LIVER DISEASE
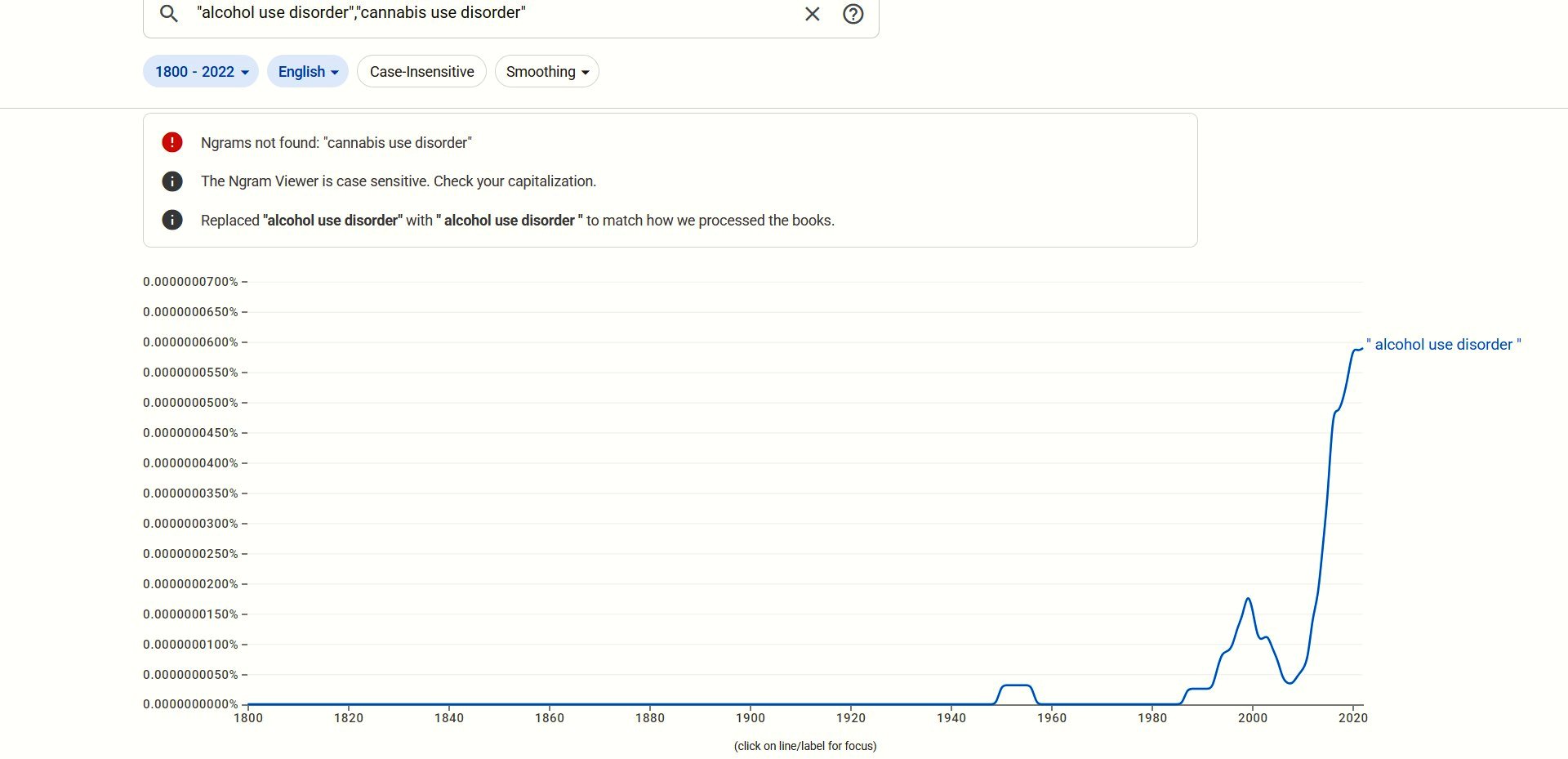
Following the runaway success of "alcohol use disorder"
attempts to set up a rival disorder - "cannabis use
disorder" - met with little success:
Sticking to the script, Fakhoury et al (2025) found that alcoholics
are less likely to die from alcoholic liver disease (ALD) by abusing
cannabis:
"Using the TriNetX US Collaborative Network, we identified adult
patients with AUD between 2010 and 2022. Three cohorts were
constructed: cannabis use disorder (CUD), cannabis users without
cannabis abuse or dependence (CU) and non-cannabis users (non-CU).
Outcomes included ALD, hepatic decompensation and composite all-cause
mortality over 3 years. Incidence and hazard ratios were calculated
using Kaplan-Meier analysis and Cox regression.
"Results: After matching, 33 114 patients were included in each
of the CUD and non-CU groups. Compared to non-CU, CUD was associated
with a lower risk of ALD (HR 0.60, 95% CI 0.53-0.67; p < 0.001),
hepatic decompensation (HR 0.83, 95% CI 0.73-0.95; p =0.005) and
all-cause mortality (HR 0.86, 95% CI 0.80-0.94; p < 0.001) among
individuals with AUD. Although CU was associated with lower risks of
ALD, its risks of hepatic decompensation and all-cause mortality were
similar to those of the non-CU cohort with AUD."
Notice how in these unpleasant results "similar" means the
same as 40%, 17%, and 14% lower risks.
https://pubmed.ncbi.nlm.nih.gov/41117396/
[5505]
Not all liver disease is exclusively alcohol-related.
"Increased incidence of obesity and excess weight lead to an
increased incidence of non-alcoholic fatty liver disease. FLI [Fatty
Liver Index] scores than non-users (F = 13.874;
p < .001). Moreover, cannabis users less frequently met
the criteria for liver steatosis than non-users
(X2 = 7.97, p = .019). Longitudinally,
patients maintaining cannabis consumption after 3 years
presented the smallest increment in FLI over time, which was
significantly smaller than the increment in FLI presented by
discontinuers (p = .022) and never-users
(p = .016). No differences were seen in fibrosis scores
associated with cannabis."
https://www.sciencedirect.com/science/article/abs/pii/S0278584619301393
[541]
Castro and Abdel Bermdez-del Sol (2025) present an alternative name
for NAFLD:
"Potential associations have been investigated between metabolic
dysfunction-associated steatotic liver disease (MASLD), formerly known
as non-alcoholic fatty liver disease, and cannabis use. This study
aimed to determine the association between cannabis use frequency and
MASLD. Up to January 2025, the evidence from PubMed, Scopus, and Web
of Science was synthesized in this systematic review and
meta-analysis, which was registered in PROSPERO (CRD42025025065) and
followed the Preferred Reporting Items for Systematic reviews and
Meta-Analyses (PRISMA) guidelines. Of the 711 initial records, 11
observational studies involving 5,968,702 individuals met the
inclusion criteria. A pooled analysis revealed that cannabis use was
associated with a reduced risk of hepatic steatosis (OR = 0.58; 95%
CI: 0.42-0.81; p = 0.002; I = 97%). The subgroup analysis revealed a
protective association for past users (OR = 0.84; 95% CI: 0.77-0.93)
and occasional users (OR = 0.35; 95% CI: 0.20-0.64), with no
significant association observed for frequent users. The study
revealed that cannabis users exhibited a decline in both the fatty
liver index (mean difference (MD) = -11.02) and the BMI (MD = -1.89
kg/m). However, the findings did not show any statistically
significant changes in liver fat (%), transaminases (aspartate
aminotransferase and alanine aminotransferase), and triglycerides. A
risk-of-bias assessment identified notable methodological limitations.
Overall, the findings suggest a strong association between cannabis
use and MASLD, though causality cannot be established."
https://www.researchgate.net/profile/Nestor-Quinapanta-Castro/publication/395836766_A_Systematic_Review_and_Meta-Analysis_of_Cannabis_Use_Frequency_and_Metabolic_Dysfunction-Associated_Steatotic_Liver_Disease_Scapegoat_or_Healer/links/68d5556cf3032e2b4be32fd8/A-Systematic-Review-and-Meta-Analysis-of-Cannabis-Use-Frequency-and-Metabolic-Dysfunction-Associated-Steatotic-Liver-Disease-Scapegoat-or-Healer.pdf?_tp=eyJjb250ZXh0Ijp7ImZpcnN0UGFnZSI6InB1YmxpY2F0aW9uIiwicGFnZSI6InB1YmxpY2F0aW9uIn19
[5537]
According to the BMJ:
"Nonalcoholic hepatic steatosis, or nonalcoholic fatty liver
disease (NAFLD), is one of the most common causes of chronic liver
disease in the developed world.
"It is a spectrum of disease, ranging from hepatic fat
accumulation without inflammation to steatohepatitis, fibrosis,
cirrhosis, and end-stage liver disease.
"NAFLD is considered the hepatic manifestation of metabolic
syndrome and is associated with obesity, dyslipidemia, and type 2
diabetes mellitus.
"The diagnosis of nonalcoholic fatty liver disease is based on
exclusion of other etiologies of hepatic steatosis, such as alcohol
use, and supportive laboratory tests and imaging. Liver biopsy and
histology is the gold standard for diagnosis, and is performed for
patients at higher risk of fibrosis or steatohepatitis."
and
"Hepatic steatosis occurs when intrahepatic fat is ≥5% of
liver weight.
"Nonalcoholic fatty liver disease (NAFLD) is evidence of hepatic
steatosis (imaging or histologic) in the absence of secondary causes
of hepatic fat accumulation, such as significant alcohol
consumption.
"NAFLD can be categorized as nonalcoholic fatty liver (NAFL) or
nonalcoholic steatohepatitis (NASH), depending on histologic features.
NAFL is the presence of hepatic steatosis without evidence of
hepatocellular injury in the form of hepatocyte ballooning. NASH is
the presence of hepatic steatosis and inflammation with hepatocyte
injury (e.g., ballooning), with or without fibrosis. This distinction
is important for prognosis because NASH may progress to cirrhosis and
liver failure. The risk of NAFL progressing to cirrhosis or liver
failure is minimal.
"To more accurately reflect the pathogenesis of fatty liver, a
new nomenclature of metabolic associated fatty liver disease (MAFLD)
has been suggested."
https://bestpractice.bmj.com/topics/en-us/796
[1968]
After five years of ZPPPD-inspired liver damage, the benefits of
cannabis could be inferred from studies of endocannabinoid action. In
a groundbreaking step, Osei-Hyiaman et al first demonstrated
that CB1R deficiency in mice conveys a protective effect
against diet-induced hepatic steatosis, independent of caloric intake,
in "Endocannabinoid activation at hepatic CB1 receptors
stimulates fatty acid synthesis and contributes to diet-induced
obesity" (2005):
"Endogenous cannabinoids acting at CB(1) receptors stimulate
appetite, and CB(1) antagonists show promise in the treatment of
obesity. CB(1) (-/-) mice are resistant to diet-induced obesity even
though their caloric intake is similar to that of wild-type mice,
suggesting that endocannabinoids also regulate fat metabolism. Here,
we investigated the possible role of endocannabinoids in the
regulation of hepatic lipogenesis. Activation of CB(1) in mice
increases the hepatic gene expression of the lipogenic transcription
factor SREBP-1c and its targets acetyl-CoA carboxylase-1 and fatty
acid synthase (FAS). Treatment with a CB(1) agonist also increases de
novo fatty acid synthesis in the liver or in isolated hepatocytes,
which express CB(1). High-fat diet increases hepatic levels of the
endocannabinoid anandamide (arachidonoyl ethanolamide), CB(1) density,
and basal rates of fatty acid synthesis, and the latter is reduced by
CB(1) blockade. In the hypothalamus, where FAS inhibitors elicit
anorexia, SREBP-1c and FAS expression are similarly affected by CB(1)
ligands. We conclude that anandamide acting at hepatic CB(1)
contributes to diet-induced obesity and that the FAS pathway may be a
common molecular target for central appetitive and peripheral
metabolic regulation."
http://www.jci.org/articles/view/23057/files/pdf
[3962]
Even without alcoholism, liver disease will knock nearly three years
off your life:
"In this nationwide population-based cohort, all patients with
NAFLD diagnosis and without baseline CVD (ascertaining from the
Swedish National Patient Register from 1987 to 2016, n = 10,023) were
matched 10:1 on age, sex, and municipality to individuals from the
general population (controls, n = 96,313). CVD diagnosis and mortality
were derived from national registers. Multistate models and flexible
parametric survival models were used to estimate adjusted hazard
ratios (aHRs) for CVD risk and loss in life expectancy due to NAFLD.
We identified 1037 (10.3%) CVD events in patients with NAFLD and 4041
(4.2%) in controls. CVD risk was 2.6-fold higher in NAFLD compared
with controls (aHR = 2.61, 95% CI = 2.362.88) and was strongest for
nonfatal CVD (aHR = 3.71, 95% CI = 3.294.17). After a nonfatal CVD
event, the risk for all-cause mortality was similar between patients
with NAFLD and controls (aHR = 0.89, 95% CI = 0.641.25). Life
expectancy in patients with NAFLD was, on average, 2.8 years lower
than controls, with the highest loss of life-years when NAFLD was
diagnosed in middle age (4060 years).
"Conclusions
NAFLD was associated with a higher risk of nonfatal CVD but did not
affect post-CVD mortality risk. Patients diagnosed with NAFLD have a
lower life expectancy than the general population."
As for cardiovascular events in those with a liver diagnosis:
"Patients with NAFLD and cirrhosis at baseline had higher rates
of all CVD events in the first model (HR 7.92, 95% CI = 4.7113.3),
although this estimate was lower after adjustments for CVD risk
factors (aHR 2.56, 95% CI = 1.315.01)."
and
"Several observations can be made from this large nationwide
cohort study set in a secondary or tertiary setting. First, we found
an elevated risk of nonfatal CVD events in patients with NAFLD
compared with matched controls. Second, patients with cirrhosis had a
higher CVD risk than controls, but not compared to patients with
noncirrhotic NAFLD. Third, while NAFLD was associated with increased
overall mortality, no increased mortality was observed in patients
with NAFLD with incident CVD compared to matched controls who had also
experienced a nonfatal CVD event. Finally, the overall loss of life
expectancy in patients with NAFLD was about 3 years, which was
affected by age and clinical setting at diagnosis. LEL [loss of
expectancy in life] was highest in hospitalized patients and when the
diagnosis of NAFLD was made at middle age, whereas no apparent loss in
life expectancy was observed for those aged ≥80."
https://aasldpubs.onlinelibrary.wiley.com/doi/10.1002/hep.32519
[1967]
In 2017's "Cannabis use is associated with reduced prevalence of
non-alcoholic fatty liver disease: A cross-sectional study",
Adejumo et al... "...conducted a population-based case-control
study of 5,950,391 patients using the 2014 Healthcare Cost and
Utilization Project (HCUP), Nationwide Inpatient Survey (NIS)
discharge records of patients 18 years and older. After identifying
patients with NAFLD (1% of all patients), we next identified three
exposure groups: non-cannabis users (98.04%), non-dependent cannabis
users (1.74%), and dependent cannabis users (0.22%). We adjusted for
potential demographics and patient related confounders and used
multivariate logistic regression (SAS 9.4) to determine the odds of
developing NAFLD with respects to cannabis use. Our findings revealed
that cannabis users (dependent and nondependent) showed significantly
lower NAFLD prevalence compared to non-users (AOR: 0.82[0.760.88];
p<0.0001). The prevalence of NAFLD was 15% lower in non-dependent
users (AOR: 0.85[0.790.92]; p<0.0001) and 52% lower in dependent
users (AOR: 0.49 [0.360.65]; p<0.0001). Among cannabis users,
dependent patients had 43% significantly lower prevalence of NAFLD
compared to non-dependent patients (AOR: 0.57[0.420.77]; p<0.0001).
Our observations suggest that cannabis use is associated with lower
prevalence of NAFLD in patients. These novel findings suggest
additional molecular mechanistic studies to explore the potential role
of cannabis use in NAFLD development."
https://journals.plos.org/plosone/article/file?id=10.1371/journal.pone.0176416&type=printable
[2772]
In 2020 Collaborators of the ANRS CO13 HEPAVIH Study Group
report:
"Mortality among individuals co-infected with HIV and hepatitis
C virus (HCV) is relatively high. We evaluated the association between
psychoactive substance use and both HCV and non-HCV mortality in
HIV/HCV co-infected patients in France, using Fine and Gray's
competing-risk model adjusted for socio-demographic, clinical
predictors and confounding factors, while accounting for competing
causes of death. Over a 5-year median follow-up period, 77 deaths
occurred among 1028 patients. Regular/daily cannabis use, elevated
coffee intake, and not currently smoking were independently associated
with reduced HCV-mortality (adjusted sub-hazard ratio [95% CI] 0.28
[0.10-0.83], 0.38 [0.15-0.95], and 0.28 [0.10-0.79], respectively).
Obesity and severe thinness were associated with increased
HCV-mortality (2.44 [1.00-5.93] and 7.25 [2.22-23.6] versus normal
weight, respectively). Regular binge drinking was associated with
increased non-HCV-mortality (2.19 [1.10-4.37]). Further research is
needed to understand the causal mechanisms involved. People living
with HIV/HCV co-infection should be referred for tobacco, alcohol and
weight control interventions and potential benefits of cannabis-based
therapies investigated."
https://pubmed.ncbi.nlm.nih.gov/31286317/
[3385]
From the perspective of organ damage from alcohol, Yan et al set out
to settle the vexed question of whether it is a good idea to add
cannabis to alcohol. Reporting in the Journal of Biochemical and
Molecular Toxicology:
"Cannabinoids (CBs) are psychoactive compounds, with reported
anticancer, anti-inflammatory, and anti-neoplastic properties. The
study was aimed at assessing the hepatoprotective effects of CB
against ethanol (EtOH)-induced liver toxicity in rats. The animals
were divided into seven groups: control (Group I) and Group II were
treated with 50% ethanol (EtOH 5 mg/kg). Groups III, IV, and VI
were treated with (EtOH + CB 10 mg/kg), (EtOH + CB
20 mg/kg), and (EtOH + CB 30 mg/kg), respectively. Groups
V and VII consisted of animals treated with 20 and 30 mg/kg, of
CB, respectively. Biochemical analysis revealed that Group IV (EtOH +
CB 20 mg/kg) had reduced levels of ALTalanine transferase,
ASTaspartate aminotransferase, ALPalanine peroxidase,
MDAmalondialdehyde and increased levels of GSH-reduced glutathione.
Histopathological analysis of liver and kidney tissues showed that
EtOH + CB (20 and 30 mg/kg) treated animal groups exhibited
normal tissue architecture similar to that of the control group. ELISA
[enzyme-linked immunosorbent assay] revealed that the inflammatory
markers were reduced in the animal groups that were treated with EtOH
+ CB 20 mg/kg, in comparison to the animals treated only with
EtOH. The mRNA expression levels of COX-2, CD-14, and MIP-2 showed a
remarkable decrease in EtOH + CB treated animal groups to control
groups. Western blot analysis revealed that CB downregulated
p38/JNK/ERK thereby exhibiting its hepatoprotective property by
inhibiting mitogen-activated protein kinase pathways. Thus, our
findings suggest that CB is a potential candidate for the treatment of
alcohol-induced hepatotoxicity.
https://onlinelibrary.wiley.com/doi/abs/10.1002/jbt.23260
[1859]
El Moneim Hussein et al of Alexandria University in Egypt used a
different experimental model of liver damage in "Protective and
therapeutic effects of cannabis plant extract on liver cancer induced
by dimethylnitrosamine in mice" (2019), finding that the Group
III mice, who received a cannabis extract with a ratio of ~2:1 THC:CBD
pre-treatment in advance of the DMNA did better than those who
received cannabis with or after the treatment, concluding:
"...exposure to DMNA plays a role in pathogenesis of liver
disease leading to carcinogenicity and causes disturbances in the
activities of mice liver enzymes while cannabis causes a partial
improvement in these enzymes. The protective effect of cannabis
extract is more pronounced than other groups and this is demonstrated
in group III. Cannabinoids might exert their anti-tumor effects by
direct induction of apoptosis and can decrease telomerase activity by
inhibiting the expression of hTERT [telomerase reverse transcriptase]
gene. Coordination between inhibition of telomerase activity and
induction of apoptosis might be a potential therapeutic agent for
cancer treatment."
https://www.tandfonline.com/doi/full/10.1016/j.ajme.2014.02.003
[4073]
Glutathione exists in reduced (GSH) and oxidized (GSSG) states. The
ratio of reduced glutathione to oxidized glutathione within cells is a
measure of cellular oxidative stress where increased GSSG-to-GSH ratio
is indicative of greater oxidative stress. In healthy cells and
tissue, more than 90% of the total glutathione pool is in the reduced
form (GSH), with the remainder in the disulfide form (GSSG).
In the reduced state, the thiol group of cysteinyl residue is a
source of one reducing equivalent. Glutathione disulfide (GSSG) is
thereby generated. The oxidized state is converted to the reduced
state by NADPH. This conversion is catalyzed by glutathione
reductase:
NADPH + GSSG + H2O → 2 GSH + NADP+ + OH−
https://en.wikipedia.org/wiki/Glutathione
[1922]
In 2011 Vara et al reported the "Anti-tumoral action of
cannabinoids on hepatocellular carcinoma: role of AMPK-dependent
activation of autophagy":
"Hepatocellular carcinoma (HCC) is the third cause of
cancer-related death worldwide. When these tumors are in advanced
stages, few therapeutic options are available. Therefore, it is
essential to search for new treatments to fight this disease. In this
study, we investigated the effects of cannabinoids--a novel family of
potential anticancer agents--on the growth of HCC. We found that
Δ(9)-tetrahydrocannabinol (Δ(9)-THC, the main active
component of Cannabis sativa) and JWH-015 (a cannabinoid receptor 2
(CB(2)) cannabinoid receptor-selective agonist) reduced the viability
of the human HCC cell lines HepG2 (human hepatocellular liver
carcinoma cell line) and HuH-7 (hepatocellular carcinoma cells), an
effect that relied on the stimulation of CB(2) receptor. We also found
that Δ(9)-THC- and JWH-015-induced autophagy relies on tribbles
homolog 3 (TRB3) upregulation, and subsequent inhibition of the
serine-threonine kinase Akt/mammalian target of rapamycin C1 axis and
adenosine monophosphate-activated kinase (AMPK) stimulation.
Pharmacological and genetic inhibition of AMPK upstream kinases
supported that calmodulin-activated kinase kinase β was
responsible for cannabinoid-induced AMPK activation and autophagy. In
vivo studies revealed that Δ(9)-THC and JWH-015 reduced the
growth of HCC subcutaneous xenografts, an effect that was not evident
when autophagy was genetically of pharmacologically inhibited in those
tumors. Moreover, cannabinoids were also able to inhibit tumor growth
and ascites in an orthotopic model of HCC xenograft. Our findings may
contribute to the design of new therapeutic strategies for the
management of HCC."
https://www.nature.com/articles/cdd201132.pdf
[3691]
Adejumo et al have performed several studies on the incidence of
hepatic disorders and cannabis:
In 2018's "Cannabis use is associated with reduced prevalence of
progressive stages of alcoholic liver disease" the aim was
to
"...determine the effects of cannabis use on the incidence of
liver disease in individuals who abuse alcohol.
"Methods: We analysed the 2014 Healthcare Cost and Utilization
Project-Nationwide Inpatient Sample (NIS) discharge records of
patients 18 years and older, who had a past or current history of
abusive alcohol use (n = 319 514). Using the International
Classification of Disease, Ninth Edition codes, we studied the four
distinct phases of progressive ALD with respect to three cannabis
exposure groups: non-cannabis users (90.39%), non-dependent cannabis
users (8.26%) and dependent cannabis users (1.36%). We accounted for
the complex survey sampling methodology and estimated the adjusted
odds ratio (AOR) for developing AS, AH, AC and HCC with respect to
cannabis use (SAS 9.4).
"Results: Our study revealed that among alcohol users,
individuals who additionally use cannabis (dependent and non-dependent
cannabis use) showed significantly lower odds of developing AS, AH, AC
and HCC [alcoholic steatosis, steatohepatitis, fibrosis-cirrhosis,
hepatocellular carcinoma] (AOR: 0.55 [0.48-0.64], 0.57 [0.53-0.61],
0.45 [0.43-0.48] and 0.62 [0.51-0.76]). Furthermore, dependent users
had significantly lower odds than non-dependent users for developing
liver disease.
"Conclusions: Our findings suggest that cannabis use is
associated with a reduced incidence of liver disease in
alcoholics."
https://pubmed.ncbi.nlm.nih.gov/29341392/
[2771]
In another 2018 paper Adejumo et al, starting with 188,333 records,
also looked at the effect of cannabis use on chronic liver disease
(CLD) from Hepatitis C Virus (HCV) infection, the most common cause of
CLD, and...
"...revealed that cannabis users (CUs) had decreased prevalence
of liver cirrhosis (aPRR: 0.81[0.72-0.91]), unfavorable discharge
disposition (0.87[0.78-0.96]), and lower total health care cost
($39,642[36,220-43,387] versus $45,566[$42,244-$49,150]), compared to
noncannabis users (NCUs). However, there was no difference among CUs
and NCUs on the incidence of liver carcinoma (0.79[0.55-1.13]),
in-hospital mortality (0.84[0.60-1.17]), and LOS [length of stay]
(5.58[5.10-6.09] versus 5.66[5.25-6.01]). Among CUs, dependent
cannabis use was associated with lower prevalence of liver cirrhosis,
compared to nondependent use (0.62[0.41-0.93])."
https://downloads.hindawi.com/journals/cjgh/2018/9430953.pdf
[2773]
In 2019 Adejumo was back again with "Reduced Risk of
Alcohol-Induced Pancreatitis With Cannabis Use"...
"We analyzed data from 2012 to 2014 of the Healthcare Cost and
Utilization Project-Nationwide Inpatient Sample discharge records of
patients 18 years and older. We used the International Classification
of Disease, Ninth Edition codes, to identify 3 populations: those with
gallstones (379,125); abusive alcohol drinkers (762,356); and
non-alcohol-non-gallstones users (15,255,464). Each study population
was matched for cannabis use record by age, race, and gender, to
records without cannabis use. The estimation of the adjusted odds
ratio (aOR) of having acute and chronic pancreatitis (AP and CP) made
use of conditional logistic models.
and
"Concomitant cannabis and abusive alcohol use were associated
with reduced incidence of AP and CP (aOR: 0.50 [0.48 to 0.53] and 0.77
[0.71 to 0.84]). Strikingly, for individuals with gallstones,
additional cannabis use did not impact the incidence of AP or CP
[acute and chronic pancreatitis]. Among
non‐alcohol‐non‐gallstones users, cannabis use was
associated with increased incidence of CP, but not AP (1.28 [1.14 to
1.44] and 0.93 [0.86 to 1.01]).
"Conclusions Our findings suggest a reduced incidence of only
alcohol-associated pancreatitis with cannabis use."
https://taliabardash.commons.gc.cuny.edu/files/2022/01/PAncreatitis-article.pdf
[2776]
Spaccavento et al (2025) present "Medical cannabis for the
management of pain in chronic pancreatitis with recurrent
exacerbations: a case report". It worked.
https://jcannabisresearch.biomedcentral.com/articles/10.1186/s42238-025-00303-w
[5266]
In "Δ9-Tetrahydrocannabinol induces endocannabinoid
accumulation in mouse hepatocytes: antagonism by Fabp1 gene
ablation" McIntosh et al (2018) considered how
"Phytocannabinoids, such as Δ9-tetrahydrocannabinol (THC),
bind and activate cannabinoid (CB) receptors, thereby piggy-backing on
the same pathway's endogenous endocannabinoids (ECs). The recent
discovery that liver fatty acid binding protein-1 (FABP1) is the major
cytosolic chaperone protein with high affinity for both Δ9-THC
and ECs suggests that Δ9-THC may alter hepatic EC
levels."
They went on to show:
"First, the phytocannabinoid CB1 agonist, Δ9-THC,
significantly increased AEA and 2-AG levels in WT hepatocytes.
Consistent with this finding, phytocannabinoids (i.e., Δ9-THC,
cannabidiol) increase levels of AEA and 2-AG in the blood and brains
of humans and rodents. Because CB1 has a similar affinity for AEA as
for Δ9-THC, this suggests that Δ9-THC may, at least in part,
exert its activating effect on CB1 by increasing the hepatocytes'
endogenous level of AEA. Δ9-THC even more dramatically increased
the WT hepatocyte level of 2-AG by 2-fold more than AEA. Despite CB1's
weaker affinity for 2-AG than for either AEA or Δ9-THC, 2-AG is
about 3-fold more potent than AEA at CB1. While the 2-AG-induced
increase in WT hepatocyte level of 2-AG may be attributable, at least
in part, to increased 2-AG available for uptake, 2-AG had no effect on
the non-ARA-containing 2-MGs, i.e., 2-OG and 2-PG, in WT hepatocytes.
Taken together, these novel observations showed that exogenously added
Δ9-THC, as well as 2-AG, increased the WT hepatocyte level of AEA
and, even more so, 2-AG. Although the hepatocytes were incubated with
about 20-fold higher concentration levels than typically observed in
mouse serum after either intravenous injection of 3 mg/kg or
inhalation of 20 mg of Δ9-THC, uptake did not appear saturated
with respect to concentration.
"Second, loss of FABP1 (i.e., Fabp1 gene ablation) alone
increased AEA and 2-AG levels in cultured primary mouse hepatocytes by
more than 2-fold. This finding is physiologically significant because
LKO also significantly increased AEA and 2-AG in mouse liver, albeit
to a smaller extent, near 30%. In addition, LKO concomitantly
increased WT hepatocyte levels of EPEA and 2-OG by >2- and 4-fold,
respectively. A similar effect, albeit also of smaller magnitude, was
also observed in livers of LKO mice. The significance of LKO's impact
on the non-ARA-containing NAE (i.e., EPEA) and 2-MG (i.e., 2-OG) lies
in their ability to indirectly alter the effectiveness of CB1
agonists. While non-ARA-containing NAEs (OEA, PEA) and 2-MGs (2-OG,
2-PG) do not directly bind/activate CB receptors, they represent
entourage molecules that may enhance the effects of AEA by competing
with either the transporters or the enzymes mediating the inactivation
of ECs or by enhancing binding/action of ECs, such as AEA. In
contrast, the EPA-derived EPEA displaces AEA and 2-AG from cell
membranes to reduce AEA and 2-AG release by synthetic enzymes. In
fact, EPA supplementation in humans and animals decreases 2-AG and AEA
in brain and plasma. Because LKO elicits a several-fold larger
increase in hepatocyte 2-OG than EPEA, this would suggest potential
net potentiation of CB1 agonists.
"Third, LKO blocked/diminished the ability of Δ9-THC to
increase both AEA and 2-AG, but, in contrast, potentiated the ability
of 2-AG to increase the hepatocyte level of AEA and 2-AG. The reasons
for the opposite effects of LKO on the ability of Δ9-THC and 2-AG
to impact hepatocyte AEA and 2-AG are not completely clear. One
possibility is based on differences in CB1's and FABP1's affinities
for these ligands. For example, CB1 binds Δ9-THC with nearly
10-fold higher affinity than for 2-AG. On the other hand FABP1 binds
2-AG with 10-fold higher affinity than for Δ9-THC. An alternate
possibility may relate to a mechanistic difference in uptake of
Δ9-THC and 2-AG. Nearly 90% of oral CB undergoes first-pass
removal by the liver by an as yet poorly understood mechanism.
Although the mechanism of EC (AEA, 2-AG) uptake across the plasma
membrane is also not completely clear, AEA uptake appears to be driven
by intracellular degradative enzymes. Much less is known about 2-AG
uptake, except that it is saturable and blocking 2-AG hydrolysis does
not alter the rate of 2-AG uptake."
https://www.jlr.org/article/S0022-2275(20)33916-X/fulltext
[5605]
This increased anandamide is the same anandamide pronounced by other
researchers to be lacking in psychosis, e.g. Morgan et al's
"first study to examine CSF eicosanoid levels in cannabis
users" - in 2013 - in which 33 subjects subjected themselves to a
lumbar puncture for fifty quid.
https://www.cambridge.org/core/services/aop-cambridge-core/content/view/6C4E16919C53C3444C90AA53C76DC85D/S0007125000274485a.pdf/div-class-title-cerebrospinal-fluid-anandamide-levels-cannabis-use-andpsychotic-like-symptoms-div.pdf
[5606]
Alcohol reduces circulating anandamide and AEA levels are repressed in
AUD. In a 2023 study by Sloan et al:
Several lines of evidence suggest that endocannabinoid signaling may
influence alcohol consumption. Preclinical studies have found that
pharmacological blockade of cannabinoid receptor 1 leads to reductions
in alcohol intake. Furthermore, variations in endocannabinoid
metabolism between individuals may be associated with the presence and
severity of alcohol use disorder. However, little is known about the
acute effects of alcohol on the endocannabinoid system in humans. In
this study, we evaluated the effect of acute alcohol administration on
circulating endocannabinoid levels by analyzing data from two
highly-controlled alcohol administration experiments. In the first
within-subjects experiment, 47 healthy participants were randomized to
receive alcohol and placebo in a counterbalanced order. Alcohol was
administered using an intravenous clamping procedure such that each
participant attained a nearly identical breath alcohol concentration
of 0.05%, maintained over 3 hours. In the second experiment, 23
healthy participants self-administered alcohol intravenously;
participants had control over their exposure throughout the paradigm.
In both experiments, circulating concentrations of two
endocannabinoids, N-arachidonoylethanolamine (AEA) and
2-arachidonoylglycerol (2-AG), were measured at baseline and following
alcohol exposure. During the intravenous clamping procedure, acute
alcohol administration reduced circulating AEA but not 2-AG levels
when compared to placebo. This finding was confirmed in the
self-administration paradigm, where alcohol reduced AEA levels in an
exposure-dependent manner. Future studies should seek to determine
whether alcohol administration has similar effects on brain
endocannabinoid signaling. An improved understanding of the
bidirectional relationship between endocannabinoid signaling and
alcohol intake may deepen our understanding of the etiology and
repercussions of alcohol use disorder.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9413364/
[5608]
The Defence believes the depressed AEA levels of chronic alcoholism
shoot back up in long-term alcohol withdrawal but may never return to
baseline. According to a review by Serrano and Natividad (2022)
"...the effects produced by chronic cannabis use returned to
normal function after a protracted abstinence period, whereas the
disruptions in patients with AUD persisted after 4 weeks of withdrawal
from alcohol use. These findings suggest that CB1 receptor
downregulation is a common neuroadaptation to chronic substance use,
although seemingly more extensive under alcohol exposure than with
substances that directly interact with CB1 receptors. This may suggest
that alcohol has potent effects on the mechanisms of CB1 receptor
expression and function (e.g., signaling transduction, epigenetic
changes). Alcohol is also a notable activator of neuroinflammation,
which over the course of repeated use may temper the anti-inflammatory
responses of exogenous/endogenous cannabinoid signaling. Moreover, it
is possible that alcohol may play a role in altering endogenous
mediators of cannabinoid signaling (e.g., eCBs), from which lapses in
the recovery of these signaling ligands influence the long-lasting
deficits in CB1 receptor signaling."
Table 1 summarises selected research on alcohol and AEA and 2-AG up
to then.
"Findings from the Parsons laboratory demonstrated that acute
alcohol self-administration elicits increases in eCB release that are
tempered over repeated exposure; however, readers are referred to the
Alcohol-Induced Alterations in Brain eCB Levels section of this review
for noteworthy distinctions. In addition, the method of alcohol
exposure plays a marked role in the subsequent analysis of
abstinence-related effects. That stated, chronic alcohol exposure is
generally associated with the disruption of eCB clearance mechanisms,
impaired eCB mediated forms of synaptic plasticity, and the
downregulation of cannabinoid receptor function. The dysregulation of
eCB signaling may be relevant given that eCBs play a prominent role in
the maintenance of affective states and the constraint of stress
responses, both of which serve as provocateurs of continued use and
relapse."
https://www.researchgate.net/journal/International-Journal-of-Molecular-Sciences-IJMS-1422-0067/publication/367536935_Cannabinoids_in_the_Modulation_of_Oxidative_Signaling/links/68043d63ded43315572db3c1/Cannabinoids-in-the-Modulation-of-Oxidative-Signaling.pdf?_tp=eyJjb250ZXh0Ijp7ImZpcnN0UGFnZSI6InB1YmxpY2F0aW9uIiwicGFnZSI6InB1YmxpY2F0aW9uIn19
[5607]
In the opinion of Dibba et al (2018) both CB1 and CB2 receptors have
roles in anticirrhotic mechanisms:
"Endocannabinoids, themselves also have mechanistic roles in
cirrhosis. Arachidonoyl ethanolamide (AEA) exhibits antifibrogenic
properties by inhibition of HSC proliferation and induction of
necrotic death. AEA induces mesenteric vasodilation and hypotension
via CB1 induction. 2-arachidonoyl glycerol (2-AG) is a fibrogenic
mediator independent of CB receptors, but in higher doses induces
apoptosis of HSCs, which may actually show antifibrotic properties.
2-AG has also demonstrated growth-inhibitory and cytotoxic effects.
The exocannabinoid, THC, suppresses proliferation of hepatic
myofibroblasts and stellate cells and induces apoptosis, which may
reveal antifibrotic and hepatoprotective mechanisms. Thus, several
components of the endocannabinoid system have therapeutic potential in
cirrhosis."
We learn:
"Those with clinically significant disease are at risk of
complications including ascites, encephalopathy, varices, variceal
hemorrhage, postsurgical decompensation and hepatocellular carcinoma.
Serum albumin, presence of gastroesophageal varices, and Model for
End-Stage Liver Disease [MELD] are predictors of decompensation in
these patients. Decompensated cirrhosis refers to those who possess
one of these complications in the setting of cirrhosis."
And in our fundamental appraisal of the dangers of NECUD in
cirrhosis:
"Median survival rate for compensated cirrhotic patients ranges
between 9 and 12 years. Decompensated cirrhotic patients have poor
survival with a 1-year survival rate less than 50% in patients with
ascites and variceal hemorrhage."
https://www.mdpi.com/2305-6320/5/2/52
[4963]
In a 2021 paper by Sobotka et al "Cannabis use may reduce
healthcare utilization and improve hospital outcomes in patients with
cirrhosis"
"Cannabis use was detected in 370 (2.1%) of 17,520 cirrhotics
admitted in 2011 and in 1162 (5.3%) of 21,917 cirrhotics in 2015
(p-value <0.001). On multivariable analysis, cirrhotics utilizing
cannabis after its legalization experienced a decreased rate of
admissions related to hepatorenal syndrome (Odds Ratio (OR): 0.51; 95%
Confidence Interval (CI): 0.34−0.78) and ascites (OR: 0.73; 95%
CI: 0.63−0.84). Cirrhotics with an etiology of disease other
than alcohol and hepatitis C had a higher risk of admission for
hepatic encephalopathy if they utilized cannabis [OR: 1.57; 95% CI:
1.162.13]. Decreased length of stay (-1.15 days; 95% CI: -1.62,
-0.68), total charges (-$15,852; 95% CI: -$21,009, -$10,694), and
inpatient mortality (OR: 0.68; 95% CI: 0.51−0.91) were also
observed in cirrhotics utilizing cannabis after legalization compared
to cirrhotics not utilizing cannabis or utilizing cannabis prior to
legalization."
https://www.sciencedirect.com/science/article/pii/S1665268120302052?via%3Dihub
[3886]
By 2023 we had "Marijuana use is inversely associated with liver
steatosis detected by transient elastography in the general United
States population in NHANES 2017-2018: A cross-sectional study"
and according to Du et al at the General Hospital of Central Theater
Command, Wuchangqu, Wuhan:
"A total of 2622 participants were included in this study. The
proportions of never marijuana users, past users, and current users
were 45.9%, 35.0%, and 19.1%, respectively. Compared to never
marijuana users, past and current users had a lower prevalence of
liver steatosis (P = 0.184 and P = 0.048, respectively). In the
alcohol intake-adjusted model, current marijuana use was an
independent predictor of a low prevalence of liver steatosis in people
with non-heavy alcohol intake. The association between marijuana use
and liver fibrosis was not significant in univariate and multivariate
regression.
"Conclusion: In this nationally representative sample, current
marijuana use is inversely associated with steatosis. The
pathophysiology is unclear and needs further study. No significant
association was established between marijuana use and liver fibrosis,
irrespective of past or current use."
https://journals.plos.org/plosone/article/file?id=10.1371/journal.pone.0284859&type=printable
[2775]
Paladiya et al (2024) used the National Inpatient Sample (NIS)
20162020:
"Of the 3,379,484 patients, CU was identified in 52,315 (1.54%)
patients. The majority of the CU patients were aged 18-44 years
(46.4%), male (59.7%) and White race (59.75). Table shows the
prevalence of CU among various comorbidities. Patients with CU had a
lower prevalence of cirrhosis (21.8% vs 36.8%, P< 0.001),
decompensated cirrhosis (DC) (11.9% vs 21.2%, P< 0.001),
hepatocellular cancer (HCC) (0.8% vs 1.7%, P< 0.001), chronic
kidney disease (CKD) (13% vs 24.3%, P< 0.001), heart failure (HF)
(14.7% vs 22.5%,P< 0.001), and in-hospital mortality (IHM) (2.2% vs
4.5%, P< 0.001). (Figure 1) After adjusting for confounding
factors, patients with CU had lower odds of IHM (aOR- 0.70, 95%
CI-0.61-0.80, P< 0.001), cirrhosis (aOR- 0.72, 95% CI-0.68-0.76,
P< 0.001), DC (aOR-0.73, 95% CI-0.68-0.78, P< 0.001), CKD
(aOR-0.81, 95% CI-0.76-0.86, P< 0.001) and HCC (aOR-0.71, 95% CI
0.57-0.89, P=0.003), however had higher odds of myocardial infarction
(MI) (aOR-1.42, 95% CI-1.27-1.83, P< 0.001) and stroke (aOR-1.53,
95% CI-1.27-1.83, P< 0.001)."
https://journals.lww.com/ajg/fulltext/2024/10001/s2046_cannabis_use_in_metabolic.2047.aspx
[5776]
Now what is it that makes people keep going back to the pub?
Conditioned Place Preference (CPP) is one of the most popular models
to study the motivational effects of alcohol in animals. According to
Amaral et al "Susceptibility to extinction and reinstatement of
ethanol-induced conditioned place preference is related to differences
in astrocyte cystine-glutamate antiporter content":
"One important regulator of glutamate homeostasis, maintaining
extrasynaptic glutamatergic tone, is the astrocyte cystine-glutamate
antiporter (xCT). It acts by transporting one glutamate molecule at
the same time as transporting one cystine molecule. This non-vesicular
transport direction is dependent on extra and intracellular
concentrations of the substrates, transporting the substrate both to
the intracellular and the extracellular space. Since the intracellular
concentration of glutamate is much higher than that of cystine in
astrocytes, xCT essentially transports one cystine molecule to the
intracellular space while transporting one glutamate molecule to the
extracellular space (Bridges et al., 2012). It is expressed throughout
the adult mouse brain, including the NAcc, the medial prefrontal
cortex (mPFC) and the amygdala (Amy) (Van Liefferinge et al.,
2016).
"Recent data have shown that chronic drug intake or withdrawal
alter xCT expression in animal models of addiction. Nicotine
self-administration or inhalation through electronic cigarettes
decreases xCT expression in the striatum, ventral tegmental area
(VTA), and hippocampus (Alasmari et al., 2017; Knackstedt et al.,
2009). Withdrawal from chronic ethanol consumption decreases xCT
content in the NAcc, while chronic ethanol consumption has the
opposite effect (Peana et al., 2014). In alcohol-preferring rats,
chronic ethanol consumption decreases xCT in the Amy (Aal-Aaboda et
al., 2015)."
https://www.sciencedirect.com/science/article/abs/pii/S0168010220304028
[976]
...while Ryu et al at the Laboratory of Liver Research, Graduate
School of Medical Science and Engineering, KAIST, Daejeon, Korea, add
that:
"Chronic alcohol drinking results in oxidative stress-mediated
shortage of cysteine and thereby induces the depletion of glutathione
(GSH), which leads to the upregulation of Slc7a11 expression (encoding
xCT in system xc--cystine/glutamate antiporter) to compensate for the
cysteine shortage. Consequently, xCT-mediated glutamate excretion
stimulates metabotropic glutamate receptor 5 (mGluR5) in neighboring
HSCs to produce 2-AG in a diacylglycerol lipase-β-dependent
manner. In addition, this study demonstrated that the inhibition of
the xCT and mGluR5 substantially reversed alcohol-mediated hepatic
steatosis by reducing 2-AG production in HSCs."
and writing in May 2022 they say:
"Recent studies have begun to dissect the interaction of
neurotransmitters such as endocannabinoid, glutamate and
neuroendocrine factors, and hepatic non-parenchymal cells. Signaling
pathways involved in different neurotransmitters indicate their
contributions to ALD pathogenesis."
Regarding the endocannabinoid part of this (while avoiding cannabis
completely) they announce that:
"Recent studies have suggested that endocannabinoids and their
receptors might be involved in the pathogenesis of non-alcoholic fatty
liver disease (NAFLD) and hepatic fibrosis. Extending these findings,
our studies demonstrated the pathogenic effects of endocannabinoid
2-AG and CB1 receptor in alcohol-related hepatic steatosis. In mice,
chronic alcohol consumption induces 2-AG production in HSCs [hepatic
stellate cells], which then stimulates CB1 receptor to upregulate the
expression of SREBP1c [Sterol regulatory element-binding protein 1]
and FAS (CD95) [aka Fas receptor, FasR, apoptosis antigen 1 (APO-1 or
APT), cluster of differentiation 95 (CD95) or tumor necrosis factor
receptor superfamily member 6 (TNFRSF6)*] and inhibit the activation
of AMPK, enhancing fat accumulation in hepatocytes. Conversely,
treatment of rimonabant, a selective antagonist of CB1 receptor, and
genetic inhibition of CB1 receptor ameliorated alcohol-related hepatic
steatosis in mice. A recent study further supported this finding by
delineating the underlying mechanism of 2-AG production in HSCs.
Chronic alcohol drinking results in oxidative stress-mediated shortage
of cysteine and thereby induces the depletion of glutathione (GSH),
which leads to the upregulation of Slc7a11 expression (encoding xCT in
system xc--cystine/glutamate antiporter) to compensate for the
cysteine shortage. Consequently, xCT-mediated glutamate excretion
stimulates metabotropic glutamate receptor 5 (mGluR5) in neighboring
HSCs to produce 2-AG in a diacylglycerol lipase-β-dependent
manner. In addition, this study demonstrated that the inhibition of
the xCT and mGluR5 substantially reversed alcohol-mediated hepatic
steatosis by reducing 2-AG production in HSCs. This study also
emphasized the bidirectional loop pathway where hepatocytes and HSCs
interact with each other by secreting neurotransmitters (e.g.
glutamate and 2-AG) and expressing their receptors (e.g. mGluR5 and
CB1), and proposed a new concept of metabolic synapse between
hepatocytes and HSCs. In contrast to CB1 receptors, CB2 receptors in
KCs are known to have protective effects against ASH. CB2 receptor
activation attenuates alcohol-induced steatohepatitis and the main
mechanism is explained by paracrine interaction of endocannabinoid
between hepatocyte and Kupffer cell. The more precise mechanism has
suggested that the CB2 receptor protects the liver from steatosis by
CB2-mediated autophagy in KCs through a heme-oxygenase-1 dependent
pathway, ameliorating inflammatory responses in ALD. to produce 2-AG
in a diacylglycerol lipase-β-dependent manner."
The study
"...emphasized the bidirectional loop pathway where hepatocytes
and HSCs interact with each other by secreting neurotransmitters (e.g.
glutamate and 2-AG) and expressing their receptors (e.g. mGluR5 and
CB1), and proposed a new concept of metabolic synapse between
hepatocytes and HSCs. In contrast to CB1 receptors, CB2 receptors in
KCs are known to have protective effects against ASH. CB2 receptor
activation attenuates alcohol-induced steatohepatitis and the main
mechanism is explained by paracrine interaction of endocannabinoid
between hepatocyte and Kupffer cell [resident macrophages in the
liver]. The more precise mechanism has suggested that the CB2 receptor
protects the liver from steatosis by CB2-mediated autophagy in KCs
through a heme-oxygenase-1 dependent pathway, ameliorating
inflammatory responses in ALD."
https://www.sciencedirect.com/science/article/pii/S2542568422000599
[1955]
In "Paracrine Activation of Hepatic CB1 Receptors by Stellate
Cell-Derived Endocannabinoids Mediates Alcoholic Fatty Liver"
(2008) Jeong et al
"...report that the steatosis induced in mice by a low-fat,
liquid ethanol diet is attenuated by concurrent blockade of
cannabinoid CB1 receptors. Global or hepatocyte-specific CB1 knockout
mice are resistant to ethanol-induced steatosis and increases in
lipogenic gene expression and have increased carnitine
palmitoyltransferase 1 activity, which, unlike in controls, is not
reduced by ethanol treatment. Ethanol feeding increases the hepatic
expression of CB1 receptors and upregulates the endocannabinoid
2-arachidonoylglycerol (2-AG) and its biosynthetic enzyme
diacylglycerol lipase b selectively in hepatic stellate cells. In
control but not CB1 receptor-deficient hepatocytes, coculture with
stellate cells from ethanol-fed mice results in upregulation of CB1
receptors and lipogenic gene expression. We conclude that paracrine
activation of hepatic CB1 receptors by stellate cell-derived 2-AG
mediates ethanol-induced steatosis through increasing lipogenesis and
decreasing fatty acid oxidation."
and
"Although alcoholic fatty liver is reversible in its early
stages by cessation of drinking, this is often not feasible. The
present findings suggest that treatment with a CB1 antagonist may slow
the development of steatosis and thus prevent or delay its progression
to more severe and irreversible forms of liver disease. Importantly,
our finding that the steatogenic effect of ethanol specifically
involves CB1 receptors expressed in hepatocytes suggests that
selective targeting of peripheral CB1 receptors may be effective in
this pathology, thereby reducing the potential for centrally mediated
adverse effects of CB1 blockade, such as anxiety and depression
(Pacher et al., 2006). The additional antifibrogenic effect of CB1
blockade could add to the benefit of such treatment."
https://www.sciencedirect.com/science/article/pii/S1550413107003804/pdfft?md5=ac54de6d739e3cab493ff27893441f7a&pid=1-s2.0-S1550413107003804-main.pdf
[1957]
*The Fas receptor is a death receptor on the surface of cells that
leads to programmed cell death (apoptosis) if it binds its ligand, Fas
ligand (FasL). It is one of two apoptosis pathways, the other being
the mitochondrial pathway.
https://en.wikipedia.org/wiki/Fas_receptor
[1956]
To these antisteatogenic Benedictions we may add the deduction, from
alcohol spending, of cannabis expenditure.
In support of their findings they cite Yeong et al:
"In view of the observed upregulation of CB1 receptors and their
endogenous ligand 2-AG in ethanol-fed mice, we tested whether
activation of CB1 receptors contributes to the development of
ethanol-induced steatosis. Male mice were treated every other day with
intraperitoneal injections of vehicle or 10 mg/kg of the CB1
antagonist SR141716 (rimonabant) throughout their 3 week exposure to
the ethanol-containing diet. Body weight gain and ethanol intake were
slightly lower in the rimonabanttreated mice than in their controls,
but the intake of ethanol per g of body weight was similar in the two
groups, and blood ethanol concentrations were also similar (see Figure
S1 available online). Despite this, rimonabant-treated mice were
resistant to the steatogenic effect of ethanol: their hepatic lipid
content, as verified histologically and by measuring hepatic
triglyceride concentrations, was not different from that of mice on
the control liquid diet (Figures 1F and 1G), although rimonabant did
not prevent the rise in plasma ALT levels."
and
"Ethanol-induced steatosis can be prevented or reversed by in
vivo treatment with AMPK activators such as metformin (Yamauchi et
al., 2002), adiponectin (Bergheim et al., 2006), or
5-aminoimidazole-4-carboxamide-1-b-D-furosamide (AICAR) (Tomita et
al., 2005), and the phytocannabinoid D9 -tetrahydrocannabinol has been
shown to inhibit hepatic AMPK activity (Kola et al.,
2005)."
https://www.sciencedirect.com/science/article/pii/S1550413107003804/pdfft?md5=ac54de6d739e3cab493ff27893441f7a&pid=1-s2.0-S1550413107003804-main.pdf
[1957]
Kola et al indeed aver that THC outperforms 2-AG in antisteatotic
activity
"While leptin, which is associated with appetite suppression,
inhibits AMPK activity in the arcuate and paraventricular nucleus of
the hypothalamus, ghrelin has been shown to stimulate whole
hypothalamic AMPK activity after peripheral administration. In the
current study using a functional AMPK assay we observed that in whole
hypothalamus total AMPK activity increased to 153 8% of control after
central 2-AG injection and to 156 26% after i.c.v. ghrelin injection
(Fig. 1A). Similar responses were also seen after peripheral injection
of THC (174 31% of control) and ghrelin (177 12%, Fig. 1B). This
increase in AMPK activity was, as expected, associated with an
increase in Thr-172 phosphorylation of AMPK (Fig. 1, C and D), while
total AMPK levels did not change in either of the tissues studied. One
of the best established downstream targets of AMPK (and therefore a
good marker for AMPK activation) is ACC. Phosphorylation by AMPK at
the equivalent sites on the two isoforms ACC1 [acetyl coenzyme A
carboxylase 1] and ACC2 causes inhibition of fatty acid synthesis and
stimulation of fatty acid oxidation, respectively. Using an antibody
that detects phosphorylation of both isoforms, we detected an increase
in phosphorylation of ACC after central cannabinoid and ghrelin
treatment in the hypothalamus (Fig. 1E). We and others have described
important peripheral effects of desacyl ghrelin (see Ref. 8 and
references therein), although this form cannot activate the
full-length, functionally active GHS-R1a [growth hormone secretagogue
receptor 1a]. In this study no change was observed in hypothalamic
AMPK activity (Fig. 1F) or AMPK phosphorylation (Fig. 1G) after i.c.v.
administration of desacyl ghrelin."
The effects of AMPK in the liver and the cardiovascular system must
be distinguished.
"AMPK is activated by ischemia in the heart, leading to
increased glucose uptake and phosphorylation of the heart-specific
6-phosphofructo-2-kinase, which activates production of ATP by
glycolysis under anaerobic conditions. Activation of AMPK during
ischemia also lowers malonyl-CoA and thus increases ATP generation via
fatty acid oxidation during reperfusion. Recent results using mice
expressing a dominant negative AMPK mutant in the heart suggest that
the presence of AMPK protects cardiac ATP levels and reduces infarct
size and damage to myocytes during ischemia. The lack of fat tissue
cytokine adiponectin (known to stimulate AMPK activity) results in
pressure overload and cardiac hypertrophy in knock-out animals, and
this could be reversed by the reintroduction of adiponectin. Recent
data suggest that long term cannabinoid treatment improves
atherosclerosis via a CB2-mediated effect on immune cells. Our present
data suggest that the beneficial effects of cannabinoids could be
mediated via activation of AMPK, although excessive activation of AMPK
may be deleterious to the heart. We also found a large increase in the
phosphorylation and activity of AMPK activity in response to ghrelin.
There have been several previous studies describing the beneficial
effects of ghrelin and its synthetic analogues on cardiovascular
function. These seem to be direct effects that are independent of
growth hormone release, as positive results were obtained both in
hypophysectomized rats and in in vitro studies on embryonic (H9c2) and
adult (HL-1) heart muscle cell lines. Ghrelin and GHS-R mRNA are
present in human myocardium, and protein expression has also been
detected both in primary tissue and in the HL-1 cell line, where
ghrelin has anti-apoptotic effects. Diastolic dysfunction associated
with myocardial stunning is improved with ghrelin analogue treatment.
Human studies have shown that ghrelin increases stroke volume both in
healthy volunteers and in chronic heart failure, while chronic
administration of ghrelin improves left ventricular dysfunction and
attenuates the development of cardiac cachexia in rats with heart
failure. As elevated ghrelin levels have been reported in patients
with cardiac cachexia, this could be part of a compensatory mechanism
in response to catabolic-anabolic imbalance. In patients with obesity
(or other insulin-resistant states that are associated with low
ghrelin levels, such as type 2 diabetes and polycystic ovarian
syndrome) the low levels of ghrelin could contribute to heart failure,
where cardiomyocyte apoptosis is known to play a role. In contrast,
the beneficial effects of weight loss on cardiac function may, at
least in part, be the result of the beneficial effects of increased
ghrelin levels."
and in sum
"We have shown that both cannabinoids and ghrelin stimulate AMPK
activity in the hypothalamus and the heart and inhibit AMPK activity
in the liver and adipose tissue, while we found no effect on skeletal
muscle. Given the proposed role of AMPK in energy sensing and
metabolism, the present findings provide important evidence of
interactions between this enzyme and the orexigenic actions of
cannabinoids and ghrelin. Either class of agent could potentially
increase appetite by central AMPK stimulation or by facilitating the
restorative actions of AMPK as the hypothalamus senses fuel
deprivation. By contrast, peripheral inhibition of AMPK by
cannabinoids and ghrelin may lead to fuel, particularly fat, storage.
The combined effect of both central and peripheral signals would
therefore be increased food intake and lipid storage, leading to lipid
deposition. The cardiac and metabolic effects of cannabinoids we
report may have important implications for the anticipated widespread
clinical use of rimonabant and other CB1 antagonists in the treatment
of obesity."
https://www.jbc.org/article/S0021-9258(20)65672-1/pdf
[1958]
In 2006 Pi-Sunyer et al similarly reported positive results with this
frankencannabinoid:
"At year 1, the completion rate was 309 (51%) patients in the
placebo group, 620 (51%) patients in the 5 mg of rimonabant group, and
673 (55%) patients in the 20 mg of rimonabant group. Compared with the
placebo group, the 20 mg of rimonabant group produced greater mean
(SEM) reductions in weight (-6.3 [0.2] kg vs -1.6 [0.2] kg;
P<.001), waist circumference (-6.1 [0.2] cm vs -2.5 [0.3] cm;
P<.001), and level of triglycerides (percentage change, -5.3 [1.2]
vs 7.9 [2.0]; P<.001) and a greater increase in level of
high-density lipoprotein cholesterol (percentage change, 12.6 [0.5] vs
5.4 [0.7]; P<.001). Patients who were switched from the 20 mg of
rimonabant group to the placebo group during year 2 experienced weight
regain while those who continued to receive 20 mg of rimonabant
maintained their weight loss and favorable changes in cardiometabolic
risk factors. Use of different imputation methods to account for the
high rate of dropouts in all 3 groups yielded similar results.
Rimonabant was generally well tolerated; the most common drug-related
adverse event was nausea (11.2% for the 20 mg of rimonabant group vs
5.8% for the placebo group)."
https://jamanetwork.com/journals/jama/fullarticle/202374
[3970]
In
2008 Kola et al reported that "The Orexigenic Effect of Ghrelin
Is Mediated through Central Activation of the Endogenous Cannabinoid
System":
"Ghrelin did not induce an orexigenic effect in CB1-knockout
mice. Correspondingly, both the genetic lack of CB1 and the
pharmacological blockade of CB1 inhibited the effect of ghrelin on
AMPK activity. Ghrelin increased the endocannabinoid content of the
hypothalamus in wild-type mice and this effect was abolished by
rimonabant pre-treatment, while no effect was observed in CB1-KO
animals. Electrophysiology studies showed that ghrelin can inhibit the
excitatory inputs on the parvocellular neurons of the paraventricular
nucleus, and that this effect is abolished by administration of a CB1
antagonist or an inhibitor of the DAG lipase, the enzyme responsible
for 2-AG synthesis. The effect is also lost in the presence of BAPTA,
an intracellular calcium chelator, which inhibits endocannabinoid
synthesis in the recorded parvocellular neuron and therefore blocks
the retrograde signaling exerted by endocannabinoids. In summary, an
intact cannabinoid signaling pathway is necessary for the stimulatory
effects of ghrelin on AMPK activity and food intake, and for the
inhibitory effect of ghrelin on paraventricular neurons."
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0001797
[4200]
Shimizu et al (2009) brought the news that in mice...
"Intraperitoneal injection of nesfatin-1 suppressed food intake
in a dose-dependent manner."
https://academic.oup.com/endo/article-abstract/150/2/662/2455552
[4958]
"Current Understanding of the Role of Nesfatin-1" from
Schalla and Stengel (2018) in the Journal of Endocrinology:
https://academic.oup.com/jes/article/2/10/1188/5092030
[4959]
Despite Rimonabant's long-concluded life as a safe and effective drug
for obesity with the unfortunate side-effect of suicidal ideation (RIP
2006-2009), Folgueira et al were still unravelling its anorexigenic
mechanism in 2017, with "Pharmacological inhibition of
cannabinoid receptor 1 stimulates gastric release of nesfatin-1 via
the mTOR pathway" contributing to a leptin-independent
understanding of satiety:
"Despite being secreted by the same cells, Nucb2 and ghrelin have
opposing biological functions and regulation. Central and peripheral
administration of Nucb2 suppresses feeding behavior, while ghrelin
stimulates appetite. Interestingly, the fact that Nucb2 and ghrelin
are produced in the same gastric cells but in different vesicles
suggests that both proteins might experience differential regulation
at the gastric level to maintain energy balance. Supporting this
theory, Nucb2/nesfatin-1 production and regulation by nutritional
status decreases during fasting, while ghrelin levels are
up-regulated. Lastly, this decrease in Nucb2 production during fasting
conditions is concomitant with inhibition of the mTOR/pS6k1 pathway, a
sensor of the metabolic status of organism. Ghrelin secretion,
meanwhile, is negatively associated with mTOR/pS6k1 pathway activity
under fasting conditions.
"The cannabinoid system plays an important role as an endogenous
regulator of energy balance, acting at multiple levels. One of those
mechanisms includes its interaction with gastric ghrelin production to
regulate appetite and body weight. More specifically, the blockade of
the cannabinoid receptor CB1 decreases ghrelin expression in the
stomach, and this effect was mediated by activation of the mTOR/pS6k1
pathway. Taking into account the opposing functions and regulation of
ghrelin and Nucb2/nesfatin at the gastric level, as well as their
opposite relationship with the mTOR/S6K1 pathway, we sought to
investigate whether the cannabinoid system might also regulate
Nucb2/nesfatin-1 production in the stomach and whether the mTOR/pS6k1
intracellular pathway mediates this effect."
And you can see from the title that it did.
https://www.wjgnet.com/1007-9327/full/v23/i35/6403.htm
[4957]
So am I correct Slovenia is in a battle with alcohol?
And yet as drinkers and drink drivers, are many Slovenians not also
in a psychological battle against any IDEA disputing the idea that
excess alcohol is mandatory?
And isn't their IDEA of excess "more than I drink"?
Isn't the IDEA that cannabis is bad supportive of alcohol profits?
Isn't the IDEA that cannabis is protective of alcohol damage
unwelcome because it not only introduces the notion of alcohol damage,
but that it must be really serious, since we already have an IDEA of
how terrible cannabis is.
For alcohol must be really bad, if we are compelled by reason to take
such a drastic leap in favour of what we have been told is dangerous,
in order to combat the alcohol folk beliefs tell us is normal, but
which is objectively 114 times worse [852].
In the area of hepatology, motivated ignorance is fortunate: people
might notice that smoking cannabis helps them cope with a hangover,
but the histology of their liver is subclinical and on a day-by-day
basis this damage is invisible to them.
According to ElTebany et al in "Lower Rates of Hepatocellular
Carcinoma Observed Among Cannabis Users: A Population-Based
Study" (2022), to more than halve your chance of hepatocellular
carcinoma, you should "abuse cannabis".
For the variables tested, only being female gave a lower odds ratio
than cannabis (0.39 versus 0.45). (Table 3).
"Using data from the National Inpatient Sample (NIS) database
between 2002 and 2014, we identified the patients with HCC and
cannabis use diagnosis using the International Classification of
Disease 9th version codes (ICD-9). Then, we identified patients
without cannabis use as the control group. We adjusted for multiple
potential confounders and performed multivariable logistic regression
analysis to determine the association between cannabis abuse and
HCC.
"Results: A total of 101,231,036 patients were included in the
study. Out of the total, 996,290 patients (1%) had the diagnosis of
cannabis abuse versus 100,234,746 patients (99%) in the control group
without cannabis abuse. We noticed that patients with cannabis abuse
were younger (34 vs 48 years), had more males (61.7% vs 41.4%) and
more African Americans (29.9% vs 14.2%) compared with the control
group (P<0.001 for all). Besides, patients with cannabis use had
more hepatitis B, hepatitis C, liver cirrhosis, and smoking, but had
less obesity and gallstones, (P<0.001 for all). Using multivariable
logistic regression, and after adjusting for potential confounders,
patients with cannabis abuse were 55% less likely to have HCC
(adjusted Odds Ratio {aOR}, 0.45, 95% Confidence Interval {CI},
0.42-0.49, P<0.001) compared with patients without cannabis
abuse.
"Conclusion: Based on our large database analysis, we found that
cannabis use patients were 55% less likely to have HCC compared to
patients without cannabis use."
Gallstones (ICD-9-CM cod 574) were 40% lower in the cannabis group
(Table 1)
https://pmc.ncbi.nlm.nih.gov/articles/PMC9138632/
[1735]
In Slovenia, there were 231 new cases of cancer of the liver and
intrahepatic bile duct in 2018, of which 126 (54.5%) were
microscopically confirmed.
https://www.onko-i.si/fileadmin/onko/datoteke/rrs/lp/Letno_porocilo_2018.pdf
[1854]
And so applying the findings of ElTebany, of 55% less HCC in the
101,231,036 patients versus a 100% NECUD condition, a 0% incidence of
NECUD would have predicted 0.55 x 231 = 127 fewer cases in 2018, about
one case every three days.
Tajik et al found "Extracellular vesicles of cannabis with high
CBD content induce anticancer signaling in human hepatocellular
carcinoma" (2022):
"The discovery of extracellular vesicles in the 1950s opened new
insights into the understanding of intercellular, inter-species, and
inter-kingdom communications. EVs, nano-sized bilayer lipid vesicles,
are being released from different cell types and can be classified
into subgroups, namely apoptotic bodies, microvesicles, and exosomes,
according to their origin and size. Apoptotic bodies (10005000 nm) are
being generated from the cells that undergo apoptosis, to be
phagocytosed. Microvesicles are being originated from phospholipid
membrane with a size range of 1501000 nm. Exosomes with 30150 nm in
size are being derived from multi-vesicular bodies (MVBs. Naturally,
EVs transfer endogenous molecules as cargo to recipient cells. In
EV-based therapeutics, molecules such as siRNA, microRNA, as well
chemicals, and biological drugs have been encapsulated within these
vehicles to be delivered to the targets of interest. Exosomes have
been considered as the promising biomarkers in the early diagnosis of
diseases such as infectious diseases, autoimmune disorders, diabetes,
and several types of cancers. Recently, large-scale production of EVs
from edible and herbal plants (range in size, 30500 nm) has been
noticed as an excellent source of nanovesicles with phenomenal
intrinsic properties and known minimal side-effects."
and in their test comparing EVs from high and low CBD strains, both
with THC:
"Cytotoxicity assay showed that H.C-EVs strongly decreased the
viability of two hepatocellular carcinoma (HCC) cell lines, HepG2 and
Huh-7, in a dose and time-dependent manner compared with L.C-EVs.
H.C-EVs had no significant effect on HUVECs normal cell growth. The
finding showed that the H.C-EVs arrested the G0/G1 phase in the cell
cycle and significantly induced cell death by activating
mitochondrial-dependent apoptosis signaling pathways in both HCC cell
lines."
https://www.sciencedirect.com/science/article/pii/S0753332222005984?via%3Dihub
[2961]
Esmaeli and Dehabadi at Gerash University of Medical Sciences, Iran
(2025) reviewed 16 mixed studies on CBD and hepatocellular cancer:
"A systematic search (PubMed, Scopus, Web of Science, Google
Scholar) up to March 2025 identified 16 relevant studies (in vitro, in
vivo, clinical). CBD exerts antitumor effects via multiple pathways,
including apoptosis, autophagy regulation, metastasis suppression, and
tumor microenvironment modulation. CBD interacts with the
endocannabinoid system (ECS), inhibits oncogenic signaling
(PI3K/AKT/mTOR), and enhances chemotherapeutic efficacy (sorafenib,
cabozantinib). Studies show CBD induces pyroptosis via
caspase-3/GSDME, and modulates autophagy by inhibiting the
PI3K/Akt/mTOR pathway. It also sensitizes HCC cells to sorafenib and
cabozantinib. Preclinical results are promising, but clinical studies
are limited."
https://link.springer.com/content/pdf/10.1186/s12935-025-03870-3.pdf
[5090]
The Court may recall CBN was found to be beneficial to mitochondrial
biogenesis [876,877]. Akbari and Taghizadeh-Hesary (2023) looked at "COVID-19
induced liver injury from a new perspective: Mitochondria",
pointing out that:
"Patients with COVID-19 are at high risk of liver damage.
"The underlying mechanism is still undefined.
"SARS-CoV-2 can damage mitochondria directly or through systemic
inflammation.
"COVID-induced liver injury is more in patients with weaker
mitochondria.
"Boosting mitochondria can protect liver from COVID-induced
injury."
Moreover:
"Upon entering the hepatocytes, the RNA and RNA transcripts of
SARS-CoV-2 engages the mitochondria. This interaction can disrupt the
mitochondrial electron transport chain. In other words, SARS-CoV-2
hijacks the hepatocytes mitochondria to support its replication. In
addition, this process can lead to an improper immune response against
SARS-CoV-2. Besides, this review outlines how mitochondrial
dysfunction can serve as a prelude to the COVID-associated cytokine
storm. Thereafter, we indicate how the nexus between COVID-19 and
mitochondria can fill the gap linking CiLI and its risk factors,
including old age, male sex, and comorbidities. In conclusion, this
concept stresses the importance of mitochondrial metabolism in
hepatocyte damage in the context of COVID-19. It notes that boosting
mitochondria biogenesis can possibly serve as a prophylactic and
therapeutic approach for CiLI."
https://www.sciencedirect.com/science/article/pii/S1567724923000338
[4986]
Huang et al (2025) examined "The protective role of cannabidiol
in stress-induced liver injury: modulating oxidative stress and
mitochondrial damage":
"CBD exhibited significant protective effects against
stress-induced liver injury in mice. Decreases in liver function
indicators (including Aspartate Aminotransferase (AST) and Alanine
Aminotransferase (ALT)) and inflammatory cytokines (such as IL-1β
and Tumor Necrosis Factor-alpha (TNF-α)) were observed. CBD
enhanced CB2R expression and reduced α-SMA levels, mitigating
liver fibrosis. It also decreased ACSL4 levels, increased SOD and
GSH-Px activities, and upregulated SLC7A11 protein expression.
Furthermore, CBD improved mitochondrial morphology, indicating a
reduction in oxidative cell death.
"Conclusion: CBD activates the CB2R/α-SMA pathway to
modulate liver inflammation and fibrosis. Through the SLC7A11/ACSL4
signaling pathway, CBD alleviates oxidative stress in stress-induced
liver injury, enhances mitochondrial morphology, and reduces liver
damage. These findings provide a theoretical basis for the potential
application of CBD in the prevention and treatment of stress-induced
liver injury."
https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2025.1567210/full
[5184]
Zhan et al (2025) reveal how "Cannabidiol attenuates the
LPS/D-Galactosamine-induced acute liver injury by inhibiting
parkin-mediated ubiquitination of MFN2":
"In vivo, an A-LI mouse model was induced by LPS/D-GalN. Each
group was treated with or without LPS/D-GalN or CBD. H&E staining,
alanine aminotransferase (ALT), aspartate aminotransferase (AST) level
assay, TUNEL staining, TEM, IF, RT-qPCR, Western blot, Co-IP and
adeno-associated virus (AAV) infection were performed. In vitro,
RAW264.7 cells were stimulated with LPS. CCK-8, ELISA, MMP,
mitochondrial ROS assay, siRNA knockdown and plasmid overexpression
were performed.
"Results: CBD (2.5 or 5 mg kg-1) mitigated LPS/D-GalN-induced
liver damage, suppressed inflammatory cytokine expression, reduced
hepatocellular apoptosis, and inhibited oxidative stress. CBD
treatment increased hepatic mitofusin-2 (MFN2) protein while
decreasing Parkin-MFN2 binding and MFN2 ubiquitination. In RAW264.7
cells, CBD pretreatment (2.5 or 5 μM) dose-dependently attenuated
LPS-induced inflammation, apoptosis, and mitochondrial dysfunction and
likewise elevated MFN2 levels while limiting its ubiquitination. MFN2
knockdown abolished CBD's protective effects, whereas MFN2
overexpression restored them. Consistently, AAV-mediated delivery of
MFN2-targeting short hairpin RNA reversed the hepatoprotective action
of CBD in vivo.
"Conclusion: CBD mediates anti-inflammatory and hepatoprotective
effects by inhibiting MFN2 degradation through disrupting the
interaction between Parkin and MFN2."
https://pubmed.ncbi.nlm.nih.gov/41419044/
[5754]
Degrave et al (2025) examined the "Effects of five cannabis oils
with different CBD: THC ratios and terpenes on hypertension,
dyslipidemia, hepatic steatosis, oxidative stress, and CB1 receptor in
an experimental model":
"Male Wistar rats were fed either a: (1) reference diet (RD;
standard commercial laboratory diet) or a: (2) sucrose-rich diet (SRD)
for 3 weeks. 3 to 7 SRD + CO as following: (3)
SRD + THC; (4) SRD + CBD; (5)
SRD + CBD:THC 1:1; (6) SRD + CBD:THC 2:1; and
(7) SRD + CBD:THC 3:1. The COs were administered orally at
a dose of 1.5 mg total cannabinoids/kg body weight daily. The
cannabinoid and terpenes content of all COs used in the study was
determined. The terpenes found in COs were beta-myrcene, d-limonene,
terpinolene, linalool, beta-caryophyllene, alpha-humulene, (-)-guaiol,
(-)-alpha-bisabolol. During the experimental period, body weight, food
intake and blood pressure were measured. Serum glucose, triglyceride,
total cholesterol, uric acid, alanine aminotransferase (ALT),
aspartate aminotransferase (AST), and alkaline phosphatase (AP) levels
were evaluated. Liver tissue histology, NAFLD activity score (NAS),
triglyceride and cholesterol content, lipogenic enzyme activities,
enzyme related to mitochondrial fatty acid oxidation, reactive oxygen
species (ROS), thiobarbituric acid reactive substance (TBARS), and
antioxidant enzyme activities were also evaluated. The CB1 receptor
expression was also determined.
"Results
The results showed that SRD-fed rats developed hypertension,
dyslipidemia, liver damage, hepatic steatosis, lipid peroxidation, and
oxidative stress. This was accompanied by upregulation of liver CB1
receptor expression. CBD-rich CO, CBD:THC 1:1 ratio CO; CBD:THC 2:1
ratio CO and CBD:THC 3:1 ratio CO showed antihypertensive properties.
THC-rich CO, CBD:THC 1:1 ratio CO; CBD:THC 2:1 ratio CO showed the
greatest beneficial effects against hepatic steatosis and liver
damage. All COs exhibited antioxidant effects in liver tissue. This
was associated with normal liver CB1 receptor expression."
...
"Figure 5A and B shows that liver ROS and TBARS were
significantly increased (P < 0.05) in the SRD group
compared to the RD group. When CBD-rich CO, THC-rich CO, CBD:THC ratio
1:1 CO, CBD:THC ratio 2:1 CO and CBD:THC ratio 3:1 CO were
administered in the SRD, these parameters decreased significantly
(P < 0.05) reaching similar values to those of the RD
group. In addition, the decrease in the GSH content in the liver of
the SRD group was increased (P < 0.05) in the
SRD + CBD, SRD + THC,
SRD + CBD:THC 1:1, SRD + CBD:THC 2:1 and
SRD + CBD:THC 3:1 groups, reaching values similar to those
of the RD group (Fig. 5C). Moreover, a significant decrease in CAT,
GPx and GR activities was observed in the SRD group
(P < 0.05). CBD-rich CO and THC-rich CO increased the
CAT activity, although the values were still lower than in the RD
group. CBD:THC ratio 1:1 CO, CBD:THC 2:1 ratio CO and CBD:THC ratio
3:1 CO increased the CAT activity, reaching values similar to those of
the RD group (Fig. 5D). GR activity was increased
(P < 0.05) in SRD + CBD,
SRD + THC and SRD + CBD:THC 1:1 groups,
although the values were still lower than in the RD group. In
contrast, the SRD + CBD:THC 2:1 and
SRD + CBD:THC 3:1 groups showed a further increase in GR
activity, reaching levels similar to the RD group (Fig. 5E). In Fig.
5F was observed an increased GPx activity in SRD + CBD,
SRD + THC and CBD:THC 1:1 groups, reaching values similar
to those of the RD group. In SRD + CBD:THC 2:1,
SRD + CBD:THC 3:1 groups, the GPx enzyme activity
increased significantly, although the values were still lower than
those in the RD group."
https://jcannabisresearch.biomedcentral.com/articles/10.1186/s42238-025-00286-8
[5286]
Bader Eddin et al (2025) concentrated their attention on how
"β-Caryophyllene Ameliorates Thioacetamide-Induced Liver
Fibrosis in Rats: A Preventative Approach", describing
prophylactic effects:
"The BCP treatment (50 mg/kg) protected against cell injury and
potentiated antioxidant defense by replenishing hepatic GSH, improving
catalase activity, and inhibiting the formation of MDA. The
co-administration of BCP mitigated the TAA-induced inflammatory
response by decreasing the release of proinflammatory cytokines.
Histological examination showed preserved cellular integrity,
decreased collagen deposits with other extracellular matrix proteins,
and low levels of myofibroblast activation. In addition, the
BCP-treated rats demonstrated upregulated sirtuin 1 (SIRT1)
expression, which had a direct inhibitory effect on hypoxia inducible
factor (HIF-1α). AM630 pre-treatment inhibited all the
aforementioned protective mechanisms of BCP. Based on our findings,
BCP exerts protective effects in liver fibrosis, which can be
attributed to its agonist action on CB2 receptors. This study provides
preclinical evidence of the potential preventative benefits of BCP in
liver fibrosis."
https://www.mdpi.com/1422-0067/26/17/8493
[5413]
To avoid liver disease, you may quit alcohol. To quit alcohol or
opioids you may, on condition of your already successful cessation, be
prescribed the opioid receptor blocker Naltrexone - which also has
hepatotoxic risks. Common side effects of Naltrexone, which may be
administered orally or via long-term injection, include:
nausea
sleepiness
headache
dizziness
vomiting
decreased appetite
painful joints
muscle cramps
cold symptoms
trouble sleeping
toothache
Serious side effects of Naltrexone:
Severe reactions at the site of injection, including: intense pain;
tissue death for which surgery may be required; swelling, lumps, or
hardness; scabs, blisters, or open wounds
Liver damage or hepatitis, including; stomach area pain lasting more
than a few days; dark urine; yellowing of the whites of your eyes;
tiredness
Serious allergic reactions, including: skin rash; swelling of face,
eyes, mouth, or tongue; trouble breathing or wheezing; chest pain;
feeling dizzy or faint
Pneumonia
Depressed mood
https://www.samhsa.gov/medications-substance-use-disorders/medications-counseling-related-conditions/naltrexone
[3811]
CaPs of course are not commonly associated with these
experiences.
----------------------------------------------------------------------------
The Englishman stands for the rights of everyone disadvantaged,
discriminated against, persecuted, and prosecuted on the false or
absent bases of prohibition, and also believes the victims of these
officially-sanctioned prejudices have been appallingly treated and
should be pardoned and compensated.
The Englishman requests the return of his
CaPs and other rightful property, for whose distraint Slovenia has
proffered no credible excuse or cause.
The Benedictions represent both empirical entities as well as
beliefs. Beliefs which the Defence evidence shows may be
reasonably and earnestly held about the positive benefits of CaPs
at the population level, in which the good overwhelmingly
outweighs the bad. Below, the latest version of this dynamic
list.
THE BENEDICTIONS
REFERENCES
TIMELINE OF DRUG LAW v. SCIENCE