxygen intermediates have
been implicated in the development of gastric mucosal injury due to
ischaemia/reperfusion, ethanol, NSAIDs, and bacteria. Cannabis has been shown to
decrease lipid peroxidation and to increase reduced glutathione content and
catalase activity in gastric mucosa. Cannabis also inhibited mucosal nitric
oxide. Although a vasodilator effect of physiological concentrations of nitric
oxide help the mucosa to withstand noxious challenge, high concentrations are
likely to have a damaging effect. Cannabis thus might protect the gastric mucosa
by virtue of an antioxidant action.
"Mucosal inflammation plays an
important role in the development of gastric ulcers and although initial
inflammatory response to the gastric mucosa helps to minimize or limit tissue
damage, an exaggerated or uncontrolled response is detrimental to the mucosal
integrity. Cannabis has been shown to inhibit the pro-inflammatory cytokine
tumour necrosis factor-alpha in mucosal homogenates, an action which might help
to minimize the extent of mucosal damage.
"Cannabis thus exerts antioxidant and
anti-inflammatory effects in the gastric mucosa. It is to be noted, however,
that these actions of Cannabis were evident only when the gastric mucosa was
challenged with increased acid secretion or after exposing the mucosa to noxious
agents such as acidified aspirin and ethanol and were not apparent under basal
conditions.
"One important factor in determining
the ability of the gastric mucosa to resist gastric acid and other noxious
agents is gastric mucosal blood flow. This has been inferred from studies
showing that interference with the blood supply to the mucosa i.e. ischaemia
resulted in the development of gastric mucosal damage or aggravated the extent
of mucosal damage evoked by NSAIDs or ethanol On the other hand, agents which
increase gastric mucosal blood flow such as isoproterenol, vasodilator
prostaglandins or capsaicin-type agents helped to protect against noxious
challenge. In this context, data have been provided that the endocannabinoid
anandamide increases gastric mucosal blood flow. There is also an evidence for a
vaso-relaxant action for methanandamide in rat gastric arteries. This effect was
independent of cannabinoid receptors. It is thus possible that a vasodilatory
action is involved in the gastric protective effects of Cannabis and or
cannabinoids."
https://www.sciencedirect.com/science/article/pii/S1995764516300712#bib54
[2047]
So now you're a bit more up to date
on the role cannabis can play in these gastric mucosal protective mechanisms, at
least up to May 2016, do you say this has all been considered and taken into
account in your operations under the ZPPPD?
Now if cannabis helps gastric mucosal
protective mechanisms, and someone has some cannabis and Mr Teodorovic or the
Police or the Republic of Slovenia steal or confiscate someone's cannabis, or a
population's cannabis, what would you expect the effect would follow from the
removal of that cannabis on those gastric mucosal protective mechanisms on that
person or population?
In fact it would be worse for a
population than a single person, wouldn't it?
And there would be no difference
between it being taken by a burglar or by the government, would it?
Since 2016 how long have Slovenia's
experts had to investigate these negative effects of the ZPPPD on gastric
mucosal protective mechanisms?
And what evidence can you offer about
these investigations?
What do you think the authors of the
international drug control treaties would have said at the time about cannabis
and gut motility?
Wasn't the British Empire
pro-dysentery, pro-cholera, for the black people?
Surely it would have been their own
fault in colonial India? Would they have tried cannabis to treat dysentery in
white patients?
Staff Surgeon S J Rennie of the
Cawnpore (now Kanpur) Hospital reports unanimous success with treatment in a
dozen or more such individuals, reporting four of his case histories in detail
in the Indian Medical Gazette in December 1886 under the title "On the
Therapeutic Value of Tinctura Cannabis Indica in the Treatment of Dysentery".
https://pmc.ncbi.nlm.nih.gov/articles/PMC5000962/ [4883]
General Smuts could not have known,
could he, that as reported by Izzo et al in the AGA journal Gastroenterology in
2003:
"Previous studies have shown that
activation of enteric CB1 inhibits esophageal and gastrointestinal motility,
including in isolated human tissues, and in an experimental model of diarrhea in
the mouse. In this study, we were able to show that the nonselective cannabinoid
receptor agonist CP55,940 and the selective CB1 receptor agonist ACEA decreased
CT-stimulated fluid accumulation in the mouse small intestine. The antidiarrheal
effect of the cannabinoid agonists examined here is very likely mediated
uniquely by CB1 receptors because: (1) the effect of both CP55,940 and ACEA was
counteracted by the selective CB1 receptor antagonist SR141716A; (2) the CB2
receptor antagonist SR144528 did not modify the antisecretory effect of
CP55,940; (3) the CB1 selective agonist ACEA reduced CT-stimulated fluid
accumulation; and (4) the CB2 receptor agonist JWH-015 was without effect."
https://www.gastrojournal.org/article/S0016-5085(03)00892-8/fulltext [4884]
Statistics strongly supportive of an
association between marijuana use and improved gut motility can be found in a
nationwide US survey of 9645 adults 20-59 in 2019 by North Shore Medical Center,
Salem, Massachusetts and Massachusetts General Hospital, Boston:
"Recent MJ use was associated with a
30% decreased odds of constipation (crude odds ratio: 0.71 [0.56–0.98], P =
0.005), which persisted after stepwise adjustment for age and other demographic
factors including sex, ethnicity, education, body mass index, and socioeconomic
status (AOR: 0.64 [0.49–0.83], P = 0.001); comorbidities, substance use
(alcohol, tobacco, heroin, and cocaine), constipating medications, general
health condition, rigorous physical activity, and emotional disturbances (AOR:
0.68 [0.48–0.93], P = 0.016); and diet (AOR: 0.68 [0.52–0.89], P = 0.006). There
was no association between recent MJ use and diarrhea."
https://journals.lww.com/ajg/Abstract/2019/12000/Relationship_Between_Recreational_Marijuana_Use.15.aspx
[785]
In "The effects of D9
-tetrahydrocannabinol and cannabidiol alone and in combination on damage,
inflammation and in vitro motility disturbances in rat colitis" (2010) by
Jamontt et al at the School of Life Sciences, University of Hertfordshire
"The 2,4,6-trinitrobenzene sulphonic
acid (TNBS) model of acute colitis in rats was used to assess damage,
inflammation (myeloperoxidase activity) and in vitro colonic motility.
Sulphasalazine was used as an active control drug.
"Key results: Sulphasalazine, THC and
CBD proved beneficial in this model of colitis with the dose-response
relationship for the phytocannabinoids showing a bell-shaped pattern on the
majority of parameters (optimal THC and CBD dose, 10 mg.kg(-1)). THC was the
most effective drug. The effects of these phytocannabinoids were additive, and
CBD increased some effects of an ineffective THC dose to the level of an
effective one. THC alone and in combination with CBD protected cholinergic
nerves whereas sulphasalazine did not.
"Conclusions and implications: In
this model of colitis, THC and CBD not only reduced inflammation but also
lowered the occurrence of functional disturbances. Moreover the combination of
CBD and THC could be beneficial therapeutically, via additive or potentiating
effects."
https://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC2931570&blobtype=pdf
[2939]
In a murine colitis model, Yekhtin et
al (2022) found "Differential Effects of D9 Tetrahydrocannabinol (THC)- and
Cannabidiol (CBD)-Based Cannabinoid Treatments on Macrophage Immune Function In
Vitro and on Gastrointestinal Inflammation in a Murine Model" and this was the
Dextran sulfate sodium (DSS)-induced colitis model. DSS is a sulfated
polysaccharide. Administration of DSS in mice causes human ulcerative
colitis-like pathologies due to its toxicity to colonic epithelial cells, which
results in compromised mucosal barrier function.
"...aimed to evaluate the effects of
the phytocannabinoids D9 tetrahydrocannabinol (THC) and cannabidiol (CBD) on
macrophage activation. Macrophages from young and aged C57BL/6 mice were
activated in vitro in the presence of pure cannabinoids or cannabis extracts.
The phenotype of the cells, nitric oxide (NO•) secretion, and cytokine secretion
were examined."
The treated mice did well and
"We identified higher activity of
cannabis extracts as compared with pure cannabinoids. Each treatment had a
unique effect on cytokine composition. Overall, our results establish that the
effects of cannabinoid treatments differ."
They explain
"Immunological dysregulation in IBD
is characterized by epithelial damage, expansion of inflammation driven by
intestinal flora, a large number of cells infiltrating into the lamina propria,
and a failure of immune regulation to control the inflammatory response. In IBD
patients, the number of macrophages increase in the inflamed mucosa."
and
"Phytocannabinoids, the biologically
active constituents of cannabis, possess a wide range of immune regulatory
properties, mediated by the endocannabinoid system."
and as regards the two best known:
"D9 tetrahydrocannabinol (THC) and
cannabidiol (CBD). THC and some of the other phytocannabinoids mediate their
biological effects primarily through the classical cannabinoid receptors CB1 and
CB2. In addition, THC can act as an agonist of the receptors/channels GPR55,
GPR18, PPARγ, transient TRPA1, TRPV2, TRPV3, and TRPV4, and as an antagonist of
the receptors/channels TRPM8 and 5-HT3A. Interestingly, although CBD affects the
immune function, it has a very weak affinity to CB2 or CB1, where it can act as
a negative allosteric modulator. Several reports have demonstrated that CBD acts
as an agonist of other receptors/channels, such as TRPA1, TRPV1, TRPV2, TRPV3,
PPARγ, and 5-HT1A, and as an antagonist of the receptors GPR55, GPR18, and
5-HT3A. CBD is also an inverse agonist of the receptors GPR3, GPR6, and GPR12."
and again
"Cannabis extracts and pure
cannabinoids were used in a concentration of 5 µg/mL; the extracts had stronger
effect than the pure cannabinoids, although cannabinoids constituted only 35–38%
of their content. This could result either from inhibitory signaling of other
molecules in the plant (not THC/CBD) or from a synergistic function of THC/CBD
with other molecules."
and broadly their results showed
"Cannabinoid Treatments Reduce Nitric
Oxide and Cytokine Production of LPS-Activated Peritoneal
Macrophages....Cannabinoid Treatments Affect the Phenotype of Activated
Peritoneal Macrophages....Cannabis Extracts Have Improved Effect in Murine
Colitis DSS Model Mice as Compared with Pure Cannabinoids....Cannabinoid
Treatments Reduce Intestinal Macrophage Infiltration and the Levels of
Inflammatory Cytokines in the Plasma of DSS Mice".
https://www.mdpi.com/2227-9059/10/8/1793/pdf?version=1658831384 [2938]
For Becker et al (2020) one model of
colitis was not enough.
"Female C57BL/6 mice were treated
with either cannabidiol [CBD], Δ 9-tetrahydrocannabinol [THC], a combination of
CBD and THC, or vehicle, in several models of chemically induced colitis.
Clinical parameters of colitis were assessed by colonoscopy, histology, flow
cytometry, and detection of serum biomarkers; single-cell RNA sequencing and
qRT-PCR were used to evaluate the effects of cannabinoids on enterocytes. Immune
cell transfer from CB2 knockout mice was used to evaluate the contribution of
haematopoietic and non-haematopoietic cells to colitis protection.
"Results: We found that THC prevented
colitis and that CBD, at the dose tested, provided little benefit to the
amelioration of colitis, nor when added synergistically with THC. THC increased
colonic barrier integrity by stimulating mucus and tight junction and
antimicrobial peptide production, and these effects were specific to the large
intestine. THC increased colonic Gram-negative bacteria, but the anti-colitic
effects of THC were independent of the microbiome. THC acted both on immune
cells via CB2 and on enterocytes, to attenuate colitis."
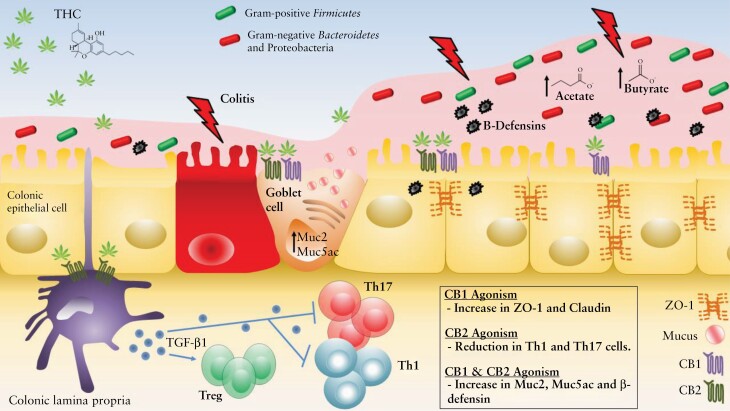
"Conclusions: Our findings
demonstrate how cannabinoid receptor activation on both immune cells and
colonocytes is critical to prevent colonic inflammation. These studies also
suggest how cannabinoid receptor activation can be used as a preventive and
therapeutic modality against colitis."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8218712/ [2940]
From the Institute of Experimental
and Clinical Pharmacology, Medical University of Graz, a summary of important
and recent findings on the role of cannabinoid receptors and their ligands in
the GI tract with emphasis on GI disorders, such as irritable bowel syndrome,
inflammatory bowel disease and colon cancer:
"In ancient medicine, extracts of the
marijuana plant Cannabis sativa were used against diseases of the
gastrointestinal (GI) tract....After many anecdotal reports suggested beneficial
effects of Cannabis in GI disorders, it was not surprising to discover that the
GI tract accommodates and expresses all the components of the ECS. Cannabinoid
receptors and their endogenous ligands, the endocannabinoids, participate in the
regulation of GI motility, secretion, and the maintenance of the epithelial
barrier integrity. In addition, other receptors, such as the transient receptor
potential cation channel subfamily V member 1 (TRPV1), the peroxisome
proliferator-activated receptor alpha (PPARα) and the G-protein coupled receptor
55 (GPR55), are important participants in the actions of CBs in the gut and
critically determine the course of bowel inflammation and colon cancer."
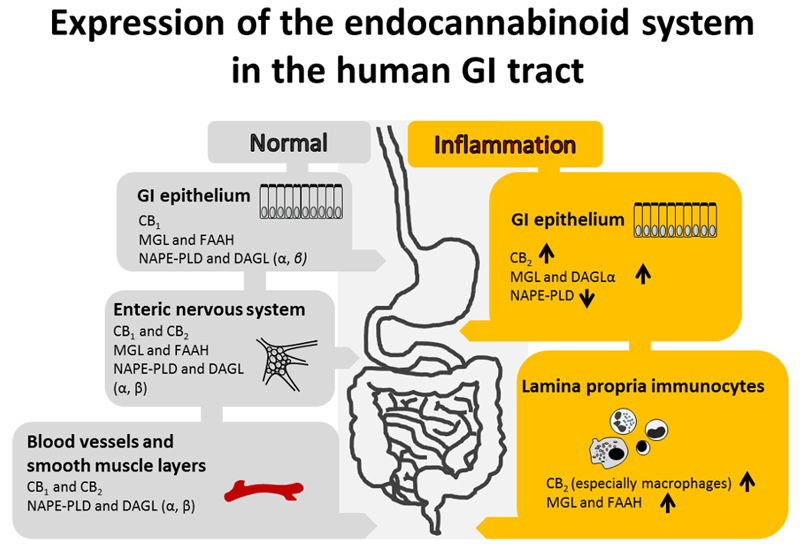
"The FAAH enzyme...seems to be a key
molecule for the regulation of endocannabinoid levels and colon motility, but
not for GI pain sensation."
"So far, the human studies indicate
increased endocannabinoid activity in colon cancer while the role of CB
receptors remains less clear.
"Cannabinoids reduce carcinogenesis
in animal models of colon cancer"
"The GI tract is one of the regions
where cannabinoid signaling is involved in many physiological and
pathophysiological regulatory mechanisms, this is now clearly understood."
"From a scientist's perspective and
all the caveats in mind, it seems to be a matter of time when cannabinoid
compounds will be used in the treatment of GI disease."
%20cannabinoids%20exert%20various%20anti-tumorigenic%20effects%20in%20colon%20cancer...see%20pic%20anti%20cancer%20effects%20433.jpg)
"A large number of studies have
confirmed that the ECS is crucially involved in the control of motility,
secretion and mucosal integrity of the gut and may even determine the course of
intestinal inflammation and cancer."
"From a scientist's perspective and
all the caveats in mind, it seems to be a matter of time when cannabinoid
compounds will be used in the treatment of GI disease."
Just hang on, they're saying. They
might be able to agree with something involving cannabis during my lifetime,
just don't go doing anything like treating yourself without them.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5130148/ [433]
And from a 2021 review:
"A database search of peer reviewed
articles published in English as full texts between January 1970 and April 2021
in Google Scholar, MEDLINE, PubMed and Web of Science was undertaken. References
of relevant literature were searched to identify additional studies to construct
a narrative literature review of oncological effects of cannabinoids in
pre-clinical and clinical studies in various cancer types.
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8310855/ [5131]
In 2018 Ferro et al demonstrated a
threefold increase in survival in a mouse model of pancreatic cancer
"...inhibition of the G
protein-coupled receptor GPR55, using genetic and pharmacological approaches,
reduces pancreatic cancer cell growth in vitro and in vivo and we propose that
this may represent a novel strategy to inhibit pancreatic ductal adenocarcinoma
(PDAC) progression. Specifically, we show that genetic ablation of Gpr55 in the
KRASWT/G12D/TP53WT/R172H/Pdx1-Cre+/+ (KPC) mouse model of PDAC significantly
prolonged survival. Importantly, KPC mice treated with a combination of the
GPR55 antagonist Cannabidiol (CBD) and gemcitabine (GEM, one of the most used
drugs to treat PDAC), survived nearly three times longer compared to mice
treated with vehicle or GEM alone. Mechanistically, knockdown or pharmacologic
inhibition of GPR55 reduced anchorage-dependent and independent growth, cell
cycle progression, activation of mitogen-activated protein kinase (MAPK)
signalling and protein levels of ribonucleotide reductases in PDAC cells.
Consistent with this, genetic ablation of Gpr55 reduced proliferation of tumour
cells, MAPK signalling and ribonucleotide reductase M1 levels in KPC mice.
Combination of CBD and GEM inhibited tumour cell proliferation in KPC mice and
it opposed mechanisms involved in development of resistance to GEM in vitro and
in vivo. Finally, we demonstrate that the tumour suppressor p53 regulates GPR55
protein expression through modulation of the microRNA miR34b-3p."
https://www.nature.com/articles/s41388-018-0390-1 [1769]
THC was not tested in this paper.
"Cannabinoids in the landscape of
cancer" by Mangal et al (2021) presents in vitro and in vivo studies on
pancreatic adenocarcinoma:
"Phyto-, endogenous and synthetic
cannabinoids demonstrated antitumour effects both in vitro and in vivo. However,
these effects are dependent on cancer type, the concentration and preparation of
the cannabinoid and the abundance of receptor targets. The mechanism of action
of synthetic cannabinoids, (−)-trans-Δ9-tetrahydrocannabinol (Δ9-THC) and
cannabidiol (CBD) has mainly been described via the traditional cannabinoid
receptors; CB1 and CB2, but reports have also indicated evidence of activity
through GPR55, TRPM8 and other ion channels including TRPA1, TRPV1 and TRPV2.
"Cannabinoids have shown to be
efficacious both as a single agent and in combination with antineoplastic drugs.
These effects have occurred through various receptors and ligands and modulation
of signalling pathways involved in hallmarks of cancer pathology."
https://link.springer.com/content/pdf/10.1007/s00432-021-03710-7.pdf#page=6.32
[786]
In 2019, a "Flavonoid Derivative of
Cannabis Demonstrates Therapeutic Potential in Preclinical Models of Metastatic
Pancreatic Cancer"
"This study reports on a new
non-cannabinoid, non-psychoactive derivative of cannabis, termed FBL-03G, with
the potential to treat pancreatic cancer. In vitro results show major increase
in apoptosis and consequential decrease in survival for two pancreatic cancer
models- Panc-02 and KPC pancreatic cancer cells treated with varying
concentrations of FBL-03G and radiotherapy. Meanwhile, in vivo results
demonstrate therapeutic efficacy in delaying both local and metastatic tumor
progression in animal models with pancreatic cancer when using FBL-03G
sustainably delivered from smart radiotherapy biomaterials. Repeated experiments
also showed significant (P < 0.0001) increase in survival for animals with
pancreatic cancer compared to control cohorts.
https://www.frontiersin.org/articles/10.3389/fonc.2019.00660/full [2413]
At the University of Camerino, Zeppa
et al (2024) were less coy about the magic ingredient of their pancreatic cancer
treatment, with "Cannabigerol Induces Autophagic Cell Death by Inhibiting
EGFR-RAS Pathways in Human Pancreatic Ductal Adenocarcinoma Cell Lines":
"Immunoblots evidenced a decrease in
EGFR expression in PANC-1 with the higher dose of CBG, while, for MIAPaCa-2, the
reduction was significant with both doses (Figure 2A). Similar results were
obtained for mTOR protein expression, which was reduced especially after the
treatment with the highest dose of CBG (Figure 2A). Then, total Akt and its
phosphorylated form were investigated. Data showed a slight modulation of total
Akt protein with CBG at a dose of 11.06 μg/mL for PANC-1 cells and a reduction
of phospho-Akt (pAkt) levels after the administration of both CBG doses (Figure
2B). In MIAPaCa-2 cells, the highest dose of CBG induced a marked reduction of
total Akt and a significant decrease in its phosphorylation (Figure 2B)."
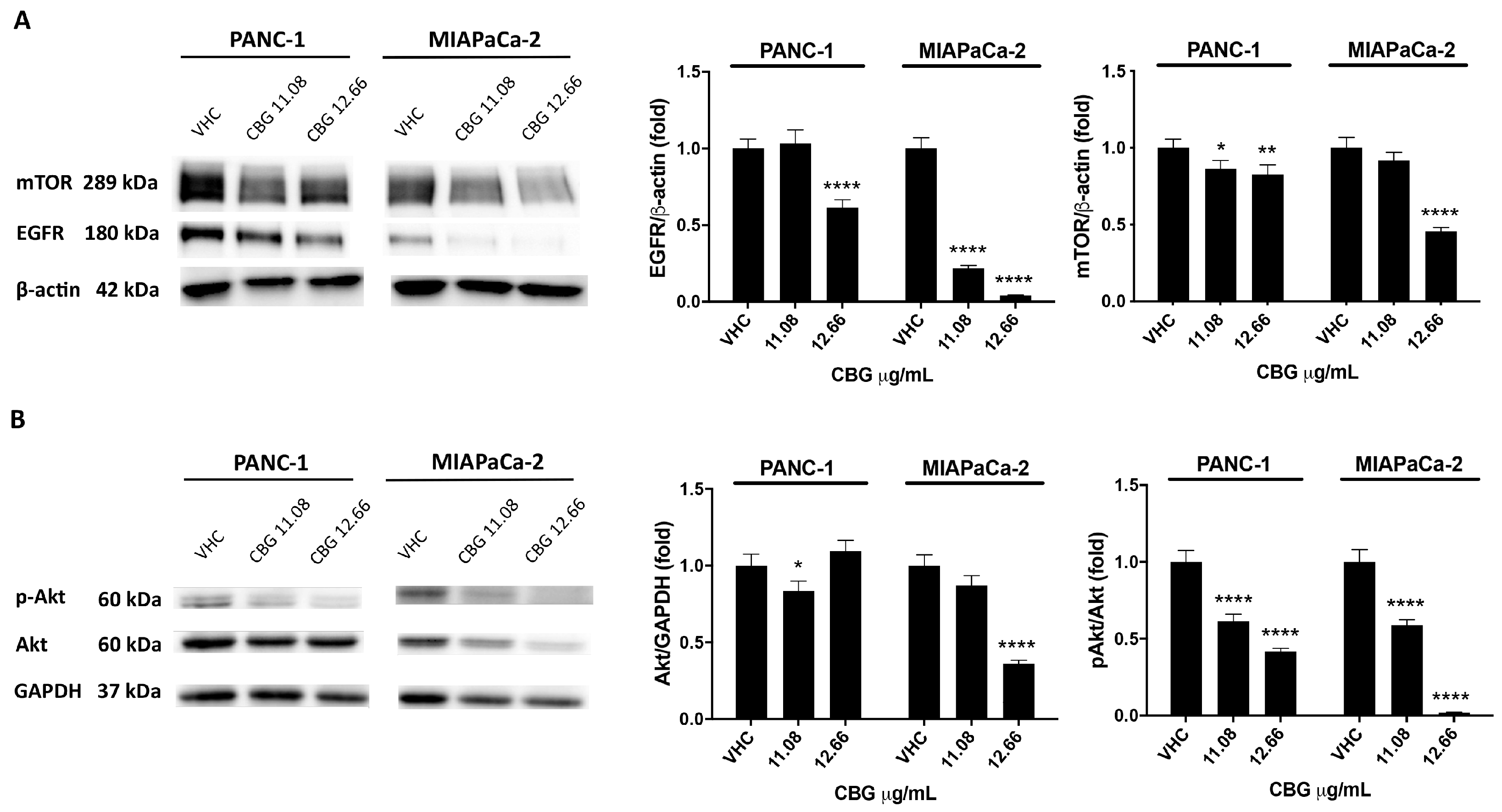
https://www.mdpi.com/1422-0067/25/4/2001 [3979]
While Turgut et al (2022) found
"Anti-cancer effects of selective cannabinoid agonists in pancreatic and breast
cancer cells":
"We found that selective CB1/2
agonists suppressed cell proliferation, clonogenicity and induced proapoptotic
function in human PANC1 pancreatic and MDA-MB-231 breast cancer cells. Based on
our findings, these agonists led to the inhibition of both cell viability and
clonogenic growth in a dose dependent manner. CB1/2 agonists were observed to
induce intrinsic apoptotic pathway by upregulating Bax, while downregulating
Bcl-2 expression levels."
https://www.elis.sk/download_file.php?product_id=7812&session_id=oh602ctcv1tfhp3l0hill6ql85
[4968]
In "Cannabinoids as Potential
Therapeutic Agents in the Treatment of Pancreatic Cancer" a review by Bimonte et
al (2025)...
"The search identified 46 studies,
with 19 meeting the inclusion criteria (14 preclinical and 5 clinical).
Preclinical studies revealed that cannabinoids, primarily Δ9‑
tetrahydrocannabinol (THC) and cannabidiol (CBD), exert anti‑tumor effects
through mechanisms such as apoptosis induction, cell cycle arrest, inhibition of
angiogenesis, immune modulation, and reduction of oxidative stress. Most
clinical studies emphasize cannabinoids’ role in symptom management rather than
direct anti‑cancer effects. A notable exception is a case series suggesting
improved survival in pancreatic cancer patients using CBD, though its
preliminary findings warrant further investigation."
https://ar.iiarjournals.org/content/anticanres/45/7/2719.full.pdf [5130]
In 2021 Sultan et al showed the
beneficial effects of anandamide (AEA) - and by implication phytogenic THC - in
lungs, colon and the mesenteric lymph nodes experimentally infected with
Staphylococcal enterotoxin B (SEB).
"Upon analysis of vascular and gut
leakage, we noted that anandamide significantly decreased the leakage in the
lungs (Figure 2D) and the gut (Figure 2E) in the SEB + AEA group, when compared
to the SEB + VEH group."
and
"To further investigate the effect of
AEA on gut-associated immune responses, we analyzed the effect of AEA on the
mesenteric lymph nodes (MLNs). The data showed that AEA significantly decreased
the percentage and absolute numbers of CD4 + T cells, CD8 + T cells, Vβ8 + T
cells, and NKT cells in the SEB + AEA group when compared to the SEB + VEH group
of mice (Figure 3A–D)."
and
"Because we noted significant
induction of AMPs [antimicrobial peptides] following AEA treatment, we next
investigated the microbial profile in the lungs and the gut following SEB
treatment. SEB treatment increased the abundance of microbiota in the lungs, and
AEA significantly reversed this, as shown using Chao1 rare fraction measure
(Figure 5A). Beta diversity analysis, which measured the similarity or
dissimilarity between various groups, showed that all three groups were well
separated, with the SEB + AEA group clustered away from the SEB + VEH group
(Figure 5B). Additionally, representatives of the orders of Caulobacterales and
Pseudomonodales were significantly decreased in the SEB + AEA group compared to
the SEB + VEH (Figure 5C,D). To distinguish significantly altered bacteria among
the three groups, linear discriminant analysis effect size (LEfSe) analysis
(Figure 6A) was performed and the corresponding cladogram (Figure 6B) was
generated. Data showed that there were several bacteria found to be distinctly
expressed in each of the three groups. Our LEfSe analysis of the lungs indicated
that beneficial bacteria, such as Muribaculaceae (s24-7), was indicated in the
SEB + AEA group only. Additionally, some beneficial bacteria, such as
Lachnospiraceae and Clostridia which produce butyrate, were indicated in the SEB
+ AEA group but not in the Naïve or the SEB + VEH group. Interestingly, some
pathogenic bacteria such as Pseudomonas and Enterobacteriaceae were indicated in
the SEB + VEH group only but not in the Naïve or SEB + AEA."
https://www.mdpi.com/2073-4409/10/12/3305 [2710]
The Major Histocompatibility Complex
(MHC) is the cellular machinery that flags tumor cells for the immune system.
However, most metastatic tumor cells have lost their MHC expression, and thus
escape immune system killing. Dada et al (2022) set out an explanation of why
"Specific cannabinoids revive adaptive immunity by reversing immune evasion
mechanisms in metastatic tumours":
"Fascinating ethnographic and
experimental findings indicate that cannabinoids inhibit the growth and
progression of several categories of cancer; however, the mechanisms underlying
these observations remain clouded in uncertainty. Here, we screened a library of
cannabinoid compounds and found molecular selectivity amongst specific
cannabinoids, where related molecules such as Δ9-tetrahydrocannabinol,
cannabidiol, and cannabigerol can reverse the metastatic immune escape phenotype
in vitro by inducing MHC-I cell surface expression in a wide variety of
metastatic tumours that subsequently sensitizing tumours to T lymphocyte
recognition. Remarkably, H3K27Ac ChIPseq analysis established that cannabigerol
and gamma interferon induce overlapping epigenetic signatures and key gene
pathways in metastatic tumours related to cellular senescence, as well as APM
genes involved in revealing metastatic tumours to the adaptive immune response.
Overall, the data suggest that specific cannabinoids may have utility in cancer
immunotherapy regimens by overcoming immune escape and augmenting cancer immune
surveillance in metastatic disease. Finally, the fundamental discovery of the
ability of cannabinoids to alter epigenetic programs may help elucidate many of
the pleiotropic medicinal effects of cannabinoids on human physiology."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10010394/ [4659]
All of these discoveries were of
course made up to eight decades after the last medicolegal assessment of
cannabis by the international forces of prohibition (1935).
The Court will observe that if I wait
as long as the United Nations took to discover that weed isn't like heroin, for
it to factor these discoveries about what I have been doing to myself for the
last 47 years into international law, by the time it percolates down to tell
Slovenia what the medical establishment wants it to do, I would be 123 years old
before being able to legally obtain a longer, healthier life, with less fat,
better immunity, and less cancer.
Slovenia can be the country that
fines people and drives them out of their homes for refusing to be fat, less
immune and more cancer-prone if it wants to. This obviously puts this drug laws
as currently imagined in conflict with the Constitution and laws to protect the
person in health matters.
If people have to go to the ECHR to
get their savings back from the bank, or get compensated for losing their house
over a 100 euro bill, or as in the case of the erased, to establish their
citizens' rights, you can obviously expect a challenge sooner or later to this
idea of punishing the self-infliction of better health.
I'm not a member of a Christian death
cult. I don't have any of the things cannabis prevents, and like any reasonable
person I will make the choices required to keep it that way.
While all these discoveries were
being made, prohibition continued in its peaceful slumbers, and weed was still
legally the same as heroin.
----------------------------------------------------------------------------
The Englishman stands
for the rights of everyone disadvantaged, discriminated against, persecuted, and
prosecuted on the false or absent bases of prohibition, and also believes the
victims of these officially-sanctioned prejudices have been appallingly treated
and should be pardoned and compensated.
The Englishman requests the return of his CaPs and other rightful property, for
whose distraint Slovenia has proffered no credible excuse or cause.
The Benedictions represent both empirical entities as well as beliefs. Beliefs
which the Defence evidence shows may be reasonably and earnestly held about the
positive benefits of CaPs at the population level, in which the good
overwhelmingly outweighs the bad. Below, the latest version of this dynamic
list.
THE BENEDICTIONS
REFERENCES
TIMELINE OF DRUG LAW v. SCIENCE