ENTOURAGE EFFECT
Synergies of cannabinoids and terpene - the
influence of RDTGH - Three cancers - Superstitions in the time of Smuts - pain
and alcohol meet the entourage - blocking addiction to opioids - Twelve cancers
- Sleep - ZPPPD is a testicle-limiting law - Glymphatic and hemifusome systems - To
pharmocratic reductionism
and back again
"Understanding the intricate
interplay between cannabinoids, terpenes, and flavonoids is paramount for
realizing the full therapeutic benefits of cannabis," say Al-Khazaleh et al
(2024)
"Cannabinoids, pivotal in cannabis’s
bioactivity, exhibit well-documented analgesic, anti-inflammatory, and
neuroprotective effects. Terpenes, aromatic compounds imbuing distinct flavours,
not only contribute to cannabis’s sensory profile but also modulate cannabinoid
effects through diverse molecular mechanisms. Flavonoids, another cannabis
component, demonstrate anti-inflammatory, antioxidant, and neuroprotective
properties, particularly relevant to neuroinflammation. The entourage hypothesis
posits that combined cannabinoid, terpene, and flavonoid action yields
synergistic or additive effects, surpassing individual compound efficacy.
Recognizing the nuanced interactions is crucial for unravelling cannabis’s
complete therapeutic potential. Tailoring treatments based on the holistic
composition of cannabis strains allows optimization of therapeutic outcomes
while minimizing potential side effects."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10821245 [4417]
To this end, Namdar et al of the
Institute of Plant Sciences and the Israeli Gene Bank
"...found that in 'high THC' or 'high
CBD' strains, phytocannabinoids are produced alongside certain sets of
terpenoids. Only co-related terpenoids enhanced the cytotoxic activity of
phytocannabinoids on MDA-MB-231 and HCT-116 cell lines. This was found to be
most effective in natural ratios found in extracts of cannabis inflorescence.
The correlation in a particular strain between THCA or CBDA and a certain set of
terpenoids, and the partial specificity in interaction may have influenced the
cultivation of cannabis and may have implications for therapeutic treatments."
The scientists discovered that for
cytotoxicity in MDA-MB-231 and HCT-116 cell lines, ingredients that went
together went together.
"In this paper we present a clear
example of the inter-entourage effect on cytotoxic activity. We showed: (1) A
significant correlation between certain terpenoids and the main
phytocannabinoids in various C. sativa strains. (2) Terpenoids, present in
relatively minute amounts in cannabis extracts and possessing no therapeutic
effect by themselves at these concentrations, add to the cytotoxicity of the
dominant phytocannabinoid. This demonstrates the inter-entourage effect in
cannabis treatments. (3) The inter-entourage interaction is specific, in part,
since THC activity was enhanced only by its co-related terpenoids, at terpenoid
to phytocannabinoid ratios found naturally in the plant, while CBD was more
tolerant. (4) The relative ratio of phytocannabinoid to terpenoids,
demonstrating the enhanced biological activity, entitled entourage effect,
showed nonlinear dose dependency, rather a dose-specificity mode of action."
https://www.mdpi.com/1420-3049/24/17/3031/pdf?version=1566384625 [4418]
The "top 25 cannabinoids" are mapped
out and grouped and described:
https://www.higherlearninglv.co/post/cannabinoid-clinic-research-based-training
[2178]
In 2006 Varvel et al
"investigated whether CBD may
modulate the pharmacological effects of intravenously administered THC or
inhaled marijuana smoke on hypoactivity, antinociception, catalepsy, and
hypothermia, the well characterized models of cannabinoid activity."
They found
"Intravenously administered CBD
possessed very little activity on its own and, at a dose equal to a maximally
effective dose of THC (3 mg/kg), failed to alter THC's effects on any measure.
However, higher doses of CBD (ED(50)=7.4 mg/kg) dose-dependently potentiated the
antinociceptive effects of a low dose of THC (0.3 mg/kg). Pretreatment with 30
mg/kg CBD, but not 3 mg/kg, significantly elevated THC blood and brain levels."
https://pubmed.ncbi.nlm.nih.gov/16572263/ [1796]
A UK study by Imperial College looked
at childhood epilepsy, again making the astonishing discovery that THC and CBD
work better together.
"Twenty-three (65.7%) patients
achieved a 50% reduction in seizure frequency. 94.1% (n = 16) of patients
treated with CBD and 9 -THC observed a 50% reduction in seizure frequency
compared to 31.6% (n ¼ 6) and 17.6% (n = 3) of patients treated with CBD
isolates and broad-spectrum CBD products, respectively (p< 0.001)."
https://www.thieme-connect.de/products/ejournals/pdf/10.1055/a-2002-2119.pdf
[2180]
It's almost as if it's part of some
divine plan! In 2017 King et al, at something called the "Center for Substance
Abuse Research" in Philadelphia discovered that THC and CBD go together! They
work better together at treating the symptoms of anti-cancer drugs with lots of
side effects.
"Both CBD and THC alone attenuated
mechanical allodynia [touch-sensitive pain] in mice treated with paclitaxel.
Very low ineffective doses of CBD and THC were synergistic when given in
combination. CBD also attenuated oxaliplatin- but not vincristine-induced
mechanical sensitivity, while THC significantly attenuated vincristine- but not
oxaliplatin-induced mechanical sensitivity. The low dose combination
significantly attenuated oxaliplatin- but not vincristine-induced mechanical
sensitivity."
https://bpspubs.onlinelibrary.wiley.com/doi/10.1111/bph.13887 [1325]
Ozmen et al (2024) found CBD reduced
the harm caused by another cancer drug.
"Methotrexate (MTX) is a widely used
medication for various cancers, yet its use is associated with adverse effects
on organs, notably the lungs. Cannabidiol (CBD), known for its antioxidant and
anti-inflammatory properties, was investigated for its potential protective
effects against MTX-induced lung injury. Thirty-two female Wistar Albino rats
were divided into four groups: control, MTX (single 20 mg/kg intraperitoneal
dose), MTX + CBD (single 20 mg/kg MTX with 0.1 ml of 5 mg/kg CBD for 7 days
intraperitoneally) and CBD only (for 7 days). Lung tissues were analysed using
histopathological, immunohistochemical and PCR methods after the study.
Histopathological assessment of the MTX group revealed lung lesions like
hyperemia, edema, inflammatory cell infiltration and epithelial cell loss.
Immunohistochemical examination showed significant increases in Cas-3, tumour
necrosis factor-alpha (TNF-α) and nuclear factor-kappa B (NF-κB) expressions.
PCR analysis indicated elevated expressions of apoptotic peptidase activating
factor 1 (Apaf 1), glucose-regulated protein 78 (GRP 78), CCAAT-enhancer-binding
protein homologous protein (CHOP) and cytochrome C (Cyt C), along with reduced
B-cell lymphoma-2 (BCL 2) expressions in the MTX group, though not statistically
significant. Remarkably, CBD treatment reversed these findings."
https://onlinelibrary.wiley.com/doi/10.1111/bcpt.13992 [3845]
In "Cannabidiol Increases
Psychotropic Effects and Plasma Concentrations of Δ9-Tetrahydrocannabinol
Without Improving Its Analgesic Properties" Gorbenko et al (2024) found the
influence of CBD on THC to be rather different to what most would expect:
"Cannabidiol (CBD), the main
non-intoxicating compound in cannabis, has been hypothesized to reduce the
adverse effects of Δ9-tetrahydrocannabinol (THC), the main psychoactive and
analgesic component of cannabis. This clinical trial investigated the hypothesis
that CBD counteracts the adverse effects of THC and thereby potentially improves
the tolerability of cannabis as an analgesic. A randomized, double-blind,
placebo-controlled, five-way cross-over trial was performed in 37 healthy
volunteers. On each visit, a double-placebo, THC 9 mg with placebo CBD, or THC
9 mg with 10, 30, or 450 mg CBD was administered orally. Psychoactive and
analgesic effects were quantified using standardized test batteries.
Pharmacokinetic sampling was performed. Data were analyzed using mixed-effects
model. Co-administration of 450 mg CBD did not reduce, but instead significantly
increased subjective, psychomotor, cognitive, and autonomous effects of THC
(e.g., VAS 'Feeling High' by 60.5% (95% CI: 12.7%, 128.5%, P < 0.01)), whereas
THC effects with 10 and 30 mg CBD were not significantly different from THC
alone. CBD did not significantly enhance THC analgesia at any dose level.
Administration of 450 mg CBD significantly increased AUClast of THC (AUClast
ratio: 2.18, 95% CI: 1.54, 3.08, P < 0.0001) and 11-OH-THC (AUClast ratio: 6.24,
95% CI: 4.27, 9.12, P < 0.0001) compared with THC alone, and 30 mg CBD
significantly increased AUClast of 11-OH-THC (AUClast ratio: 1.89, 95% CI: 1.30,
2.77, P = 0.0013), and of THC (AUClast ratio: 1.44, 95% CI: 1.01, 2.04,
P = 0.0446). Present findings do not support the use of CBD to reduce adverse
effects of oral THC or enhance THC analgesia."
https://ascpt.onlinelibrary.wiley.com/doi/10.1002/cpt.3381 [3498]
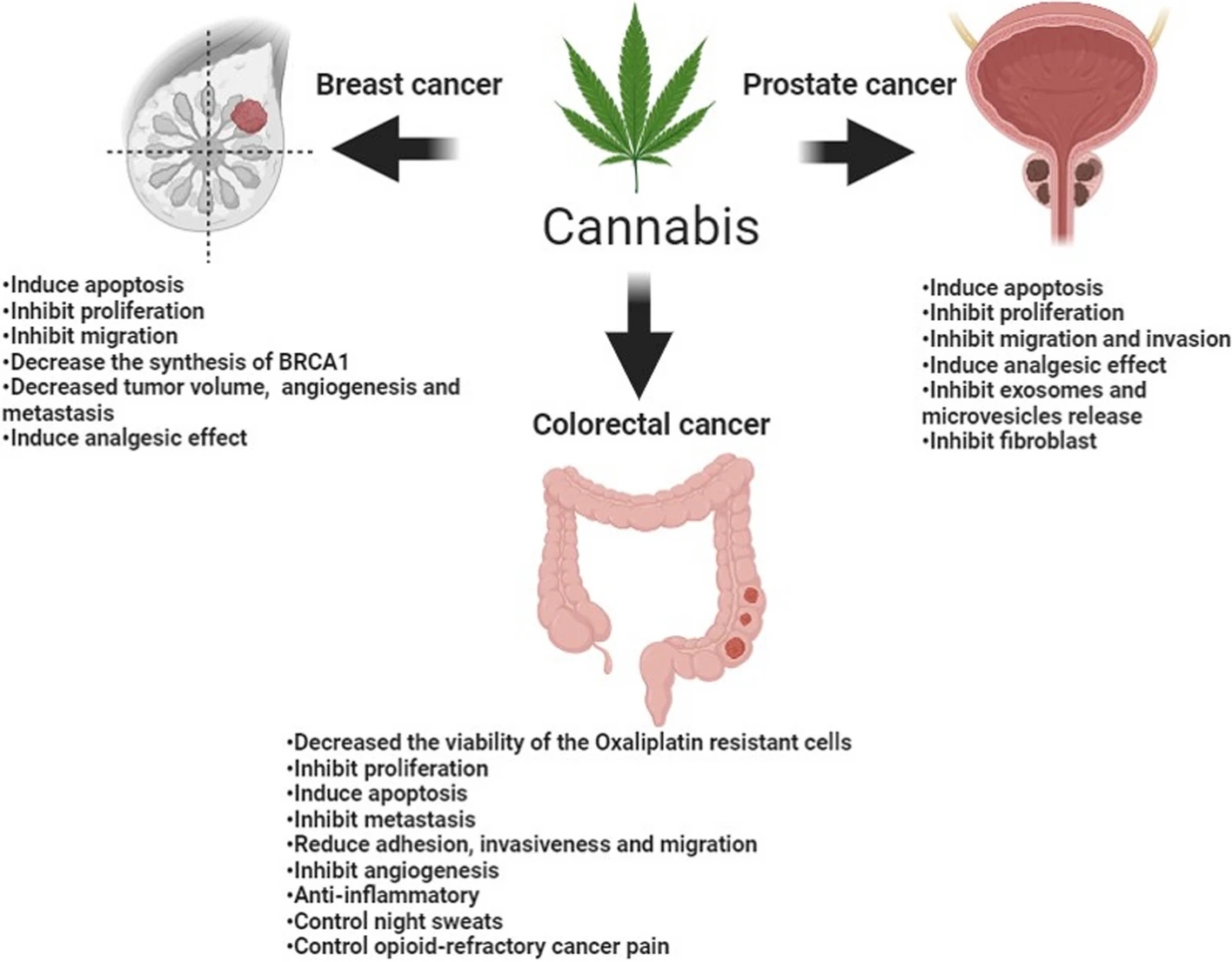
Summarising the benefits of cannabis
in "Cannabis and cancer: unveiling the potential of a green ally in breast,
colorectal, and prostate cancer" AlSalamat et al (2024) add to data on the
synergy of cannabinoids and oxaliplatin:
"Oxaliplatin is a chemotherapeutic
medication that is used to treat cancer. It is a platinum medication with
alkylating properties (O'Dowd et al. 2023). Oxaliplatin, like other alkylating
drugs, operates by interfering with the development of DNA in a cell. It kills
cells by preventing them from growing and replicating (O'Dowd et al. 2023). This
aids in the treatment of cancer, which is characterized by uncontrollable cell
growth and division (O'Dowd et al. 2023). Exploring novel techniques to improve
the efficacy of CRC treatment by identifying molecules and mechanisms linked
with oxaliplatin resistance is necessary (Jeong et al. 2019). CBD has the
potential to assist human CRC cells overcome Oxaliplatin resistance. Jeong et
al. conducted a study to demonstrate the effect of CBD on inducing autophagy in
Oxaliplatin resistance colorectal cancer cell (CRC), they generated
oxaliplatin-resistant cell lines, which didn’t respond to oxaliplatin treatment
(Jeong et al. 2019). When the cell lines were treated with a combination of CBD
and oxaliplatin, the death of oxaliplatin-resistant CRC was considerably raised
(Jeong et al. 2019). The authors also performed an in-vivo study on mice. They
injected a group of mice with oxaliplatin-resistant cell lines subcutaneously,
then they measured the tumor size and weight every 2 days. They found that both
size and weight of tumor were lower in mice that were treated with both
oxaliplatin and CBD than in the non-treated control group and mice that were
treated with either drug. The mechanism behind this is that CBD decreases NOS3
phosphorylation-which is essential for Oxaliplatin resistance development- and
superoxide dismutase-2 (which is an intracellular antioxidant) increasing
Reactive Oxygen Species (ROS) through mitochondrial dysfunction leading to
induce autophagy (Jeong et al. 2019)."
https://jcannabisresearch.biomedcentral.com/articles/10.1186/s42238-024-00233-z
[4655]
Summarising the anti-cancer activities of cannabis, Nigro et al (2021) say:
"Both THC and non-psychoactive cannabinoids have been reported to possess
peripheral anti-inflammatory properties in a plethora of in vitro and in vivo
models. In human peripheral blood cells, CB1 is expressed by B cells, NK cells,
neutrophils, CD8+ T cells, monocytes, and CD4+ T cells, whereas CB2 mRNA is
expressed by human B cells, NK cells, monocytes, neutrophils, and T cells.
Typically, CB2 inhibits the production of proinflammatory cytokines, such as
tumor necrosis factor alpha (TNF-𝛼), interleukin (IL)-2, IL-6, IL-8, and IFN-𝛾
by immune cells. CBD decreases peripheral inflammation through reduction of
prostaglandin E2 (PGE2), nitric oxide (NO), and malondialdehyde production. In
addition, CBD, in combination with minor phytocannabinoids of Cannabis sativa L.
extracts, can induce a greater pharmacological anti-inflammatory activity.
Indeed, a standardized cannabis extract enriched with CBD exerts a more powerful
anti-inflammatory activity than CBD alone. Besides CBD, THC also possesses
potent anti-inflammatory properties both in vivo and in vitro. Recently, in a
mouse model of acute respiratory distress syndrome, THC leads to the suppression
of the cytokine storm. The molecular mechanisms at the basis of THC
down-regulation of the inflammatory processes are various and tissue-dependent.
Indeed, regarding gastrointestinal and systemic inflammatory reactions, THC
suppresses both lymphocytes and neutrophils activity; in epithelial and skin
cells, THC inhibits the release of inflammatory mediators through impairment of
the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-kB)
pathway. It is of note that there is clear evidence of the synergistic action of
THC and CBD in terms of down-regulation of the inflammatory processes.
"Regarding other combination extracts, Shebabya et al. demonstrated that
Cannabis sativa L. oil extract markedly suppresses the release of TNF-α in
LPS-stimulated rat monocytes with inhibition of LPS-induced COX-2 and i-NOS
protein expression and blockage of MAPKs phosphorylation. Additionally, the
presence of phenols, terpenes, or other phytocannabinoids enhance the
therapeutic activity of CBD, defined as ‘entourage effects’. In addition,
cannabis extract inhibits the production of IL-8, matrix metallopeptidase
(MMP)-9, and vascular endothelial growth factor (VEGF), an effect not detected
with CBD alone, in skin cells. Other non-psychoactive cannabinoids,
including CBC and CBN, also showed substantial in vivo anti-inflammatory
responses. On the other hand, monoterpenes such as α- and β-pinene, myrcene, and
limonene have been also reported to possess substantial anti-inflammatory
properties.
"Regarding neuroinflammation, both CBD and THC have protective effects through
the activation of NF-𝜅B as well as the inhibition of Toll like receptor (TLR4).
Indeed, in a vitro model of LPS-stimulated neuroinflammation, CBD suppresses the
release of TNF-α, IL-1β, and IL-6 through the inhibition of NF-𝜅B
phosphorylation and the concomitant activation of COX and iNOS. In addition, THC
treatment selectively reduces CD8+ T cell response accompanied by inhibition of
IL-6 release. The combination of THC and CBD seems to be the most potent
anti-inflammatory drug able to inhibit the T helper response as well as CD4+ T
response in a mouse model of multiple sclerosis (MS).
"Beyond the regulation of inflammation, phytocannabinoids can prevent
proliferation, metastasis, and angiogenesis, as well as induce apoptosis in a
variety of cancer cell types. Treatments with CBC and THC or CBD led to cell
cycle arrest and cell apoptosis. Additionally, CBC and THC or CBD treatments
inhibit bladder urothelial carcinoma cell migration and affected F-actin
integrity.
"Beyond the actions of CBC, THC, and CBD on different pathways involved into
development of cancer cell types, also cannabigerol (CBG), cannabidivarin
(CBDV), cannabinol (CBN), cannabivarin (CBV), and tetrahydrocannabivarin (THCV)
have showed a role as anti-cancer for different cells line."
https://pmc.ncbi.nlm.nih.gov/articles/PMC8124362/
[5796]
For Anis et al (2025) "Targeting bladder cancer: Potent anti-cancer effects of
cannabichromene and delta-9-tetrahydrocannabinol-rich Cannabis sativa strains"
"A large retrospective epidemiological study revealed that cannabis use among
the general population may be associated with a reduced incidence of bladder
cancer. This association remained unexplained. We have previously shown that
cannabis-derived compounds have cytotoxic synergistic activity against UC cell
lines. Our work demonstrated a consistent inhibitory effect of cannabichromene
(CBC) and delta-9-tetrahydrocannabinol (THC) at well-defined concentrations and
ratios on UC cell proliferation, migration, cell cycle arrest, and
treatment-induced apoptosis of UC cells."
https://www.sciencedirect.com/science/article/pii/S2214388225000335?via%3Dihub#bib2
[5797]
Apparently the worst thing that can
happen to you if cannabinoids make you better is that you will actually feel
that you are better. Having such feelings is very much against the trend of
modern western pharmaceutical interventions.
"One of the major challenges for
future research is designing synthetic cannabinoids that elicit positive effects
of CB1 activation in peripheral neurons and in specific brain regions, but
without significant cognitive effects."
...say Scott et al in an otherwise
enthusiastic article loaded heavily in favour of synthetic cannabinoids. But it
remains inescapable that a plant got there first. [4027]
And how or why these "positive
effects of CB1 activation" must take place without cognitive effects is not
explained. An analogy:
"Alcohol free pubs allow people to
gather, and you can laugh, spill things, or fall over, leading to neuronal
stimulation, without the significant cognitive effects caused by alcohol."
Indeed no pro-alcohol researchers
claiming red wine has health benefits have ever claimed that it ought to be
alcohol-free red wine. So the feelgood benefits of wine and those of cannabis
are strangely set apart for no discernable reason. Except of course, the reason
that you won't get any money for supporting cannabis euphoria. Thus Dobovišek et
al are able to state in "Cannabinoids and triple-negative breast cancer
treatment" (2024):
"Cannabinoids show antitumor activity
in most preclinical studies in TNBC models and do not appear to have adverse
effects on chemotherapy."
and
"The antitumor effect of THC on
breast cancer cell lines was documented. Among the tumor cells, those with a
more aggressive phenotype, including the MDA-MB-231 cell line, were more
sensitive to THC."
and
"The antitumor efficacy of pure THC
was compared with that of an herbal drug preparation of fresh cannabis flowers
containing a variety of cannabinoids and terpenes. The herbal drug preparation
contained THC and CBG, but no CBD, and was more effective than pure THC in
producing antitumor responses in cell cultures and animal models of various
breast cancer subtypes, including the TNBC subtype (MDA-MB-231 and SUM159 cell
lines)."
and
" The herbal drug preparation was
significantly more potent than pure cannabinoid (the same dose of THC was
administered)."
As for reducing the harms of the
official cures:
"Importantly, the major cannabinoids
(THC, CBD, and cannabinol) and their metabolites found in the plasma of cannabis
users can inhibit several P450 enzymes, including CYP2B6, CYP2C9, and CYP2D6,
and cause pharmacokinetic interactions between these cannabinoids and
xenobiotics that are extensively metabolized by these enzymes. There is evidence
that cannabinoids alleviate peripheral neuropathic pain caused by chemotherapy
and prevent doxorubicin-induced cardiomyopathy. Both are side effects of taxane
and anthracycline chemotherapy, which is frequently used in TNBC."
While it may seem important that
"Cannabis use correlated with a
significant reduction in time to tumor progression and OS [overall survival].
Cannabis users were associated with a lower number of immune-related adverse
events (iAEs)."
The researchers do not seem to think
much of the placebo effect or belief:
"Many patients take cannabinoids in
the belief that this will help cure their disease, although there is currently
no clinical data to support this claim in breast cancer patients, including
TNBC. A survey of breast cancer patients found that 42% of survey participants
used cannabis to treat symptoms and about half of these participants believed
that cannabis could treat the cancer itself."
But it is as all this never existed
when we learn that, for some reason, CBD
"...is a non-psychoactive substance
and therefore a potential therapeutic agent."
https://www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2024.1386548/pdf
[3427]
Many researchers have plodded on obediently
with this "rather die than get high" mentality (RDTGH). Thus, in a study of
phytocannabinoids' effects upon calcium fluxes dependent on transient vanilloid
receptor type 1 only
"Cannabinoids other than the highly
psychoactive tetrahydrocannabinol (THC) that rank order in abundance directly
below THC in Cannabis chemotypes were selected for analysis. Cannabidiol (CBD),
Cannabinol (CBN) and the minor cannabinoids Cannabidiolic Acid (CBDA),
Cannabidivarin (CBDV), Cannabichromene (CBC), Cannabigerol (CBG), Cannabigerolic
Acid (CBGA) were selected."
They writhe around in a twisted mess
of self-interest and legality:
"Cannabinoids are of significant
interest in the context of 'medicinal' [note the sarcastic quotes] Cannabis use.
Pain is one of the most common indications for which medical marijuana is
legally allowed to be prescribed and is demanded by patients."
According to their thinking, which is
apparently anti-euphoria:
"The psychoactive nature of
THC-containing whole chemovars of Cannabis, which is typically the available
form of the drug in dispensaries, leads to regulatory issues and adverse
side-effects."
A key assumption is that a pain-free
existence and happiness are mututally exclusive - it sounds like a religious
idea. You can see what they are trying to do is like alcohol-free beer or decaf.
We could go on to take vitamin pills instead of eating vegetables. We have
meat-free protein, but perhaps what we really need is a scientist to design
protein-free meat.
"The distinct response profiles of
the different cannabinoids that we observe also provide the possibility of
fine-tuning or shaping desirable responses using cannabinoid mixtures. At the
level of the sensory neuron bundles, the fact that cannabinoids appear to
discriminate between TRP receptors and that the receptors in turn respond
distinctively to the compounds, again offers the potential for rational design
of therapeutic mixtures."
Their 2019 ideas for the future are
not much use if you wanted pain relief in 2012 or 1991, are they?
While they continue to tinker around,
there's this plant, isn't there?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6557596/ [1639]
Other researchers are more understanding to THC and other CCx. Consider Reva et
al (2025) who examined "Comparative Effects of THC and CBD on
Chemotherapy-Induced Peripheral Neuropathy: Insights from a Large Real-World
Self-Reported Dataset":
"Chemotherapy-induced peripheral neuropathy (CIPN) is a common dose-limiting
adverse effect of various chemotherapeutic agents. Previous work demonstrated
that cannabis alleviates symptoms of oxaliplatin-induced CIPN. To evaluate the
effects of cannabis components, cannabidiol (CBD) and tetrahydrocannabinol
(THC), on CIPN-related symptoms. Methods: We reviewed a patient-reported
outcomes dataset from 'Tikun Olam,' a major medical cannabis provider. Of 1493
patients, 802 reported at least one CIPN symptom at baseline, including a
burning sensation, cold sensation, paresthesia (prickling) and numbness, and 751
of them met the study inclusion criteria. Patients were categorized into
THC-high/CBD-low and CBD-high/THC-low groups. Symptom changes after six months
of cannabis use were analyzed using K-means clustering and logistic regression,
incorporating interactions between baseline symptoms and THC and CBD doses.
Linear regression assessed changes in activities of daily living (ADL) and
quality of life (QOL). Results: Both groups reported symptom improvement. The
THC-high group showed significantly greater improvement in burning sensation and
cold sensation (p = 0.024 and p = 0.008). Improvements in ADL and QOL were also
significantly higher in the THC group (p = 0.029 and p = 0.006). A significant
interaction between THC and CBD was observed for symptom improvement (p <
0.0001). Conclusions: Cannabis effectively reduces CIPN symptoms and improves
QOL and ADL. Higher THC doses were more effective than lower doses, with
combined CBD and THC doses yielding greater symptom relief."
https://www.mdpi.com/2227-9059/13/8/1921 [5352]
Is there any evidence Jan Smuts knew
anything about insulin in 1924? Here's an ngram.
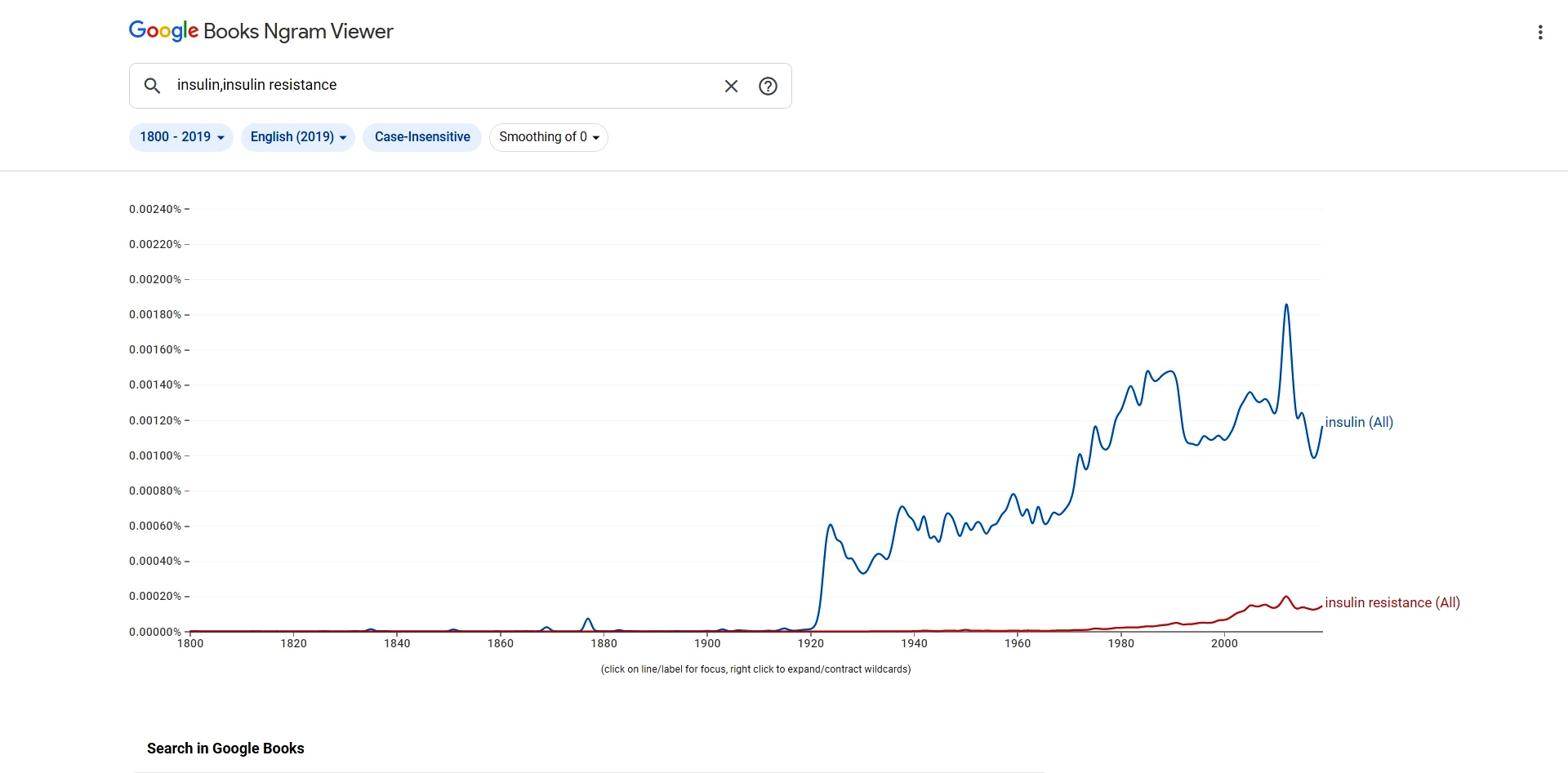
Smuts was a keen reader, so he might
have come across it. Would he have associated it in his mind with dagga? This
proposition is impossible to prove. Smuts' contributions to the field of
physiology are more of a philosophical nature:
"Also at that time, biological
science was evolving away from materialism as the pure physiology model of
nineteenth century. So, while psychology’s original aim was to explain all
mental activity by mechanical principles – with its failure on the physiological
level – biochemistry as the familiar partner of mechanistic physiology began
pointing in another, relativistic-biologic direction. Escaping this irrelevance,
biochemistry better and better differentiated living from dead matter and, as a
result, scientific interest turned to investigating living material. These
investigations produced questions more fundamental to human life; those about
organic material and about its biological phenomena, for example the process of
regeneration in nature (e.g., tapeworm survival after vivisection) and the
healing process in general. What grew to be a revolution in biology joined
phenomenology in conceptualizing organisms as unities. As Smuts (1926) had
conjectured philosophically and Goldstein (1934/1963) contended neurologically,
maintenance of the integrity of the whole cannot be deduced biochemically. Each
tissue and every organ seem to follow a law of the total organism."
Though he was probably interested in
battle wounds, the Defendant could find no evidence Smuts dug deeply into the small stuff,
like insulin. In the Boer War, if you got shot in a limb, they chopped it off.
If you were shot anywhere else, you died.
In fact the idea of lipid cell
membranes began in December 1925, with a paper by Gortel and Grendel at the
University of Leiden.
"It is clear that all our results fit
in well with the supposition that the chromocytes are covered by a layer of
fatty substances that is two
molecules thick."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2130960/pdf/439.pdf [2539]
Theories of cell membrane structure
continued through the prohibition era and various iterations of the cannabis
legislation:
"Then in the 1950s, Robertson
proposed a three-layer structure, where two layers of proteins were attached to
a lipid layer in the middle. A few years later Lenard and Singer suggested a
revised model, where the proteins were now allowed to span a lipid bilayer
structure. This picture was yet considered incomplete, and in 1972 Singer and
Nicolson proposed the famous 'fluid mosaic' model that is nowadays generally
known also as the Singer–Nicolson model."
But even by 2019, many mysteries were
unresolved:
"Biological membranes are everywhere.
All our cells are surrounded by a biological membrane. So also are the tiny
organelles such as the nucleus that contains our genetic code and the
endoplasmic reticulum that synthesizes most of our proteins. Biological
membranes keep us alive when they transfer oxygen from our lungs to our
bloodstream. Biomembranes also control our mood, because they host the receptors
of signaling molecules such as dopamine in our brain.
"It is quite intriguing that
membranes can play such crucial roles in maintaining life, yet these membranes
are basically just soft, few nanometers thick lipid interfaces. However, the
more closely one looks at them, the more complex they turn out to be. It is
quite justified to note that despite about 100 years of research, we still do
not understand exactly what biological membranes really look like."
https://pubs.acs.org/doi/10.1021/acs.chemrev.8b00538 [2531]
So obviously Smuts did not know
anything about that?
Smuts was already 55 by 1925. Germ
layer theory was wiped out in 1926. Endosymbiosis in evolutionary theory was
proposed in 1927. Penicillin arrived in 1928. ATP was discovered in 1929.
Vitalism had died by the end of the 20s. Essential fatty acids arrived in
1929/1930. Human metabolism was far removed from anything going on in Smuts'
head about cannabis.
https://www.researchgate.net/publication/367444844_Psychopathology/link/63d94b8dc465a873a271f667/download
[2129]
Here's another example of woo woo in
the way.
Jan Smuts or the League of Nations
could not have known in 1924 that
"The endocannabinoid system has
emerged as a key regulatory signaling pathway in the pathophysiology of
alcohol-associated liver disease (ALD). More than 30 years of research have
established different roles of endocannabinoids and their receptors in various
aspects of liver diseases, such as steatosis, inflammation, and fibrosis."
But what is curious is how the
introduction goes on. For, they warn
"However, pharmacological
applications of the endocannabinoid system for the treatment of ALD have not
been successful because of psychoactive side effects, despite some beneficial
effects."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8496755/ [2048]
Two things should strike the Court as
curious about this.
Firstly, nowhere do they query the
role of alcohol in alcohol-associated liver disease. For these authors these
liver diseases are alcohol-associated because it says so in the name. It is
incontrovertibly true that alcohol has gotten the ALD patients into this disease
spectrum.
Secondly, their complaint about
euphoria is entirely directed towards the putative medicaments for ALD.
Why is no one suggesting making
alcohol non-euphoric?
Rather than trying to cure liver
disease after you have drunk the legal drugs, why not make them ineffective? You
could limit the alcohol content to 0.2%. You could make it no crime to buy but
illegal to sell. Or you could make a complicated medical model concentrating the
supply into the hands of a coterie of doctors or therapists, thickening
Slovenia's starchy rentier economy. Why not do that?
Why, given the euphoria potential for
alcohol, is that not reason enough alone to stop people being attracted to it in
the first place?
And yet for someone who doesn't want
to be a fat alcoholic diabetic with cancer, these kind of measures are in
effect?
The euphoria of alcohol is brief, and
associated with a low BAC. Why are the scientists closing the barn door after
the horse has bolted?
So we have, essentially a "good
euphoria" in the past which has made all these people ill, and a "bad euphoria"
which - like most anxiety - concerns the future, specifically the future for
patentable pharmaceuticals that can target the endocannabinoid system without
the alcohol victim losing his shit. The Defence fears this is much more of a concern around
the former reason than the latter. "Bad euphoria" may be added to the list of
Prohibition's friends.
Later they come back to this
"limitation" of drugs that make you happy while fixing your alcohol-ravaged
liver:
"The endocannabinoid system has been
observed in both the hepatocytes and various nonparenchymal cells in the liver,
in which the endocannabinoid production and its receptor activation may
contribute to the development of a spectrum of ALD, ranging from simple
alcoholic steatosis to more severe forms such as steatohepatitis and fibrosis.
Therefore, understanding the precise physiology of the endocannabinoid system in
the liver and unveiling the mechanism underlying the association between ALD
progression and hepatic endocannabinoid signaling seem to bear a paramount
significance for the advancement of ALD treatment, as well as for the treatment
of other chronic liver diseases (e.g., NAFLD, viral hepatitis). Moreover,
developing efficacious and highly selective cannabinoid receptor–modulating
drugs could be a major breakthrough in the treatment of ALD.
"However, efforts to develop second-
and third-generation CB1R antagonists must overcome the complications caused by
the first generation of CB1R antagonists, which were able to penetrate the
blood-brain barrier and produced critical psychiatric side effects."
and
"However, pharmacological
applications of the endocannabinoid system for the treatment of ALD have not
been successful because of psychoactive side effects, despite some beneficial
effects."
Meanwhile findings continue to
demonstrate the relative uselessness in many pathways of legally-available CBD
products and point towards whole-plant effectiveness due to the so-called
entourage effect.
University of Michigan researchers
with the company Gb Sciences Inc. evaluated the effect of selected terpenes and
cannabinoids on human primary leukocytes.
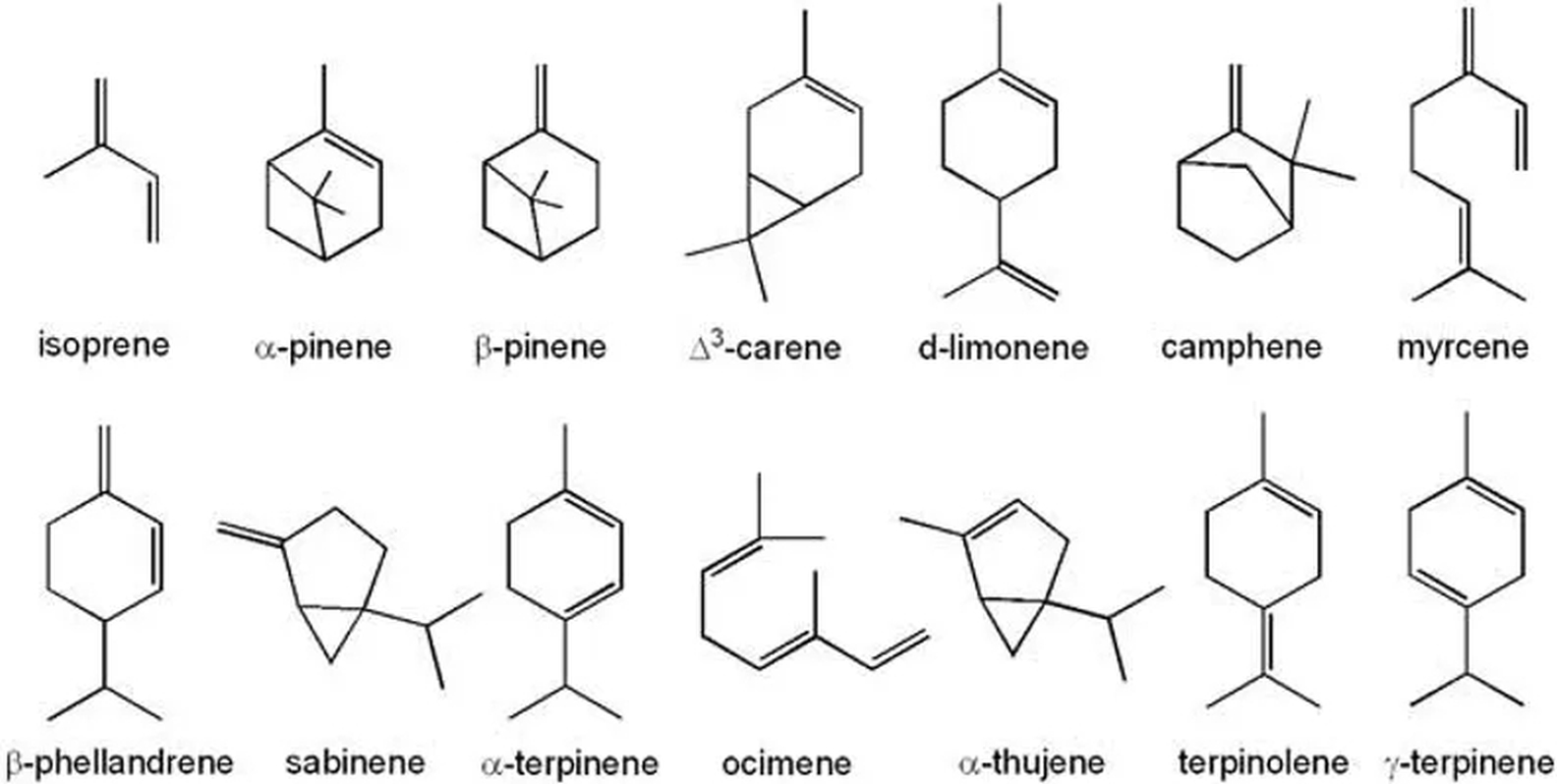
The terpenes evaluated included
α-pinene, trans-nerolidol, D-limonene, linalool and phytol. The three immune
cell types were chosen based on their important roles in modulating the
inflammatory cascade.
The study found that the most
efficient cannabinoid was THC, followed by CBDV (Cannabidivarin), CBG
(Cannabigerol), CBC (Cannabichromene), CBN (Cannabinol) and finally, CBD.
The terpene α-Pinene showed the
greatest immune modulating activity from the group followed by linalool, phytol
and trans-nerolidol. Limonene had no effect which was attributed to some
terpenes being highly selective or targeting a single cell type.
Peripheral Blood Mononuclear Cells
are any peripheral blood cell having a round nucleus, and include lymphocytes (T
cells, B cells, and NK cells), monocytes, and dendritic cells. In humans, the
frequencies of these populations vary across individuals, but typically,
lymphocytes are in the range of 70–90 %, monocytes from 10 to 20 %, while
dendritic cells are rare, accounting for only 1–2 %.
"Human PBMC were pretreated with each
compound, individually, at concentrations extending from 0.001 to 10 μM and then
stimulated with CpG (plasmacytoid dendritic cell), LPS (monocytes), or
anti-CD3/CD28 (T cells). Proliferation, activation marker expression, cytokine
production and phagocytosis, were quantified. Of the 21 responses assayed for
each compound, cannabinoids showed the greatest immune modulating activity
compared to their vehicle control. Delta-9-tetrahydrocannabinol possessed the
greatest activity affecting 11 immune parameters followed by cannabidivarin,
cannabigerol, cannabichromene, cannabinol and cannabidiol. α-Pinene showed the
greatest immune modulating activity from the selected group of terpenes,
followed by linalool, phytol, trans-nerolidol. Limonene had no effect on any of
the parameters tested. Overall, these studies suggest that selected
cannabis-derived terpenes displayed minimal immunological activity, while
cannabinoids exhibited a broader range of activity."
https://www.sciencedirect.com/science/article/abs/pii/S0278691522006561
[1726]
Some consider the effect to be
additive, rather than synergistic or multiplicative in nature. Discussing D9-THC
and terpene interactions in 2021, Liktor-Busa et al at the Department of
Pharmacology of the University of Arizona summarise:
"These studies suggest that although
terpenes may have significant antinociceptive properties (discussed above), it
is likely that these properties are not modulated through direct interactions at
cannabinoid receptors, nor does it appear they will modify antinociception
induced by cannabinoids such as D9 -THC. However, these studies are limited and
do not rule out an interaction definitively."
As for CBD, evidence is "limited":
"An in vivo study observing the
difference between CBD, D9 -THC, or a C. sativa high-CBD extract (containing
other phytocompounds) demonstrated that the antinociceptive properties of the
CBD extract were greater than CBD or D9 -THC alone in a chronic constriction
injury model of neuropathic pain (Comelli et al., 2008). Furthermore, combining
pure CBD and pure D9 -THC in a similar ratio to the high-CBD extract could not
recapitulate the greater effect of the extract, suggesting other noncannabinoid
contributions. They also state that although a single dose of CBD could not
alleviate the neuropathic pain, a single dose of the CBD extract could reduce
thermal hyperalgesia comparable to D9 -THC, but data were not provided. The
antinociceptive effects of the CBD extract could be blocked with a TRPV1
antagonist but not a CB1 or CB2 antagonist."
https://pharmrev.aspetjournals.org/content/pharmrev/73/4/1269.full.pdf
[2937]
Tomko et al at Dalhousie University
in Halifax, Canada found "Anti-cancer properties of cannflavin A and potential
synergistic efects with gemcitabine, cisplatin, and cannabinoids in bladder
cancer" (2022):
"Cell viability of bladder cancer
cell lines was affected in a concentration-dependent fashion in response to
cannflavin A, and its combination with gemcitabine or cisplatin induced
differential responses-from antagonistic to additive-and synergism was also
observed in some instances, depending on the concentrations and drugs used.
Cannflavin A also activated apoptosis via caspase 3 cleavage and was able to
reduce invasion by 50%. Interestingly, cannflavin A displayed synergistic
properties with other cannabinoids like Δ9-tetrahydrocannabinol, cannabidiol,
cannabichromene, and cannabivarin in the bladder cancer cell lines."
https://jcannabisresearch.biomedcentral.com/counter/pdf/10.1186/s42238-022-00151-y.pdf
[2941] and see [3007]
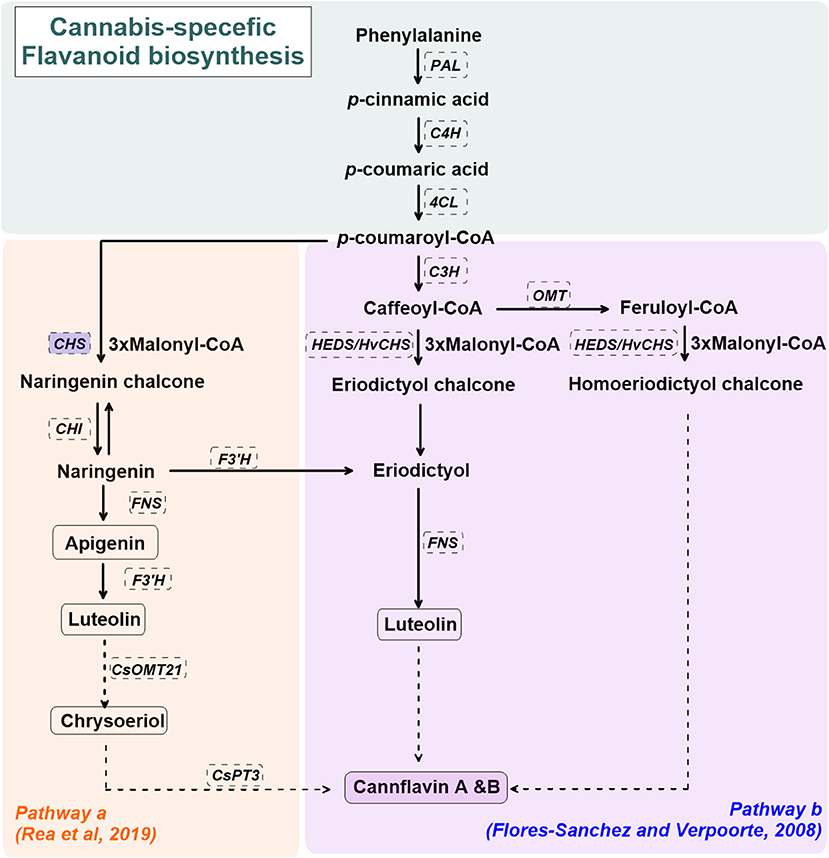
Cannabis components such as the
cannflavins may be manipulable using different artificial light and cultivars:
"Increased solar UV radiation results
in higher CBDA, terpene, and cannaflavin [sic] content in the hemp variety
“Kompolti” (Giupponi et al., 2020). Notably, UV radiation sources used in both
studies had relatively broad spectra, compared to electrical UV radiation
sources, such UV-discharge lamps and light-emitting diodes (LEDs). It is unknown
if there is was an interactive effect between UV-A (315–380 nm) and UV-B
radiation, as a high percentage of UV-A radiation was present in both the UV-B
and control light treatments (Mirecki and Teramura, 1984; Lydon et al., 1987;
Giupponi et al., 2020). A subsequent study examined the impact of UV-A radiation
on cannabinoid accumulation, and reported increased cannabinoid levels other
than Δ9-THC (Magagnini et al., 2018). Low percentages of UV-A radiation (2%)
from full-spectrum LED arrays induced an increase of several cannabinoids,
including CBD, CBG, Δ9-THC, and tetrahydrocannabivarin (THCV), compared to a
high pressure sodium (HPS) lamp that contained 1% of UV-A radiation (Magagnini
et al., 2018)."
Yet by 2021, according to
"Cannabinoids and Terpenes: How Production of Photo-Protectants Can Be
Manipulated to Enhance Cannabis sativa L. Phytochemistry" the pathway(s) by
which cannflavins are produced in the plant was still a matter of debate.
Brousseau et al also offer a
"simplified overview" of the effect of spectra on synthesis of the cannabis
components:
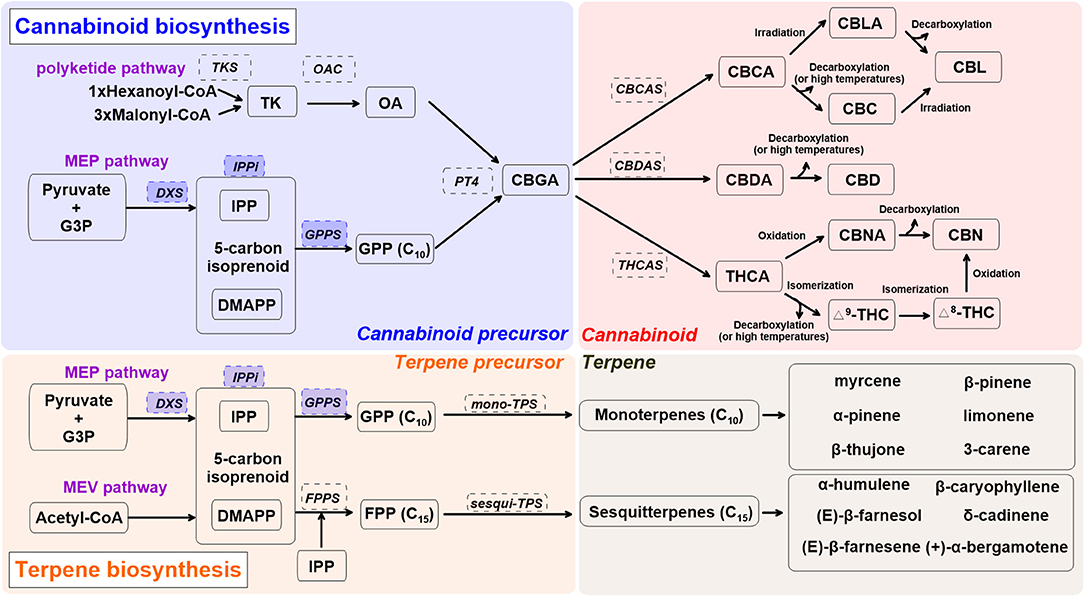
"FIGURE 1. A simplified overview of
cannabinoid and terpene biosynthesis pathways in cannabis (Cannabis sativa L.),
derived from recent reviews (Hazekamp, 2007; Degenhardt et al., 2017;
Sirikantaramas and Taura, 2017; Jin et al., 2019). Enzymes are in dashed line
box. Enzymes in shaded blue boxes are upregulated by UV radiation and blue light
in Lamiaceae [a family that includes mint. basil, oregano and lavender].
Cannabis precursor (shade blue): CBDA, cannabidiolic acid; DMAPP, dimethylallyl
pyrophosphate; G3P, glyceraldehyde 3-phosphate; GPP, geranyl pyrophosphate;
GPPS, geranyl pyrophosphate synthase; MEP, methylerythritol phosphate; PT4,
geranylpyrophosphate: olivetolate geranyltransferase 4; IPP, isopentenyl
diphosphate; IPPi, isopentenyl-diphosphate delta-isomerase; OA, olivetolic acid;
OAC, olivetolic acid cyclase; TK, tetraketide; TKS, tetraketide synthase.
Cannabinoid (shade red): CBC, cannabichromene; CBCA, cannabichromentic acid;
CBCAS, cannabichromentic acid synthase; CBDAS, cannabidiolic acid synthase; CBD,
cannabidiol; CBG, cannabigerol; CBGA, cannabigerolic acid; CBL, cannabicyclol;
CBLA, cannabicyclolic acid; CBN, cannabinol; CBNA: cannabinolic acid; Δ8-THC,
Δ8-tetrahydrocannabinol; Δ9-THC (or THC), Δ9-tetrahydrocannabinol; THCA,
tetrahydrocannabinolic acid. Terpene precursor (shade orange): FPP, farnesyl
diphosphate; FPPS, farnesyl diphosphate synthase; MEV, mevalonate; TPS, terpene
synthase."
https://www.frontiersin.org/articles/10.3389/fpls.2021.620021/full [3038]
de Christo Scherer et al found a
dose-dependent effect in the "Wound healing activity of terpinolene and
α-phellandrene by attenuating inflammation and oxidative stress in vitro"
(2019). As they explain:
"Terpenoids represent the oldest and
most diverse class of secondary metabolites formed from five-carbon isoprene
units called isoprenoids. They represent a highly diversified group of naturally
occurring organic compounds, and more than 30,000 different natural terpene
metabolites were identified. In plants, terpenoids have a multitude of
ecological and physiological functions. They chemically defend against insects
and environmental stress and are involved in the repair mechanism of wounds and
injuries."
and
"In summary, the results of the
present study showed that terpinolene and α-phellandrene, which share similar
chemical characteristics, exhibited similar wound healing properties. Using
cell-based assays, both compounds effectively stimulated proliferation and
migration of fibroblasts, protected macrophages against cellular oxidative
damage, and suppressed the production of pro-inflammatory cytokines (IL-6 and
TNF-α) and NF-κB activity."
https://www.sciencedirect.com/science/article/abs/pii/S0965206X18301311 [2494]
According to Susanto et al (2024)
phellandrene, found in several herbs, has a synergestic antiproliferative effect
on cancer cells with 5-fluorouracil. HT-29 is a human colorectal adenocarcinoma
cell line with epithelial morphology, sensitive to 5-FU.
"The combination of 5-FU and α-PA had
a synergistic inhibitory effect on cell viability, as determined by assessing
the combination index value. Bax protein expression levels were higher in the
50, 100 or 250 µM α-PA combined with 5-FU groups compared with those in the 5-FU
alone group (P<0.05). By contrast, Bcl-2 protein expression levels and
mitochondrial membrane potential (MMP, ΔΨm) were lower in the 100 or 250 µM α-PA
combined with 5-FU groups than those in the 5-FU alone group (P<0.05). In
addition, hexokinase-2 (HK-2) protein expression levels were lower in the 50,
100 or 250 µM α-PA combined with 5-FU groups than those in the 5-FU alone group
(P<0.05). Compared with 5-FU alone, after HT-29 cells were treated with 50, 100
or 250 µM α-PA combined with 5-FU, the mRNA expression levels of
extrinsic-induced apoptotic molecules, including caspase-8 and Bid, were higher
(P<0.05). Treatment with 50, 100 or 250 µM α-PA combined with 5-FU also
increased the mRNA expression levels of cytochrome c, caspase-9 and caspase-3,
regulating intrinsic apoptosis (P<0.05). These results showed that α-PA and 5-FU
had a synergistic effect on reducing the viability of human colon cancer HT-29
cells by inducing extrinsic and intrinsic apoptosis pathways."
https://pmc.ncbi.nlm.nih.gov/articles/PMC10940876/ [3649]
Ten years earlier, Slovenia's
alcohol-worshippers could have learned from Hsieh et al (2014) about "Induction
of necrosis in human liver tumor cells by α-phellandrene":
"Human liver tumor (J5) cells were
incubated with α-PA and analyzed for cell cycle distribution, expression of Bax,
Bcl-2, poly (ADP-ribose) polymerase (PARP) protein, and caspase-3 activity of J5
cells, and levels of nitric oxide (NO) production, lactate dehydrogenase (LDH)
leakage, and ATP depletion were also analyzed in this study. Results found that
α-PA significantly (P < 0.05) decreased the cell viability of J5 cells after
24-h treatment. The cell cycle distribution, Bax, Bcl-2, PARP protein levels,
and caspase-3 activity of J5 cells did not change for 24 h after treatment with
30 μM α-PA. Reactive oxygen species levels significantly increased,
mitochondrial membrane potential levels significantly decreased when J5 cells
were treated with 30 μM α-PA for 24 h (P < 0.05). Thirty μM α-PA significantly
(P < 0.05) increased the necrotic cell number, NO production, LDH leakage, and
ATP depletion after 24 h of incubation. These results suggest that α-PA induced
J5 cell necrosis but not apoptosis, and α-PA-induced necrosis possibly involved
ATP depletion."
https://pubmed.ncbi.nlm.nih.gov/25077527/ [3650]
Aydin et al (2013) investigated
"Anticancer and antioxidant properties of terpinolene in rat brain cells":
"Terpinolene (TPO) is a natural
monoterpene present in essential oils of many aromatic plant species. Although
various biological activities of TPO have been demonstrated, its neurotoxicity
has never been explored. In this in vitro study we investigated TPO's
antiproliferative and/or cytotoxic properties using the
3-(4,5-dimethylthiazol-2-yl)-2,5 diphenyltetrazolium bromide (MTT) test,
genotoxic damage potential using the single-cell gel electrophoresis (SCGE), and
oxidative effects through total antioxidant capacity (TAC) and total oxidative
stress (TOS) in cultured primary rat neurons and N2a neuroblastoma cells.
Dose-dependent effects of TPO (at 10 mg L(-1), 25 mg L(-1), 50 mg L(-1), 100 mg
L(-1), 200 mg L(-1), and 400 mg L(-1)) were tested in both cell types.
Significant (P<0.05) decrease in cell proliferation were observed in cultured
primary rat neurons starting with the dose of 100 mg L(-1) and in N2a
neuroblastoma cells starting with 50 mg L(-1). TPO was not genotoxic in either
cell type. In addition, TPO treatment at 10 mg L(-1), 25 mg L(-1), and 50 mg
L(-1) increased TAC in primary rat neurons, but not in N2a cells. However, at
concentrations above 50 mg L(-1) it increased TOS in both cell types. Our
findings clearly demonstrate that TPO is a potent antiproliferative agent for
brain tumour cells and may have potential as an anticancer agent, which needs to
be further studied."
As for genotoxicity:
"In vitro exposure to TPO of either
cell type did not result in comet formation, regardless of the dose, indicating
the non-genotoxic nature of TPO (Figure 2)."
For total antioxidant capacity (in
Trolox Equivalent / mmol L-1)...
"TPO at the concentrations of 100 mg
L-1 and 200 mg L-1 did not affect TAC in primary rat neuron cells, increased it
signifi cantly at the concentrations of (10, 25, and 50) mg L-1, and decreased
it signifi cantly at the highest concentration (400 mg L-1) compared to control
(Table 1). Similarly, in N2a neuroblastoma cells TPO (at 10 mg L-1 and 25 mg
L-1) did not change TAC levels, but decreased them signifi cantly at ((50, 100,
200, and 400) mg L-1, compared to control."
https://sciendo.com/pdf/10.2478/10004-1254-64-2013-2365 [3562]
Reminding us that "Cannabis sativa has been
utilized for medical purposes for thousands of years. It continues to be
recognized as a plant with an extensive variety of medicinal and nutraceutical
uses today," a paper on the discovery of "New Cannabinoids and Chlorin-Type
Metabolites from the Flowers of Cannabis sativa L.: A Study on Their
Neuroblastoma Activity" by Nguyen et al from Korea reported in April 2025:
"Eleven compounds were isolated from the flowers of C. sativa, including two new
compounds, namely cannabielsoxa (1), 132-hydroxypheophorbide c ethyl ester (2),
and six known cannabinoids (6–11), together with the first isolation of
chlorin-type compounds: pyropheophorbide A (3), 132-hydroxypheophorbide b ethyl
ester (4), and ligulariaphytin A (5) from this plant. The results also
demonstrated that cannabinoid compounds had stronger inhibitory effects on
neuroblastoma cells than chlorin-type compounds. Conclusions: The evaluation of
the biological activities of compounds showed that compounds 4–10 could be
considered as the potential compounds for antitumor effects against
neuroblastomas. This is also highlighted by using docking analysis.
Additionally, the results of this study also suggest that these compounds have
the potential to be developed into antineuroblastoma products."
https://www.mdpi.com/1424-8247/18/4/521 [4978]
Sztolsztener et al (2023) describe
the "Concentration-Dependent Attenuation of Pro-Fibrotic Responses after
Cannabigerol Exposure in Primary Rat Hepatocytes Cultured in Palmitate and
Fructose Media":
"Hepatic fibrosis is a consequence of
liver injuries, in which the overproduction and progressive accumulation of
extracellular matrix (ECM) components with the simultaneous failure of matrix
turnover mechanisms are observed. The aim of this study was to investigate the
concentration dependent influence of cannabigerol (CBG, Cannabis sativa L.
component) on ECM composition with respect to transforming growth factor beta 1
(TGF-β1) changes in primary hepatocytes with fibrotic changes induced by
palmitate and fructose media. Cells were isolated from male Wistar rats’ livers
in accordance with the two-step collagenase perfusion technique. This was
followed by hepatocytes incubation with the presence or absence of palmitate
with fructose and/or cannabigerol (at concentrations of 1, 5, 10, 15, 25, 30 µM)
for 48 h. The expression of ECM mRNA genes and proteins was determined using PCR
and Western blot, respectively, whereas media ECM level was evaluated using
ELISA. Our results indicated that selected low concentrations of CBG caused a
reduction in TGF-β1 mRNA expression and secretion into media. Hepatocyte
exposure to cannabigerol at low concentrations attenuated collagen 1 and 3
deposition. The protein and/or mRNA expressions and MMP-2 and MMP-9 secretion
were augmented using CBG. Considering the mentioned results, low concentrations
of cannabigerol treatment might expedite fibrosis regression and promote
regeneration."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10526512/pdf/cells-12-02243.pdf
[4045]
A reduction in cell viability in human
pancreatic ductal adenocarcinoma (PDAC) cell lines was assisted by a
"synergistic effect of CBG in combination with gemcitabine (GEM) and paclitaxel
(PTX)" [3979]
Sativa terpenes on their own "mimic
the effects of cannabinoids, including a reduction in pain sensation," notes a
statement from the University of Arizona Health Sciences.
But when terpenes were combined with
cannabinoids, "the pain-relieving effects were amplified without an increase in
negative side effects," investigators report.
https://www.nature.com/articles/s41598-021-87740-8 [500]
Smith et al examined the chemical
reality of THC-dominant, CBD-dominant and balanced THC:CBD strains and found the
present labels inadequate. 2022's "The phytochemical diversity of commercial
Cannabis in the United States" found that CBD-dominant and THC:CBD balanced
products "displayed myrcene-dominant terpene profiles compared to THC-dominant
samples."
"Mapping the chemical diversity of
the Cannabis-derived products consumed by millions of people has important
implications for consumer health and safety, such as identifying the number of
chemically distinct types of Cannabis being consumed in legal markets. This may
be consequential if distinct chemotypes are later determined to cause reliably
different effects."
The researchers analyzed 89,923
different samples of loose-leaf cannabis from six certified testing laboratories
in the U.S. states.
"84.5 percent of CBD-dominant samples
had total THC levels above 0.3 percent, the threshold used to legally define
hemp in the U.S.," noted the researchers. "This indicates that a substantial
fraction of CBD-dominant cannabis would not meet the legal definition of hemp in
the U.S.," indicating a collision between the biochemical reality of this plant
species and the regulatory framework wrapped around it in the United States.
The most common terpenes present in
the flower samples were beta-caryophyllene (BCP), limonene, and myrcene (the
most common terpene in cannabis, according to other studies). "In most cases,
individual terpenes were rarely present at more than 0.5 percent weight."
and the research found that
THC-dominant cannabis products (Type I) "displayed significantly higher levels
of [terpene] diversity than both balanced THC:CBD [Type II] and CBD-dominant
products [Type III]."
The study found that the labels of
indica, sativa, and hybrid did not correspond well to the terpene profiles of
the samples. "It is likely that a sample with the label 'indica' will have an
indistinguishable terpene composition as samples labelled 'sativa' or 'hybrid.'"
The scientists determined that a
simple product labeling system "in which THC-dominant samples are labelled by
their dominant terpene" would better serve both the industry and consumers and
be "better at discriminating samples than the industry-standard labelling
system" of indica, sativa, and hybrid.
The study found "a large amount of
variability in mean consistency scores across all 'strain names.'" Sometimes,
the chemical makeup of a strain featured relatively strong consistency across
the data set. For example, 96 percent of flower samples labeled to be the strain
Purple Punch feature strong levels of beta-caryophyllene and limonene, while
only 62.5 percent of products labeled Tangie fell into a single cluster.
The study identified three cluster
groups that each are dominated by a different terpene pair.
Cluster I: Relatively high levels of
beta-caryophyllene and limonene
Cluster II: Relatively high levels of
myrcene and pinene
Cluster III: Relatively high levels
of myrcene and terpinolene
"Samples across these clusters
display similar total THC distributions, while Cluster III is associated with
modestly higher CBG levels," summarized the study's authors.
The scientists concluded that their
study results "provide new possibilities for systematically categorizing
commercial cannabis [products] based on chemistry, the design of preclinical and
clinical research experiments, and the regulation of commercial cannabis
marketing."
"The general approach we have used in
this study can serve as a basic guide for cannabis product segmentation and
classification rooted in product chemistry," they wrote. "Consumer-facing
labelling systems should be grounded in such an approach so that consumers can
be guided to products with reliably different sensory and psychoactive
attributes."
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0267498
[2007]
I predict that Slovenian
fun-reduction experts will want, for the first time ever, a ban on emotive,
hyperbolic advertising, with only government-approved strain names like
"Bureaucrat Grey" and "Reverend Brown" allowed.
For some researchers, the major
cannabinoids are relatively uninteresting:
"In this study we provide the first
comprehensive overview of the effects of whole-plant Cannabis extracts and
various pure cannabinoids on store-operated calcium (Ca2+) entry (SOCE) in
several different immune cell lines. Store-operated Ca2+ entry is one of the
most significant Ca2+ influx mechanisms in immune cells, and it is critical for
the activation of T lymphocytes, leading to the release of proinflammatory
cytokines and mediating inflammation and T cell proliferation, key mechanisms
for maintaining chronic pain. While the two major cannabinoids cannabidiol and
trans-Δ9-tetrahydrocannabinol were largely ineffective in inhibiting SOCE, we
report for the first time that several minor cannabinoids, mainly the carboxylic
acid derivatives and particularly cannabigerolic acid, demonstrated high potency
against SOCE by blocking calcium release-activated calcium currents. Moreover,
we show that this inhibition of SOCE resulted in a decrease of nuclear factor of
activated T-cells [NFAT] activation and Interleukin 2 production in human T
lymphocytes. Taken together, these results indicate that cannabinoid-mediated
inhibition of a proinflammatory target such as SOCE may at least partially
explain the anti-inflammatory and analgesic effects of Cannabis."
You should know
"The release of proinflammatory
mediators is regulated by calcium-dependent signaling mechanisms that activate
several transcription factor pathways, including NFAT, nuclear factor kappa B
(NF-KB), and cAMP response element-binding protein."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9334010/ [2005]
Musetti et al, discussing the
anti-atherosclerotic effects of three cannabis extracts, point out that:
"...the effect of the extracts was
greater than the addition of the inhibitory effect of the individual cannabinoid
components. This synergy or more than additive effect could be explained by the
entourage effect. The term was first coined by Ben-Shabat et al. to explain that
non-active metabolites potentiated the effect of the endocannabinoid
2-arachidonoylglycerol. Individual components could exhibit additive effects,
their combined impact is simply the sum of their individual effects;
antagonistic interactions, or synergistic interactions when compounds produce an
effect surpassing the sum of their individual contributions.
Cannabinoid-cannabinoid interactions, cannabinoid-terpene, and terpene-terpene
interactions could account for intra or inter entourage effects. Our observation
that the extracts as a whole exhibit stronger inhibition than the sum of the
effect of the component cannabinoids supports either an entourage effect or the
additive effect of a low-abundance component with potent bioactivity.
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0310777
[3817]
Despite insisting on looking only at
CBD a review of 246 studies on lung cell cancer apoptosis reported, in 2022:
"The most common cell line used in
all of the studies was A549; however, some studies included other cell lines,
including H460 and H358. We concluded that CBD has direct antineoplastic effects
on lung cancer cells by various mechanisms mediated by cannabinoid receptors or
independent of them."
https://pubmed.ncbi.nlm.nih.gov/36437760/ [1756]
"Humulene Inhibits Acute Gastric
Mucosal Injury by Enhancing Mucosal Integrity" by Yeo et al (2021) looks at the
cannabis terpene humulene.
"In this study, a HCl/ethanol-induced
gastritis or pylorus ligation-induced ulcer rat model was utilized to reveal the
protective effect of α-humulene and its related mechanism for mucus secretion,
gastric acid secretion, oxidant/antioxidant balance, and mucosal stabilizing
factors such as MUC5AC and MUC6 in vivo. In addition, we used the phorbol
12-myristate 13-acetate (PMA)-induced human mast cell-1 (HMC-1) model. PMA, a
potent activator of protein kinase C, stimulates HMC-1 cells to exhibit
characteristis of tissue mast cells including degranulation, surface antigen
profile, and cytokine activation pathways. Thus, we examined the inhibitory
effect of α-humulene and its underlying molecular mechanism of histamine
release, oxidative stress, and NF-κB-mediated inflammatory responses in the
HMC-1 cell line stimulated with PMA."
finding that
"α-Humulene Attenuates Mucosal
Lesions in an HCl/Ethanol-Induced Gastritis Model"
and
"α-Humulene Increases mRNA Expression
Levels of Mucus-Stabilizing Factors in
HCl-Ethanol-Injured Stomach Tissues"
yet
"the protective action of α-humulene
against HCl/ethanol-induced gastric injury was not driven by direct
neutralization."
but
"α-Humulene Inhibits Histamine
Release in HMC-1 Cells through Ca2+ and Cyclic Adenosine Monophosphate"
plus
"α-Humulene Inhibits
Inflammation-Related Factors in PMA-Stimulated HMC-1 Cells"
and
"Under stress conditions such as
alcohol abuse, the level of histamine is elevated, which increases acid
production, thus inducing gastritis. Therefore, we investigated the inhibitory
effect of α-humulene on histamine release using HMC-1 cells. When stimulated
with compound 48/80 or PMA, HMC-1 cells release histamine. Here, we showed that
α-humulene significantly decreased histamine secretion without cellular
toxicity. Previous studies have shown that both intracellular calcium and cAMP
act as important modulators during the degranulation of HMC-1 cells. When mast
cells are stimulated, calcium channels rapidly open at the membrane, and a large
amount of calcium enters the cytoplasm. Moreover, activated phospholipase C
converts phosphatidylinositol 4,5-bisphosphate (PIP2) to inositol
1,4,5-trisphosphate (IP3), which binds to the IP3-gated calcium channel of the
mast cell endoplasmic reticulum (ER). Then, a large amount of calcium stored in
the ER is released into the cytoplasm. To investigate the underlying molecular
mechanism of the antihistamine effect of α-humulene, the following experiment
was conducted. First, we examined the changes in calcium influx using the
fluorescent dye, Fluro-2/AM. Compared to compound 48/80-treated cells,
α-humulenetreated cells showed lower levels of intracellular calcium. Next, we
investigated the changes in cAMP, because intracellular cAMP increases to
inhibit the release of mediators in mast cell. Similar to curcumin (positive
control), α-humulene increased intracellular cAMP levels, which resulted in the
inhibition of histamine release. Taken together, α-humulene inhibits histamine
secretion by regulating intracellular calcium and cAMP concentrations without
any cytotoxicity."
https://www.mdpi.com/2076-3921/10/5/761/pdf?version=1620732119 [1932]
In "Terpenes from Cannabis sativa
Induce Antinociception in Mouse Chronic Neuropathic Pain via Activation of
Spinal Cord Adenosine A2A Receptors" by Schwarz et al (2024) five cannabis
terpenes were tested on pain in mice using a Chemotherapy-Induced Peripheral
Neuropathy, and lipopolysaccharide-induced Acute Inflammatory Models:
"Terpenes are small hydrocarbon
compounds that impart aroma and taste to many plants, including Cannabis sativa.
A number of studies have shown that terpenes can produce pain relief in various
pain states in both humans and animals. However, these studies were
methodologically limited and few established mechanisms of action. In our
previous work, we showed that the terpenes geraniol, linalool, β-pinene,
αhumulene, and β-caryophyllene produced cannabimimetic behavioral effects via
multiple receptor targets. We thus expanded this work to explore the efficacy
and mechanism of these Cannabis terpenes in relieving chronic pain. We first
tested for antinociceptive efficacy by injecting terpenes (200 mg/kg, IP) into
male and female CD1 mice with chemotherapy-induced peripheral neuropathy (CIPN)
or lipopolysaccharide-induced inflammatory pain, finding that the terpenes
produced roughly equal efficacy to 10 mg/kg morphine or 3.2 mg/kg WIN55,212. We
further found that none of the terpenes produced reward as measured by
conditioned place preference, while low doses of terpene (100 mg/kg) combined
with morphine (3.2 mg/kg) produced enhanced antinociception vs. either alone. We
then used the adenosine A2A receptor (A2AR) selective antagonist istradefylline
(3.2 mg/kg, IP) and spinal cord-specific CRISPR knockdown of the A2AR to
identify this receptor as the mechanism for terpene antinociception in CIPN. In
vitro cAMP and binding studies and in silico modeling studies further suggested
that the terpenes act as A2AR agonists. Together these studies identify Cannabis
terpenes as potential therapeutics for chronic neuropathic pain, and identify a
receptor mechanism in the spinal cord for this activity."
In the LPS arm
"Mechanical allodynia was produced by
LPS in all mice (Figure 2A). Most terpenes (200 mg/kg, IP) produced significant
time-dependent antinociception over vehicle control; the only exception was
β-pinene, which produced a small, non-significant improvement in mechanical
threshold (Figure 2A). AUC analysis backed up this conclusion, with geraniol and
linalool both producing significant elevation in AUC over vehicle control
(Figure 2B). Much like with CIPN above, while the other terpenes had
non-significant AUC increases, the mean values were still elevated 5-7 fold over
the vehicle mean (Figure 2B). Both data types together suggest that all terpenes
except β-pinene are effective antinociceptive agents in this second, different
pathological pain type."
https://journals.lww.com/pain/fulltext/2024/11000/terpenes_from_cannabis_sativa_induce.16.aspx [3100]
"'The terpenes were tested
individually and compared with morphine. The research team found that each
terpene was successful in reducing the sensation of pain at levels near to or
above the peak effect of morphine. When the terpenes were combined with
morphine, the pain-relieving effects of all five terpene/morphine combinations
were significantly increased.
"'That was really striking to us, but
just because something relieves pain doesn’t necessarily mean it’s going to be a
good therapy,' [lead researcher John] Streicher said.
"Comparing Terpenes and Opioids
Opioids are often used to treat many
types of pain, but they can come with a host of unwanted side effects. Opioids
activate the brain’s reward system, which is what can lead to addiction, and can
cause tolerance, a condition that occurs when the body gets used to a medication
and needs increasingly larger doses to have the same effect. Opioids also can
cause respiratory depression, which can lead to death.
“'We looked at other aspects of the
terpenes, such as: Does this cause reward? Is this going to be addictive? Is it
going to make you feel awful?' Streicher said. 'What we found was yes, terpenes
do relieve pain, and they also have a pretty good side effect profile.'
"None of the terpenes had reward
liability, making them a low risk for addiction. Some of the terpenes also did
not cause aversive behaviors, which suggests they could be effective
therapeutics without producing distressing side effects.
"Finally, researchers tested
different routes of terpene administration: injection, oral dosing, and
inhalation of vaporized pure terpenes. They found that when terpenes were given
orally or inhaled, the effects were significantly reduced or absent.
"'A lot of people vape or smoke
terpenes as part of cannabis extracts that are available commercially in states
where cannabis use is legal,' Streicher said 'We were surprised to find that the
inhalation route didn’t have an impact in this study, because there are a lot of
at least anecdotal reports saying that you can get the effects of terpenes
whether taken orally or inhaled. Part of the confounding factor is that terpenes
smell quite nice and it’s hard to disguise that aroma, so people could be kind
of having the psychosomatic placebo-style effect.'"
Their future aims to exploit this
supposedly placebo, anti-rewarding effect:
"...you could have a combination
therapy, an opioid with a high level of terpene, that could actually make the
pain relief better while blocking the addiction potential of opioids,' Streicher
said. 'That’s what we are looking at now.'"
https://scitechdaily.com/natures-painkiller-natural-molecules-found-in-cannabis-rival-morphine-in-groundbreaking-study/
[3101]
2019's "The heterogeneity and
complexity of Cannabis extracts as antitumor agents" from the University of
Haifa, Israel concluded your chances against cancer are improved with a shotgun
effect of natural cannabinoid combinations compared to single extracts. Nature
got it right again.
"Dr. Baram et al. investigated the
effect of various combinations of cannabis extracts and their effect on 12
different cancers. Results demonstrated a variable response depending upon the
cancer type and content profile of the specific cannabis extract. Of the 12
cancer varieties tested, components of THC were found to be successful in
inducing cell death. Apoptotic features and/or inhibition of proliferation were
found to be the underlying mechanism. Interestingly, two extracts consisting of
equal amounts of THC but varying levels of other cannabinoids (i.e., CBD,
Cannabigerol [CBG], THCA, etc.) had different outcomes in terms of cell death.
Such findings indicate the likelihood that the interplay of the combination of
cannabinoids may be the true determining factor of the extract's effectiveness
rather than the presence or amount of THC. Therefore, the authors recommend
whole extract cannabinoid therapy as opposed to single-agent THC formulations
that have higher anti-tumor properties."
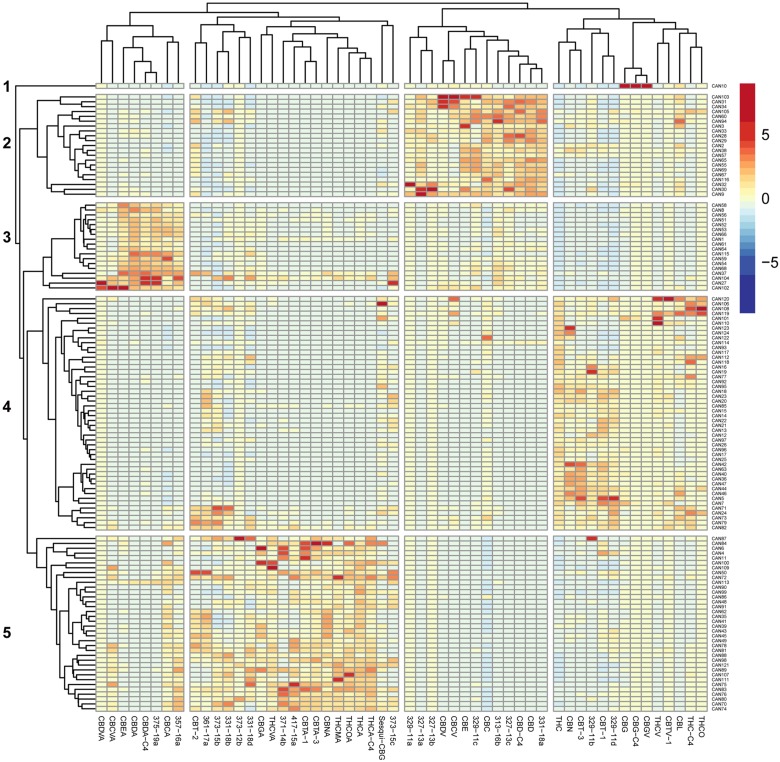
"The 124 extracts segregate into five
major clusters comprised of phytocannabinoids that associate with: (1) larger
amounts of CBG-type; (2) larger amounts of CBD-type.; (3) larger amounts of
CBDA-type; (4) larger amounts of Δ9-THC-type; (5) larger amounts of
Δ9-THCA-type."
Twelve cannabinoids were selected and
their effect on A549 lung cancer cell survival is shown in
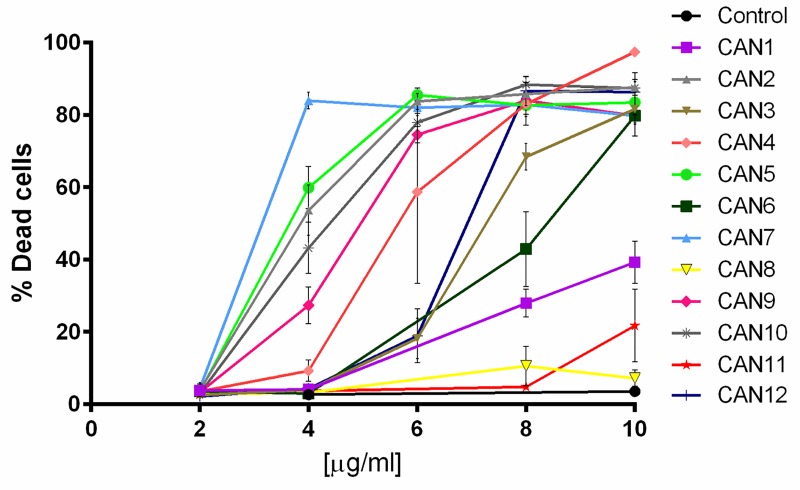
"A549 cells were treated with three
different Cannabis extracts: CAN5, a Δ9-THC-rich extract; CAN9, a CBD-rich
extract; and CAN10, a CBG-rich extract. Treatment with each of these Cannabis
extracts for 24 h led to apoptosis of A549 cells in a dose-dependent manner."
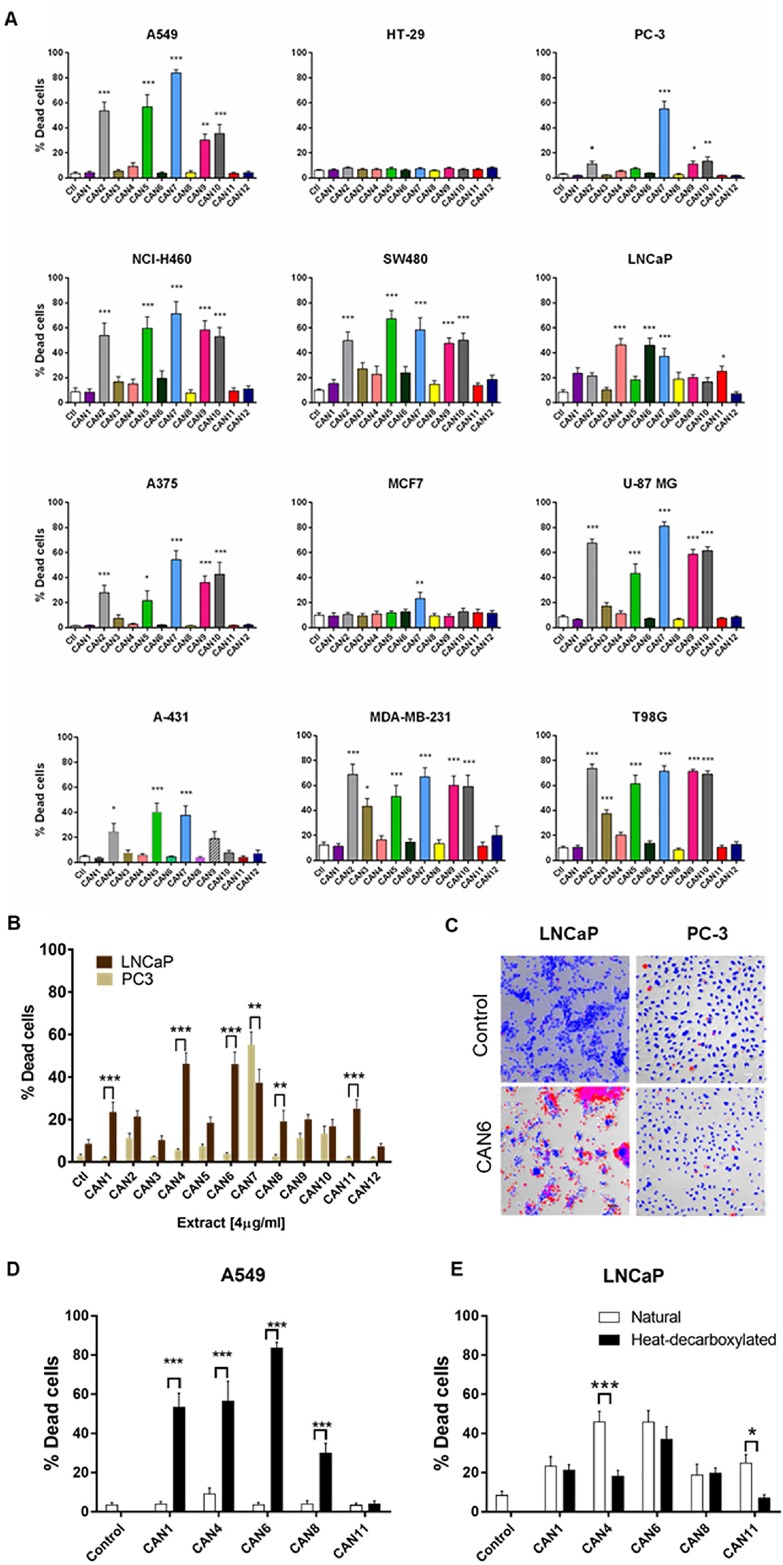
Again in A549,
"CAN5 and CAN9 extracts produced
statistically significant reductions in cell proliferation."
Both CAN2 (a CBD-type extract) and
CAN5 (high THC) were among the top scorers overall.
The colorectal adenocarcinoma HT29
cell line was the least sensitive to all the extracts studied of all the cell
lines studied, but even so, increased apoptosis was observed with all 12
extracts in HT29.
The values in Supplementary Table I
are IC50 (not LC50 as printed - the LC50 is an LD50 for substances in air) and
IC50 is measured in µg/ml. Values above 10 are lumped together as showing the
action to be relatively useless: the lower the figure the more effective the
extract.
The half maximal inhibitory
concentration (IC50) is a measure of the potency of a substance in inhibiting a
specific biological or biochemical function. IC50 is a quantitative measure that
indicates how much of a particular inhibitory substance (e.g. drug) is needed to
inhibit, in vitro, a given biological process or biological component by 50%.
The 144 cell line/extract
combinations are CAN1 to CAN12 and
A549 (lung cancer)
NCIH460 (fast growing hypertriploid
lung cancer)
PC3 (Caucasian prostate
adenocarcinoma)
LNcAP (androgen-sensitive human
prostate adenocarcinoma)
HT29 (colorectal adenocarcinoma)
SW480 (adenocarcinoma of the colon)
A431 (squamous carcinoma)
A375 (melanoma)
MDA231 (breast adenocarcinoma)
MCF7 (breast cancer)
U87MG (glioblastoma)
T98G (glioblastoma)
"CAN7, a Δ9-THC-rich extract, was the
least discriminatory of the twelve extracts, as it significantly reduced the
survival of both cancerous and non-cancer lung epithelial cell lines."
By my own count, pure THC beat
extracts in 31 (19.9%) out of 156 pairings (Supplementary Table 1). This of
course means that entourage effects were more proapoptotic in 125 (80.1%) of the
cases. At the same time this doesn't mean THC did not contribute in the 19.9%.
The results are summarised in
graphical form in Figure 3:
In their discussion the authors refer
to some other reports of synergistic effects between THC and CBD and consider
that
"...beyond the major
phytocannabinoids present in these extracts, other Cannabis extract components
may play a role in either increasing phytocannabinoid potency or
phytocannabinoid affinity to respective cannabimimetic receptors, and therefore
are important for the anti-tumor effects produced by Cannabis."
They are quite definite that
"Although we observed that specific
Δ9-THC-rich Cannabis extracts were very potent in inducing cell death, their
cytotoxic effects cannot be explained solely by the amount of Δ9-THC in the
extracts. Nor can the potencies of these extracts be explained by other
individual phytocannabinoids detected in them." (Supplementary Table 2)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6609248/ [1164]
Rios et al (2025)
"...investigated the effect of combining a terpene, Beta-Caryophyllene (BCP),
and cannabidiol (CBD) on neuropathic pain and associated depression. We employed
a chronic constriction injury (CCI) neuropathic pain model and a series of
behavioral tests to evaluate how oral administration of this combination
influences neuropathic pain and depression-like behaviors in mice. We employed
immunohistochemistry and proteomics approaches to explore the mechanism.
Results: The analgesic effect of combining CBD and BCP is synergistic in
neuropathic pain and also shows an antidepressant effect. Additionally, we found
that this combination decreases neuroinflammation associated with CCI and
affects specific genes involved in the inflammation."
https://www.mdpi.com/2227-9059/13/12/3103 [5802]
"Does cannabidiol make cannabis
safer? A randomised, double-blind, cross-over trial of cannabis with four
different CBD:THC ratios" examined various cognitive and physiological markers:
"This study aimed to determine if
increasing the CBD content of cannabis can reduce its harmful effects. Forty-six
healthy, infrequent cannabis users participated in a double-blind,
within-subject, randomised trial of cannabis preparations varying in CBD
content. There was an initial baseline visit followed by four drug
administration visits, in which participants inhaled vaporised cannabis
containing 10 mg THC and either 0 mg (0:1 CBD:THC), 10 mg (1:1), 20 mg (2:1), or
30 mg (3:1) CBD, in a randomised, counter-balanced order. The primary outcome
was change in delayed verbal recall on the Hopkins Verbal Learning Task.
Secondary outcomes included change in severity of psychotic symptoms (e.g.,
Positive and Negative Syndrome Scale [PANSS] positive subscale), plus further
cognitive, subjective, pleasurable, pharmacological and physiological effects.
Serial plasma concentrations of THC and CBD were measured. THC (0:1) was
associated with impaired delayed verbal recall (t(45) = 3.399, d = 0.50, p =
0.001) and induced positive psychotic symptoms on the PANSS (t(45) = −4.709, d =
0.69, p = 2.41 × 10–5). These effects were not significantly modulated by any
dose of CBD. Furthermore, there was no evidence of CBD modulating the effects of
THC on other cognitive, psychotic, subjective, pleasurable, and physiological
measures. There was a dose-response relationship between CBD dose and plasma CBD
concentration, with no effect on plasma THC concentrations. At CBD:THC ratios
most common in medicinal and recreational cannabis products, we found no
evidence that CBD protects against the acute adverse effects of cannabis. This
should be considered in health policy and safety decisions about medicinal and
recreational cannabis."
and
"There were no significant
differences in either peak plasma THC, OH-THC or COOH-THC, or their respective
AUCs [areas under the curve] between the CBD:THC ratios (p > 0.008, Fig. 3A,
Appendix pp6–12). In contrast, there was a significant, dose-dependent increase
in peak plasma CBD, and in plasma CBD AUC, as CBD:THC ratio increased (p <
0.001, Fig. 3B, Appendix pp6–12). Peak plasma 7-OH-CBD was higher for the 3:1
ratio compared to 0:1 (EMM [estimated marginal mean] difference = 2.686, 95%CI:
1.888, 3.483, p = 1.25 × 10−9) and 1:1 (EMM difference = 2.206, 95% CI: 1.551,
2.861, p = 0.002), with AUC higher for 2:1 compared to 0:1 (EMM difference =
4.676, 95% CI: 3.287, 6.064, p = 0.003) and for 3:1 compared to 0:1 EMM
difference = 8.898, 95%CI: 6.256, 11.540, p = 1.71 × 10−9) and 1:1 (EMM
difference = 6.843, 95% CI: 4.811, 8.875, p = 3.57 × 10−6). Logarithmic
concentrations of THC and CBD over time, with intercept and slope across ratios
are presented in Appendix pp13–14."
CBD and coughing...
"There was evidence of greater
CBD:THC ratios increasing inhalation time and coughing in a dose responsive
manner (Appendix pp46–50). Greater inhalation time was correlated with lower
peak and AUC concentrations of cannabinoids at higher CBD:THC ratios."
and as for the pleasure
"All CBD:THC ratios increased scores
for both chocolate and music compared to baseline, but there were no significant
differences between the CBD:THC ratios (p > 0.008, Appendix pp43–45)."
https://www.nature.com/articles/s41386-022-01478-z [1876]
In another study Preet et al (2007)
demonstrated that two different lung cancer cell lines as well as patient lung
tumor samples express CB1 and CB2, and that non-toxic doses of THC inhibited
growth and spread in the cell lines. “When the cells are pretreated with THC,
they have less EGFR stimulated invasion as measured by various in-vitro assays,”
Preet said.
"In this study we characterized the
effects of THC on the EGF-induced growth and metastasis of human non-small cell
lung cancer using the cell lines A549 and SW-1573 as in vitro models. We found
that these cells express the cannabinoid receptors CB(1) and CB(2), known
targets for THC action, and that THC inhibited EGF-induced growth, chemotaxis
and chemoinvasion. Moreover, signaling studies indicated that THC may act by
inhibiting the EGF-induced phosphorylation of ERK1/2, JNK1/2 and AKT. THC also
induced the phosphorylation of focal adhesion kinase at tyrosine 397.
Additionally, in in vivo studies in severe combined immunodeficient mice, there
was significant inhibition of the subcutaneous tumor growth and lung metastasis
of A549 cells in THC-treated animals as compared to vehicle-treated controls.
Tumor samples from THC-treated animals revealed antiproliferative and
antiangiogenic effects of THC."
https://www.researchgate.net/publication/6217199_D9-Tetrahydrocannabinol_inhibits_epithelial_growth_factor-induced_lung_cancer_cell_migration_in_vitro_as_well_as_its_growth_and_metastasis_in_vivo/link/0deec525c152d7388c000000/download
[1734]
In 2010 Preet et al confirmed:
"Reduced proliferation and
vascularization, along with increased apoptosis, were observed in tumors
obtained from animals treated with JWH-133 and Win55,212-2. Upon further
elucidation into the molecular mechanism, we observed that both CB1 and CB2
agonists inhibited phosphorylation of AKT, a key signaling molecule controlling
cell survival, migration, and apoptosis, and reduced matrix metalloproteinase 9
expression and activity. These results suggest that CB1 and CB2 could be used as
novel therapeutic targets against NSCLC."
https://pubmed.ncbi.nlm.nih.gov/21097714/ [3681]
According to Ramer et al (2011)
"Cannabidiol inhibits lung cancer cell invasion and metastasis via intercellular
adhesion molecule-1":
"Cannabinoids inhibit cancer cell
invasion via increasing tissue inhibitor of matrix metalloproteinases-1
(TIMP-1). This study investigates the role of intercellular adhesion molecule-1
(ICAM-1) within this action. In the lung cancer cell lines A549, H358, and H460,
cannabidiol (CBD; 0.001-3 μM) elicited concentration-dependent ICAM-1
up-regulation compared to vehicle via cannabinoid receptors, transient receptor
potential vanilloid 1, and p42/44 mitogen-activated protein kinase.
Up-regulation of ICAM-1 mRNA by CBD in A549 was 4-fold at 3 μM, with significant
effects already evident at 0.01 μM. ICAM-1 induction became significant after 2
h, whereas significant TIMP-1 mRNA increases were observed only after 48 h.
Inhibition of ICAM-1 by antibody or siRNA approaches reversed the anti-invasive
and TIMP-1-upregulating action of CBD and the likewise ICAM-1-inducing
cannabinoids Δ(9)-tetrahydrocannabinol and R(+)-methanandamide when compared to
isotype or nonsilencing siRNA controls. ICAM-1-dependent anti-invasive
cannabinoid effects were confirmed in primary tumor cells from a lung cancer
patient. In athymic nude mice, CBD elicited a 2.6- and 3.0-fold increase of
ICAM-1 and TIMP-1 protein in A549 xenografts, as compared to vehicle-treated
animals, and an antimetastatic effect that was fully reversed by a neutralizing
antibody against ICAM-1 [% metastatic lung nodules vs. isotype control (100%):
47.7% for CBD + isotype antibody and 106.6% for CBD + ICAM-1 antibody]. Overall,
our data indicate that cannabinoids induce ICAM-1, thereby conferring TIMP-1
induction and subsequent decreased cancer cell invasiveness."
https://pubmed.ncbi.nlm.nih.gov/22198381/ [3680]
Meanwhile in real life:
"Conventional lung cancer treatments
include surgery, chemotherapy and radiotherapy; however, these treatments are
often poorly tolerated by patients. Cannabinoids have been studied for use as a
primary cancer treatment. Cannabinoids, which are chemically similar to our own
body’s endocannabinoids, can interact with signalling pathways to control the
fate of cells, including cancer cells. We present a patient who declined
conventional lung cancer treatment. Without the knowledge of her clinicians, she
chose to self-administer ‘cannabidiol (CBD) oil’ orally 2–3 times daily. Serial
imaging shows that her cancer reduced in size progressively from 41 mm to 10 mm
over a period of 2.5 years. Previous studies have failed to agree on the
usefulness of cannabinoids as a cancer treatment. This case appears to
demonstrate a possible benefit of ‘CBD oil’ intake that may have resulted in the
observed tumour regression. The use of cannabinoids as a potential cancer
treatment justifies further research."
https://casereports.bmj.com/content/14/10/e244195.full [1761]
Research that began in 1975 with the
discovery of the antineoplastic properties of Δ9-THC, Δ8-THC and CBN, which
inhibited the growth of Lewis lung adenocarcinoma cells. More research was
needed then and more research is still needed, now. Of course a lot of cannabis
users have delayed or prevented their death and a lot of NECUD sufferers have
not, in the intervening period.
According to "Antineoplastic activity
of cannabinoids",
"Lewis lung adenocarcinoma growth was
retarded by the oral administration of delta9-tetrahydrocannabinol (delta9-THC),
delta8-tetrahydrocannabinol (delta8-THC), and cannabinol (CBN), but not
cannabidiol (CBD). Animals treated for 10 consecutive days with delta9-THC,
beginning the day after tumor implantation, demonstrated a dose-dependent action
of retarded tumor growth. Mice treated for 20 consecutive days with delta8-THC
and CBN had reduced primary tumor size. CBD showed no inhibitory effect on tumor
growth at 14, 21, or 28 days. Delta9-THC, delta8-THC, and CBN increased the mean
survival time (36% at 100 mg/kg, 25% at 200 mg/kg, and 27% at 50 mg/kg,
respectively), whereas CBD did not. Delta9-THC administered orally daily until
death in doses of 50, 100, or 200 mg/kg did not increase the life-spans of
(C57BL/6 times DBA/2)F1 (BDF1) mice hosting the L1210 murine leukemia. However,
delta9-THC administered daily for 10 days significantly inhibited Friend
leukemia virus-induced splenomegaly by 71% at 200 mg/kg as compared to 90.2% for
actinomycin D. Experiments with bone marrow and isolated Lewis lung cells
incubated in vitro with delta9-THC and delta8-THC showed a dose-dependent
(10(-4)-10(-7)) inhibition (80-20%, respectively) of tritiated thymidine and
14C-uridine uptake into these cells. CBD was active only in high concentrations
(10(-4))."
https://pubmed.ncbi.nlm.nih.gov/1159836/ [1996]
Powells et al (2005) found that THC is
cytotoxic to leukemic cell lines:
"Concentration-dependent decreases in cell viability were seen in all cell lines
cultured with THC for 2 days".
However:
"Cytotoxic effect of THC is not mediated via the CB1-R and CB2-R."
And:
"THC does not increase p53 expression."
Moreover, THC decreases phosphorylated pERK protein expression:
"Genes in the MAPK signaling cascade that showed altered expression were DUSP6
(encoding dual specificity phosphatase 6/MAPK phosphatase 3 [MKP3]) and MAP2K2
(mitogenactivated protein kinase kinase 2/MEK2). Interestingly, MKP3 and MAP2K2
have the same intracellular target, the extracellular signal-regulated kinase 2
protein (ERK2/mitogen-activated protein kinase 1). They have, however, opposing
functions: MEK2 phosphorylates, and thereby activates ERK2, whereas MKP3
dephosphorylates ERK2, taking it to an inactive state. Accordingly, the
expression changes in response to THC observed were an increase in MKP3
expression in all 3 samples and a decrease in MAP2K2 expression (Table 2). Both
changes are consistent with decreased MAPK signaling."
https://www.researchgate.net/profile/Robert-Te-Poele/publication/8261865_Cannabis-induced_cytotoxicity_in_leukemic_cell_lines_The_role_of_the_cannabinoid_receptors_and_the_MAPK_pathway/links/53e0abbf0cf24f90ff6091e2/Cannabis-induced-cytotoxicity-in-leukemic-cell-lines-The-role-of-the-cannabinoid-receptors-and-the-MAPK-pathway.pdf?_tp=eyJjb250ZXh0Ijp7ImZpcnN0UGFnZSI6Il9kaXJlY3QiLCJwYWdlIjoicHVibGljYXRpb24iLCJwcmV2aW91c1BhZ2UiOiJfZGlyZWN0In19
[4808]
Now the idea in practice is, you
ignore alcohol causing cancer, food causing cancer, heavy metals causing cancer,
plastics causing cancer and everything else causing cancer. After you have
ignored those things for a while,...Oh! You have cancer. But the mechanisms
involved in the progress of cancer did not suddenly appear with the diagnosis of
the disease. They were there all the time, but in balance and under control.
Following the 1975 Munson et al paper on
Lewis lung adenocarcinoma, according to Abrams:
"For unclear reasons, that line of
research was not pursued further at the National Institutes of Health in the
United States, but was subsequently picked up by investigators in Spain and
Italy, who have made enormous contributions to the field.
"If cannabinoids are postulated to
have a potential anticancer effect working through the cb1 receptor, it would
follow that the brain—where the cb1 receptor is the most densely populated
seven-transmembrane domain G protein–coupled receptor—would be a good place to
start the investigation. And, in fact, numerous studies in vitro and in animal
models have suggested that cannabinoids can inhibit gliomas. Other tumour cell
lines are also inhibited by cannabinoids in vitro, and cannabinoid
administration to nude mice curbs the growth of various tumour xenografts
representing multiple solid and hematologic malignancies, including
adenocarcinomas of the lung, breast, colon, and pancreas, and also myeloma,
lymphoma, and melanoma."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4791148/ [1997]
Abrams, who can be found in the Hematology-Oncology department
at San Francisco General Hospital; also at Integrative Oncology, UCSF Osher
Center for Integrative Medicine; and also at the University of California–San
Francisco, San Francisco, CA, U.S.A., writing March 23 in Current Oncology,
wrote:
"Much attention has been paid to the
unearthing of the 2500-year-old mummy known as the 'Siberian Ice Maiden.'
Discovered in 1993, her subterranean burial chamber included a pouch of cannabis
among other archeologic findings. Magnetic resonance imaging revealed that the
princess had a primary tumour in the right breast, with axial adenopathy and
metastatic disease. It is hypothesized that the cannabis was used to manage her
pain and perhaps other symptoms, or even possibly as a treatment for her
malignant disease.
"Widely used as medicine during the
ensuing millennia, cannabis disappeared from the pharmaceutical armamentarium in
the 1940s as its prohibition took hold. Today, we are in the midst of what
appears to be something of a medicinal cannabis renaissance, with patients
across the globe gaining increased access to this potent botanical medicine. In
a 2014 WebMD poll, 82% of oncologists indicated their belief that patients
should have access to cannabis, ranking highest among medical subspecialists in
their support. Regrettably, most oncologists trained during the era of cannabis
prohibition and have no knowledge of how to use the plant as medicine. In these
days of targeted therapies and nanotechnology, the modern oncologist might feel
somewhat ill at ease recommending a herbal intervention, notwithstanding the
number of potent cytotoxic chemotherapeutic agents derived from plants."
and
"...administration of anandamide (an
endocannabinoid) together with an inhibitor of the fatty-acid amide hydrolase
that metabolizes anandamide attenuated chemotherapy-induced peripheral
neuropathy. Cannabidiol pretreatment stops paclitaxel-induced neuropathy in
mice. To date, the only human study of a cannabis-based medicine in
chemotherapy-induced peripheral neuropathy is a crossover placebo-controlled
trial of nabiximols."
and in a suggestion for more research
that might be needed...
"Even more exciting would be a study
demonstrating the potential for cannabis to actually lower the risk for
neuropathy or to prevent it from developing in the first place, as the animal
models suggest."
Meanwhile we are reminded
"The cb receptors are not present to
react with the phytocannabinoids from cannabis alone. They exist because, on
demand, humans produce endogenous cannabinoids—“endocannabinoids”—that react
with the receptors, effecting changes in intracellular signalling. It has been
suggested that the entire function of the system of cannabinoid receptors and
endocannabinoids might be to assist in modulation of the response to pain. With
that in mind, it is not surprising that an increasing body of knowledge is being
developed about the effects on pain of cannabinoid medicines." [1997]
By 2022 the same author was reporting
that
"THC and CBD may both impact the
metabolism of other pharmaceuticals and botanicals by way of cytochrome p450
interactions. To date, very few pharmacokinetic interaction studies have been
investigated to evaluate the effects of cannabis or isolated cannabinoids on
blood levels of conventional cancer therapies."
and
"No studies of cannabis to promote
weight gain in cancer patients have been reported likely due to the barriers to
conducting research with the botanical. Cannabis, however, with both antiemetic
and orexigenic effects, may be a useful therapeutic for cancer patients and
should be further explored in future clinical investigations."
https://journals.sagepub.com/doi/full/10.1177/15347354221081772 [1998]
Tai, Wong and Wen (2015), recalling
that
"Innate immunity is the first line of
defense of the body in response to exogenous insults such as bacterial, viral
and fungal infections and innate immunity acts through highly conserved
pattern-recognition receptors, such as Toll-like receptors (TLR), to coordinate
the innate inflammatory response to both endogenous and exogenous stimuli. After
engaging with their ligands, the downstream inflammatory responses of most TLRs
are mediated through the [Myeloid differentiation primary response 88]
MyD88-dependent pathway, except TLR3, which is [TIR-domain-containing
adapter-inducing interferon-β] TRIF dependent."
and they tell us a 2014
"...study by Alkanani and colleagues
also showed that induction of diabetes in the RIP-B7.1 C57BL/6 mouse model was
critically dependent on TLR3 and MyD88 pathways and an altered intestinal
microbiome was responsible for the diabetes modulation. Experimental data from
BB rats performed by Roesch and colleagues also showed the altered gut
microbiota were linked to the onset of diabetes in BB-DP (diabetes-prone)
compared to BB-DR (diabetes-resistant) rats. Moreover, Hara et al showed that
antibiotic treatment could prevent Kilham rat virus-induced insulitis and T1D in
the LEW1.WR1 rat model, suggesting that microbiota might also be involved in
virus-induced diabetes. Transfer of gut microbiota from diabetes-protected
MyD88-deficient [non-obese diabetic] NOD mice at an early age could stably alter
the composition of the gut microbiota of recipient NOD mice, reduce insulitis
and significantly delay the onset of diabetes. Taken together, these data
indicate altered gut microbiota are strongly associated with T1D and modulation
of the gut microbiota by transfer of so-called 'protective gut flora' could
delay and/or prevent diabetes development. However, how gut microbiota are
altered and what mechanisms are involved in the immune regulation by the
commensal bacteria in diabetes development need to be further investigated."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4348024/ [1546]
Can demyelination be prevented,
slowed, or reversed? Some Google search results for these show you are allowed
to believe in these things - by such treatments as lowering depression,
preventing activation of innate immune mechanisms that provoke hypoxia, and
superoxide and nitric oxide formation, increasing inspired oxygen, upregulation
of miR-23, arsa-cel gene therapy, Sphingosine 1-phosphate receptor modulation
with BAF312 (siponimod), astrocytic yes-associated protein, induction of heat
shock protein 70, administration of interferon beta-1a, glatiramer acetate, the
monoclonal antibody, BIIB033, agonists of PPAR-beta and RXR-alpha, Astragalus
polysaccharides, nervonic acid, EHP-101, thrombin inhibitors, nerve growth
factor or its analogues, transcranial electrical stimulation, a compound found
in cashew nut shells, ginger, omega-3 fatty acids, vitamin D, vitamin B12,
folate, vitamin C, glutathione, vitamin K, lithium, melatonin, lipoic acid,
niacin, and cholesterol, curcumin, thyme, rosemary, quercetin, licorice,
resveratrol, and black cumin seeds.
https://www.google.co.uk/search?q=%22preventing+demyelination%22&lr=&newwindow=1&safe=images&as_qdr=all&ei=CrypY5u2HqPosAfy6IOoDw&ved=0ahUKEwib45yMy5f8AhUjNOwKHXL0APUQ4dUDCA8&uact=5&oq=%22preventing+demyelination%22&gs_lcp=Cgxnd3Mtd2l6LXNlcnAQAzIECAAQHjIFCAAQhgMyBQgAEIYDMgUIABCGAzIFCAAQhgMyBQgAEIYDOgoIABBHENYEELADOgYIABAHEB46CggAEAgQBxAeEA86CAgAEAUQHhANOggIABAIEB4QDToKCAAQCBAeEA8QDUoECEEYAEoECEYYAFC3C1iXDmCnEWgBcAF4AIABqQGIAfMCkgEDMS4ymAEAoAEByAEIwAEB&sclient=gws-wiz-serp
[3907]
In "CNS Demyelination Syndromes
Following COVID-19 Vaccination: A Case Series" by Yasser et al (2024):
"The study was carried out on 18
patients who presented with different neurological disorders after the first or
second dose of the COVID-19 vaccine. There were eight men (44.44%) and ten women
(55.56%) with a mean age of 34.78 ± 7.13 years, ranging from 23 to 44 years. The
mean duration between the onset of symptoms and the date of the last dose of the
COVID-19 vaccine was 7.67 ± 3.83 days, ranging from 2–14 days. Regarding the
type of vaccine, 12 patients (66.67%) received the Pfizer vaccine, and the
remaining six (33.33%) received the AstraZeneca vaccine. Eight patients (44.44%)
developed neurological manifestations after the first dose of the vaccine, and
the remaining ten (55.56%) developed them after the second dose [Table 1].
"Four patients (22.22%) presented
with optic neuritis, three (16.67%) with hemiparesis, three (16.67%) with
paraparesis, three (16.67%) with seizures (GTC and myoclonic), two (11.11%) with
ataxia, one (5.56%) with hemihypesthesia, one (5.56%) with headache, and one
(5.56%) with tinnitus [Table 2]. Sixteen patients (88.89%) had brain MRI
findings suggestive of a demyelinating disorder [Figures 1 and 2], and two
(11.11%) had a normal brain MRI but with the spine MRI showing a picture of
transverse myelitis [Figure 3]. In the results of the oligoclonal band in CSF
and serum, ten patients (55.56%) had a positive oligoclonal band in the CSF
only, and the remaining eight (44.44%) had negative results. VEP was performed
for ten patients. The results showed that four (22.22%) had prolonged P 100
latency, and the remaining six had normal P 100 latency. AQP-4 was performed for
three patients and was negative [Tables 3 and 4]."
As to the potential mechanisms of
this they say:
"Although the precise mechanism of
demyelination following COVID-19 vaccinations is still not fully known, a
combination of vaccine-related variables and patient susceptibility plays a
significant role. Some individuals may experience an unintended immune reaction
as a result of the resemblance between the proteins of the viruses used for
vaccination and self-antigens (such as myelin). Another factor is the use of
immunologic adjuvants, which are substances that increase immune responses to
certain antigens and can mimic evolutionarily conserved chemicals that activate
both the innate and adaptive immune systems. TLR7 and TLR8 activation also
results in the production of type I interferon, potent T and B cell responses,
and the activation of bystander autoreactive cells. This bystander activation
and cytokine secretion by macrophages might lead to local inflammation and the
recruitment of more T-helper cells."
https://journals.lww.com/jpbs/fulltext/2024/16001/cns_demyelination_syndromes_following_covid_19.298.aspx
[3127]
Demyelinating conditions are among those
whose odds ratios increased after Covid-19 vaccination according to a VAERS
analysis by Cosgrove et al, who compared adverse events from the mRNA shots with
influenza vaccine recipients, finding increases in:
Rare Neurodegenerative & Demyelinating Conditions:
Creutzfeldt–Jakob disease (CJD) — 847× more likely to be reported compared to
flu shots
Myelitis (all types) — 31× more likely
Transverse myelitis — 21× more likely
Viral myelitis — 115× more likely
Noninfectious myelitis — 132× more likely
Prion disease (general) — 62× more likely
CNS Infections:
Meningitis (all types) — 34× more likely
Aseptic meningitis — 53× more likely
Bacterial meningitis — 36× more likely
Autoimmune encephalitis — 79× more likely
Limbic encephalitis — 146× more likely
Bickerstaff’s encephalitis — 68× more likely
Neuroborreliosis (Lyme CNS infection) — 321× more likely
Toxic encephalopathy — 157× more likely
Progressive multifocal leukoencephalopathy (PML) — 45× more likely
Herpetic CNS Reactivations:
Herpes zoster meningitis — over 1,200× more likely
Herpes zoster meningoencephalitis — 339× more likely
Herpes zoster neurological disease — 680× more likely
Herpes simplex meningitis — 132× more likely
Herpetic meningoencephalitis — 136× more likely
Varicella meningitis — 168× more likely
Brain & Spinal Abscesses:
Brain abscess — 120× more likely
Extradural abscess — 169× more likely
Spinal cord abscess — 89× more likely
Subdural abscess — 36× more likely
https://www.researchgate.net/profile/Nicolas-Hulscher/publication/395581251_COVID-19_mRNA_Vaccination_Implications_for_the_Central_Nervous_System/links/68cb55840f14e901fcd12bbc/COVID-19-mRNA-Vaccination-Implications-for-the-Central-Nervous-System?_tp=eyJjb250ZXh0Ijp7ImZpcnN0UGFnZSI6InB1YmxpY2F0aW9uIiwicGFnZSI6InB1YmxpY2F0aW9uIn1
[5461]
Anything which could ameliorate these odds ought not to be banned.
In 2000, five months after the
enactment of the ZPPPD, Derocq and colleagues investigated the "enigma" of the
CB2 receptor, becoming the first to discover a role in immune cell
differentiation and chemotaxis, as:
"...activation of the CB2 receptors
induced an up-regulation of nine genes involved in cytokine synthesis,
regulation of transcription, and cell differentiation. A majority of them are
under the control of the transcription factor NF-kB, whose nuclear translocation
was demonstrated. Many features of the transcriptional events, reported here for
the first time, appeared to be related to an activation of a cell
differentiation program, suggesting that CB2 receptors could play a role in the
initialization of cell maturation. Moreover, we showed that CB2-activated
wild-type HL-60 cells developed properties usually found in host defense
effector cells such as an enhanced release of chemotactic cytokines and an
increased motility, characteristic of more mature cells of the
granulocytic-monocytic lineage."
https://www.jbc.org/article/S0021-9258(19)80340-X/pdf [3531]
In 2005 the CB2 receptor was shown to
be essential for macrophage chemotaxis.
https://www.jbc.org/article/S0021-9258(19)46626-X/pdf [3530]
Low dose THC was found to reduce the
progression of atherosclerosis in mice. According to Steffens et al (2005):
"Lymphoid cells isolated from
THC-treated mice showed diminished proliferation capacity and decreased
interferon-γ secretion. Macrophage chemotaxis, which is a crucial step for the
development of atherosclerosis, was also inhibited in vitro by THC. All these
effects were completely blocked by a specific CB2 receptor antagonist. Our data
demonstrate that oral treatment with a low dose of THC inhibits atherosclerosis
progression in the apolipoprotein E knockout mouse model, through pleiotropic
immunomodulatory effects on lymphoid and myeloid cells."
https://www.jbc.org/article/S0021-9258(19)46626-X/pdf [3532]
This could turn out to be useful and
adds to the risks of NECUD as SARS-CoV-2, the virus that causes COVID-19, can
directly infect the arteries of the heart and cause the fatty plaque inside
arteries to become highly inflamed, increasing the risk of heart attack and
stroke, according to "SARS-CoV-2 infection triggers pro-atherogenic inflammatory
responses in human coronary vessels" by Eberhardt et al (2023):
"Here we report that SARS-CoV-2 viral
RNA is detectable and replicates in coronary lesions taken at autopsy from
severe COVID-19 cases. SARS-CoV-2 targeted plaque macrophages and exhibited a
stronger tropism for arterial lesions than adjacent perivascular fat,
correlating with macrophage infiltration levels. SARS-CoV-2 entry was increased
in cholesterol-loaded primary macrophages and dependent, in part, on
neuropilin-1. SARS-CoV-2 induced a robust inflammatory response in cultured
macrophages and human atherosclerotic vascular explants with secretion of
cytokines known to trigger cardiovascular events. Our data establish that
SARS-CoV-2 infects coronary vessels, inducing plaque inflammation that could
trigger acute cardiovascular complications and increase the long-term
cardiovascular risk."
Cholesterol-laden foam cells were the
most susceptible to infection and unable to readily clear the virus. This
suggested that foam cells might act as a reservoir of SARS-CoV-2 in the
atherosclerotic plaque:
"The significantly higher
accumulation of nucleoprotein (NP) in foam cells compared to macrophages
infected with SARS-CoV-2 USA WA1/2020 isolate (Fig. 2b and Extended Data Fig.
3b) confirmed a higher susceptibility of foam cells to the virus."
https://www.nature.com/articles/s44161-023-00336-5 [3640]
In a 2015 study macrophage chemotaxis
was found to be activated by CB2R agonists but independently of them. According
to Taylor et al:
"Activation of CB2 has been
demonstrated to induce directed immune cell migration. However, the ability of
CB2 to act as a chemoattractant receptor in macrophages remains largely
unexplored. Using a real-time chemotaxis assay and a panel of chemically diverse
and widely used CB2 agonists, we set out to examine whether CB2 modulates
primary murine macrophage chemotaxis. We report that of 12 agonists tested, only
JWH133, HU308, L-759,656 and L-759,633 acted as macrophage chemoattractants.
Surprisingly, neither pharmacological inhibition nor genetic ablation of CB2 had
any effect on CB2 agonist-induced macrophage chemotaxis. As chemotaxis was
pertussis toxin sensitive in both WT and CB2-/- macrophages, we concluded that a
non-CB1/CB2, Gi/o-coupled GPCR must be responsible for CB2 agonist-induced
macrophage migration. The obvious candidate receptors GPR18 and GPR55 could not
mediate JWH133 or HU308-induced cytoskeletal rearrangement or JWH133-induced
β-arrestin recruitment in cells transfected with either receptor, demonstrating
that neither are the unidentified GPCR. Taken together our results conclusively
demonstrate that CB2 is not a chemoattractant receptor for murine macrophages.
Furthermore we show for the first time that JWH133, HU308, L-759,656 and
L-759,633 have off-target effects of functional consequence in primary cells and
we believe that our findings have wide ranging implications for the entire
cannabinoid field."
They say:
"Real-time analysis of changes in
cell morphology demonstrated that L-759,656 induced concentration dependent
signalling (Fig. 3D), whereas the chemotaxis negative compounds CP55,950, AM1241
(Fig. 3D), GP1a and WIN55212-2 (Fig. 3E) did not induce signalling at any
concentration tested. In summary, using both Boyden chamber and real-time
chemotaxis assays we have shown that only a subset of CB2 agonists act as
primary murine macrophage chemoattractants and only chemotaxis positive
compounds were capable of inducing changes in cell morphology as measured by
changes in electrical impedance.
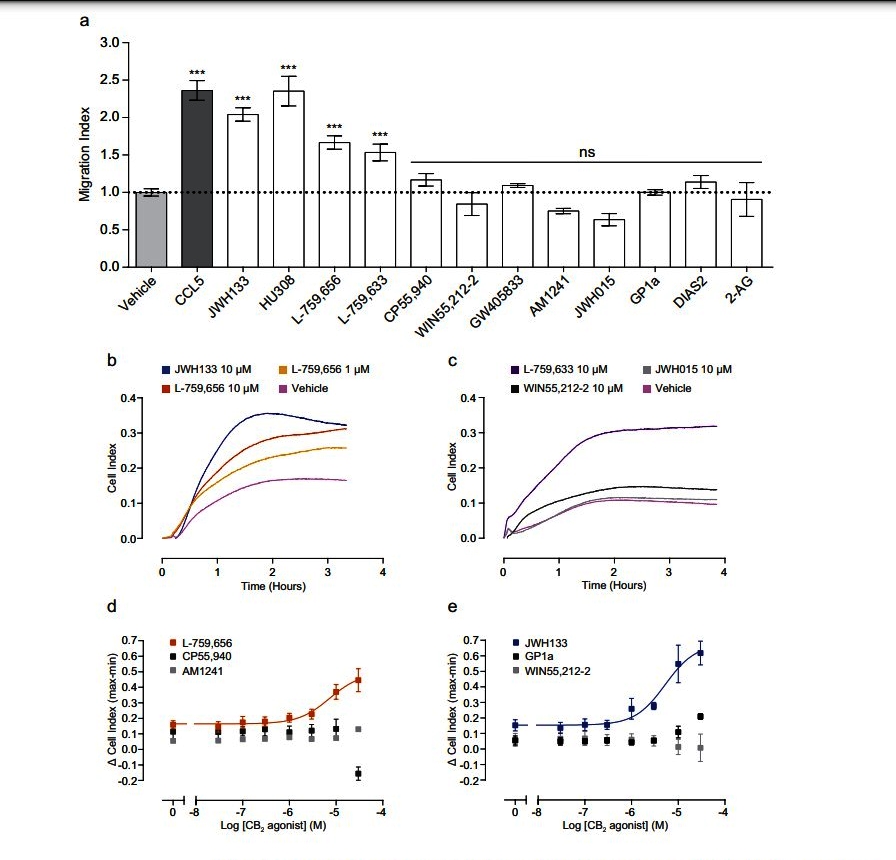 https://www.nature.com/articles/srep10682.pdf [3352]
https://www.nature.com/articles/srep10682.pdf [3352]
Writing in 2016, F Rohan Walker and
Raz Yirmani describe the shift in thinking about microglia:
"The remarkable number of discoveries
over the last decade concerning microglial involvement in the most fundamental
CNS processes has caught many by surprise. To a certain extent, this surprise
has been driven by long established assumptions concerning the primary role of
microglia as immune type cells within the brain. Indeed, the literature prior to
2005 is filled with descriptions of microglia as the macrophages of the brain,
with detailed investigation of how these cells function as the first-responders
to tissue injury or insult (Kreutzberg, 1996). However, 2005 represented a
departure from this classical outlook, with the first observation of these cells
in real time being reported (Davalos et al., 2005, Nimmerjahn et al., 2005).
These multiphoton imaging studies revealed that microglia are incredibly active,
rapidly extending and retracting their processes, apparently in an effort to
scan their microenvironment. The question on all ‘microgliologists’ minds at the
time was, “scanning for what?” In rapid succession, it became apparent that
rather than patrolling for threats (or only for threats), microglia were in fact
making continuous contact with pre- and post-synaptic terminals to monitor
synaptic activity (Kettenmann et al., 2013, Tremblay et al., 2010, Wake et al.,
2009). Furthermore, during development, such microglial-neuronal interactions
were found to be crucial for synaptic maturation and pruning, which underlie the
activity-dependent tuning and refinement of neuronal circuits and the brain’s
global connectivity pattern (Paolicelli et al., 2011, Schafer et al., 2012, Zhan
et al., 2014). These discoveries subsequently proved to be immensely important,
as there was now a credible chain of evidence through which immunological
activity could directly influence both neuronal architecture and function."
https://www.sciencedirect.com/science/article/abs/pii/S0889159116300514
[3533]
According to "Neuroscience" 2nd
edition (2001):
"By acting as an electrical
insulator, myelin greatly speeds up action potential conduction (Figure 3.14).
For example, whereas unmyelinated axon conduction velocities range from about
0.5 to 10 m/s, myelinated axons can conduct at velocities up to 150 m/s. The
major reason underlying this marked increase in speed is that the time-consuming
process of action potential generation occurs only at specific points along the
axon, called nodes of Ranvier, where there is a gap in the myelin wrapping (see
Figure 1.4F). If the entire surface of an axon were insulated, there would be no
place for current to flow out of the axon and action potentials could not be
generated. As it happens, an action potential generated at one node of Ranvier
elicits current that flows passively within the myelinated segment until the
next node is reached. This local current flow then generates an action potential
in the neighboring segment, and the cycle is repeated along the length of the
axon. Because current flows across the neuronal membrane only at the nodes (see
Figure 3.13), this type of propagation is called saltatory, meaning that the
action potential jumps from node to node. Not surprisingly, loss of myelin, as
occurs in diseases such as multiple sclerosis, causes a variety of serious
neurological problems."
https://www.ncbi.nlm.nih.gov/books/NBK10921/ [2273]
A 2019 view of multiple sclerosis:
"The pathogenesis of this disease is
characterized by neuroinflammation leading to demyelination and consequently
paralysis. Although the complete etiology and the pathogenesis of MS remains
unclear, there is evidence that increased migration of myelin-reactive CD4 + Th1
and Th17 cells across the blood-brain barrier (BBB) causing inflammation in the
CNS which leads to axonal demyelination of neurons, axonal injury,
oligodendrocyte loss, neuronal damage, and glial plaques (Wu and Chen, 2016)." [1285]
In 2022 Biomedicine published
"Neurological Benefits, Clinical Challenges, and Neuropathologic Promise of
Medical Marijuana: A Systematic Review of Cannabinoid Effects in Multiple
Sclerosis and Experimental Models of Demyelination" by Longoria et al.
"Despite current therapeutic
strategies for immunomodulation and relief of symptoms in multiple sclerosis
(MS), remyelination falls short due to dynamic neuropathologic deterioration and
relapses, leading to accrual of disability and associated patient
dissatisfaction. The potential of cannabinoids includes add-on
immunosuppressive, analgesic, neuroprotective, and remyelinative effects."
and
"MS exhibits heterogeneity with
respect to clinical, genetic, radiographic, and pathologic features. Triggers
for MS development and relapses involve interactions between genetic, lifestyle,
and environmental factors. Genome-wide association studies (GWAS) have
identified over 230 genetic risk loci for MS, revealing a ~5-fold increase in
the risk of MS when the presence of the class II variant HLA-DRB1*15:01 is
combined with an absence of the class I variant HLA-A*02. Other risk factors for
MS include smoking, alcohol consumption, obesity, low dietary intake of vitamin
D, lower sun exposure, latitude farther away from equator, and certain chronic
viral infections. Longitudinal analysis using data from US military recruits
over a period of 20 years has revealed that Epstein–Barr virus (EBV) increased
the risk of subsequent MS by 32-fold. MS patients have significantly higher
serum anti-EBV nuclear antigen-1 (EBNA-1) titers as compared to healthy
controls, and the higher EBV responses correlate with more extensive lesion and
gray matter tissue destruction as measured by magnetization transfer imaging in
RRMS patients. Molecular mimicry may explain the association between EBV titers
and more severe neuropathology since ~20–25% of MS patients have anti-EBNA1
antibodies that cross-react with the CNS protein glial cell adhesion molecule
(GlialCAM].
"In humanized non-obese
diabetic-severe combined immunodeficiency (NOD-scid) IL2 receptor
γ-chain-deficient (huNSG) mice, EBV infection was found to synergize with
HLA-DR15 by priming cross-reactive CD4+ T-cell clones which control the viral
infection less efficiently. It is hypothesized that EBV might activate ancestral
human endogenous retroviruses (HERVs) in the human genome. Antibodies to other
viruses have been associated with increased MS conversion and relapse including
human herpes virus 6 (HHV-6). It is believed that the induction of demyelination
in the brain and spinal cord in MS may be initiated by excess innate and
myelin-specific autoimmune activation mechanisms that are sensitive to chronic
viral infections and gut microbiome status and perpetuated by the loss of
oligodendrocytes and their progenitors through either perforin-mediated lysis or
apoptotic cell death."
and
"Early studies also demonstrated that
cannabinoids could ameliorate clinical progression, downregulate proinflammatory
T cells, and promote remyelination in TMEV-IDD."
and
"Clinical studies suggest that
combinations of the cannabinoids derived from the Cannabis sativa plant,
cannabidiol (CBD) and Δ9-tetrahydrocannabinol (Δ9-THC), are comparably as
effective for short-term symptomatic relief as conventional pharmacotherapeutic
agents while causing less side effects. An oromucosal spray formulation,
Sativex® (nabiximols), which contains Δ9-THC and CBD in a nearly 1:1 ratio, was
licensed in the United Kingdom in 2010 as a prescription-only medicine for the
treatment of spasticity in multiple sclerosis."
14 animal and 14 human studies were
reviewed. In the human tests:
"Spasticity outcomes were reported in
nine studies: three randomized, double-blind, placebo-controlled clinical
trials, and six cohort/observational studies. The quality of evidence [Cochrane]
GRADE [Grading of Recommendation Assessment, Development and Evaluation] was
moderate in six and low in three of the studies (Table 7 and Table 8). The total
number of subjects for spasticity studies was 1582. The mean maximal change in
NRS [numerical rating scale] spasticity scores was 2.8 (range 0.04 to 7.4) lower
than baseline. Assessments were repeated more than once within a period of 4
months, and two of the studies extended up to 12 months. In the three clinical
trials, the mean difference in NRS spasticity scores was 0.62 (range 0.5 to
0.83) points lower in the treatment groups as compared to controls, as a placebo
effect was noted in two of the trials."
"Cannabis-based medicine has long
been known to be useful in pain management including central pain in multiple
sclerosis and post-operative pain. Promising benefits of cannabis use and
medical marijuana have also been observed for relief of neurologic symptoms in
patients with movement disorders, including Parkinson disease and Huntington
disease. Furthermore, oral CBD has been used for the treatment of drug-resistant
seizures in children with tuberous sclerosis (TSC), and Epidiolex® (pure CBD)
has been approved for the treatment of intractable epilepsy in patients with
developmental epileptic encephalopathies including Dravet syndrome and
Lennox–Gastaut syndrome (LGS). Multiple mechanisms are implicated in the ability
of CBD to modulate seizures that include antagonism of CB1, CB2, GPR18, GPR55,
and voltage-gated sodium channel (VGSC) receptors; agonism of GABAA receptors;
activation and desensitization of TRPV1/2 receptors; and allosteric modulation
of opioid receptor types μ [mu] and δ [delta], leading to inhibition of
glutaminergic N-methyl-D-aspartate (NMDA) receptors."
...
"In addition to neuroprotective
effects, cannabinoid treatment in vitro and in vivo has antiseizure, antiemetic,
anti-inflammatory, and antitumor effects which include antiproliferative,
proapoptotic, autophagic, antiadhesion, antimigration, and antiangiogenic
mechanisms affecting cancer cells, cell lines, human tumor xenografts, and
animal cancer models."
...
"Recent studies have provided
evidence implicating lysophosphatidic acid (LPA) signaling through its G
protein-coupled receptor, LPA1, as a mechanism of macrophage activation that
correlates with the onset of relapses and greater disease severity in both EAE
and MS. Interactions between the endocannabinoid system and the LPA system in
the mouse brain have been identified in studies demonstrating upregulation of
LP1 receptor activity in CB1 knockout mice. Cannabinoids have also been shown to
promote a reparative activation state of microglia and macrophages, diminishing
the reactivity and the number of microglia in Theiler’s virus-induced
demyelination disease. RNA sequencing analysis has revealed that oral CBD
treatment of EAE mice can reduce the expression of CXCL9, CXCL10, and IL-1β,
leading to decreased macrophage infiltration into the CNS, and also induce
myeloid-derived suppressor cells (MDSCs)."
...
"CB2-mediated facilitation of
oligodendrocyte survival involved decreases in the phosphorylation of the
protein kinase R (PKR)-like endoplasmic reticulum (ER) kinase (PERK), eIF2α,
ATF4, and GADD34 (Growth Arrest and DNA Damage-inducible protein) signaling
pathway in microglia."
...
"Treatment with Δ9-THC also promoted
axonal remyelination in organotypic cerebellar cultures. CB1 receptors regulate
the mTORC1 signaling pathway during oligodendrocyte development, and the
remyelination effects could be abrogated by both mTORC1 blockade and CB1
receptor-selective antagonism."
...
"Analysis of patient-reported outcome
measures in 312 patients from the UK medical cannabis registry revealed
statistically significant improvements at 6 months in the Generalized Anxiety
Disorder Scale score (GAD-7, p < 0.001), the EuroQol Group EQ-5D-5L index value
(p < 0.001), the EQ-5D Visual Analog Scale score (VAS, p < 0.012), and the Sleep
Quality Scale (SQS, p < 0.001) score."
https://www.mdpi.com/2227-9059/10/3/539 [1938]
In 2022, examining the effects of
cannabinoids on toll-like receptors, Fitzpatrick et al
"...employed the use of poly(I:C) and
lipopolysaccharide (LPS) to induce viral TLR3 and bacterial TLR4 signalling, and
[peripheral blood mononuclear cells] PBMCs were pre-exposed to plant-derived
highly purified THC (10 μM), CBD (10 μM), or a combination of both
phytocannabinoids (1:1 ratio, 10:10 μM), prior to LPS/poly(I:C) exposure. TLR3
stimulation promoted the protein expression of the chemokine CXCL10 and the type
I IFN-β in PBMCs from both cohorts. THC and CBD (delivered in 1:1 combination at
10 μM) attenuated TLR3-induced CXCL10 and IFN-β protein expression in PBMCs from
[people with multiple sclerosis] pwMS and HCs, and this effect was not seen
consistently when THC and CBD were delivered alone."
As their paper "Botanically-Derived ∆
9 -Tetrahydrocannabinol and Cannabidiol, and Their 1:1 Combination, Modulate
Toll-like Receptor 3 and 4 Signalling in Immune Cells from People with Multiple
Sclerosis" explains:
"A body of preclinical data indicate
that THC and CBD have anti-inflammatory and antioxidant propensity, and TLRs are
cannabinoid targets. Indeed, recent findings from our laboratory indicate that
both THC and CBD target inflammatory signalling governed by TLRs in human
macrophages, specifically TLR3 and TLR4. Such data, particularly with regard to
THC, are important in the context of evidence linking the endocannabinoid system
(ECS) with the pathogenesis of MS. Indeed, the expression of the endocannabinoid
anandamide (AEA) is enhanced in CSF, lymphocytes, and plasma of pwMS, while
knock-out of the cannabinoid receptors CB1 and CB2, and administration of the
AEA metabolising enzyme fatty acid amide hydrolase (FAAH), alters the clinical
progression of [experimental autoimmune encephalomyelitis] EAE in mice."
https://www.mdpi.com/1420-3049/27/6/1763/pdf?version=1646732841 [1547]
"Δ9-Tetrahydrocannabinol and cannabidiol
selectively suppress toll-like receptor (TLR) 7– and TLR8-mediated
interleukin-1β production by human CD16+ monocytes by inhibiting its
post-translational maturation" say Sermet et al (2025):
"We hypothesized that THC and CBD suppress toll-like receptor (TLR) 7– or
TLR8-induced inflammatory profiles by CD16+ and CD16− monocytes, specifically
interleukin (IL) 1β maturation. Cannabinoid receptor 2 selective agonist,
JWH-015, was used to deduce whether cannabinoid receptor 2 signaling alone can
mimic immune-modulating properties of THC. Primary human CD16+ and CD16−
monocytes were pretreated with THC, CBD, or JWH-015 and then activated through
TLR7 or TLR8. Activated monocytes mainly produced IL-1β, tumor necrosis
factor-⍺, and IL-6. We show that THC and CBD, but not JWH-015, exert
anti-inflammatory effects on primary human monocyte apoptosis-associated
speck-like protein–incorporating inflammasome formation and subsequent caspase-1
activity, contributing to suppressed IL-1β production. In addition, mRNA
expression of IL1B, CASP1, NLRP3, and PYCARD were unaffected by THC. Minimal THC
effects were observed on TLR8-mediated AIM2 mRNA expression. Collectively,
results from these studies suggest THC and CBD may be useful in mitigating
IL-1β–mediated acute or chronic inflammation."
https://jpet.aspetjournals.org/article/S0022-3565(25)39828-9/abstract
[5109]

https://iris.unibs.it/retrieve/ddc633e2-aede-4e2e-e053-3705fe0a4c80/Ziegler%20Blood%202010.pdf
[5110]
So we need to know a bit more about
oligodendrocytes. These were discovered by the application of a novel silver
carbonate staining method in 1918 by Pio Del Río Hortega.
"After developing modifications of
Achúcarro’s ammoniacal silver method (Del Río Hortega, 1916), Del Río Hortega
challenged the accuracy of Ramón y Cajal’s concept about the third element of
CNS which grouped non neuronal (first element) and non-astrocytic (second
element) cells (Ramón y Cajal, 1913b, 1916; García-Marín et al., 2007). Later,
he described his silver carbonate staining technique which was the
methodological key to identify two distinct elements: the microglia, the “true
third element”, and what he called initially “interfascicular cells” and later
oligodendroglia (Del Río Hortega, 1918, 1920, 1921)."
And, writing in 2015, Achucarro
Basque Center for Neuroscience authors say that:
"He established their ectodermal
origin and suggested that they built the myelin sheath of CNS axons, just as
Schwann cells did in the periphery. Notably, he also suggested the trophic role
of OLGs for neuronal functionality, an idea that has been substantiated in the
last few years....Yet, the difficulty of metal impregnation methods and their
variability in results, delayed for some decades the confirmation of his great
insights into oligodendrocyte biology until the development of electron
microscopy and immunohistochemistry."
https://www.frontiersin.org/articles/10.3389/fnana.2015.00092/full [1557]
From whence does damage to
oligodendrocytes originate? All around us, in everyday household products, in my
home and yours. According to Cohn et al at the Department of Genetics and Genome
Sciences, Case Western Reserve University School of Medicine, Cleveland, who...
"...revealed environmental chemicals
in two classes that disrupt oligodendrocyte development through distinct
mechanisms. Quaternary compounds, ubiquitous in disinfecting agents, hair
conditioners, and fabric softeners, were potently and selectively cytotoxic to
developing oligodendrocytes through activation of the integrated stress
response. Organophosphate flame retardants, commonly found in household items
such as furniture and electronics, were non cytotoxic but prematurely arrested
oligodendrocyte maturation. Chemicals from each class impaired human
oligodendrocyte development in a 3D organoid model of prenatal cortical
development. In analysis of epidemiological data from the CDC’s National Health
and Nutrition Examination Survey, adverse neurodevelopmental outcomes were
associated with childhood exposure to the top organophosphate flame retardant
identified by our oligodendrocyte toxicity platform."
https://www.biorxiv.org/content/biorxiv/early/2023/02/12/2023.02.10.528042.full.pdf
[4518]
A Madrid-Boston collaboration states
that it is not just a matter of maintenance for people already diagnosed with
MS, but also of remyelination - i.e. repair of myelin - and prevention of
demyelination in the first place that cannabinoids impart to the user
population, and they say:
"Neuroprotective therapies, and those
targeting oligodendrocyte progenitors and other CNS cells, such as astrocytes
and microglia, are likely to promote recovery and prevent long-term
neurodegeneration. Indeed, the neuroprotective effects of CBs have been
confirmed in different models of injury and CNS disease, like Alzheimer’s
Disease (Martín-Moreno et al., 2012; Schubert et al., 2019), stroke (Zarruk et
al., 2012; Kolb et al., 2019), ischemic injury (Fernández-López et al., 2007),
Parkinson’s Disease (García et al., 2011) and ALS (Rodríguez-Cueto et al.,
2018). In the TMEV-IDD model of progressive MS, the administration of synthetic
CBs (Arévalo-Martín et al., 2003) or pCBs (Mecha et al., 2013; Feliú et al.,
2015) has been associated with an improvement in neurological defects, also
observed by inhibiting selective AEA uptake (Ortega-Gutiérrez et al., 2005) or
the enzymatic hydrolysis of 2-AG (Feliú et al., 2017). In this latter study,
both remyelination and axon preservation was showed, while chondroitin sulfate
proteoglycans diminished through the involvement of CB1R and CB2R. In addition,
2-AG administration or inhibition of its hydrolysis favors oligodendrocyte
precursor cell (OPC) differentiation (Gomez et al., 2015) and, by diminishing
the excitotoxicity of oligodendrocytes, demyelination is prevented in the EAE
(Bernal-Chico et al., 2015) and the cuprizone model (Manterola et al., 2018)."
https://www.frontiersin.org/articles/10.3389/fncel.2020.00034/full [1549]
https://link.springer.com/article/10.1007/s11481-015-9609-x [1550]
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4052930/ [3563]
Next, to a recent but flawed review,
"Drugs and Bugs: The Gut-Brain Axis and Substance Use Disorders":
"CBD is immune suppressive in both in
vitro and in vivo models (Nichols and Kaplan 2019). In contrast, when whole
cannabis was explored in individuals with cannabis use disorder, IL-1β, IL-6,
IL-8 and TNF⍺ were increased in cannabis users compared to controls."
https://link.springer.com/article/10.1007%2Fs11481-021-10022-7 [784]
Kaplan's review of 2021 concluded:
"The risks of respiratory symptoms
and of COPD seemed to be related to a synergistic interaction between marijuana
and tobacco, but did not occur in cannabis-only smokers."
https://link.springer.com/content/pdf/10.1007/s41030-021-00171-8.pdf[4640]
By 2016 Omar Abdel-Salam at the
Department of Toxicology and Narcotics in the Medical Division of the National
Research Centre, in Cairo, Egypt, was convinced that "The effects of Cannabis
are, however, the sum of its constituents."
This is an article which begins with
the sentence:
"Cannabis is the most commonly abused
illicit substance worldwide."
But he could have said, "Cannabis is
the most commonly prohibited substance used worldwide."
It's clear from the context of the
following paragraph that what Abdel-Salam means to say is:
"The effects of Cannabis are,
however, [more than] the sum of its constituents. There are more than 70
different cannabinoids and these may have effects that are synergistic with or
antagonistic to Δ9-THC effects. Other important constituents are terpenoids and
the flavonoids flavocannabiside. One terpenoid that is beta-caryophyllene has
been shown to inhibit the development of gastric lesions evoked by ethanol or
0.6 N HCl when given orally to rats."
https://www.sciencedirect.com/science/article/pii/S1995764516300712 [788]
A year later mrstinkysgreengarden.com
discussing the benefits of linalool:
"Modern research has confirmed the
practices of ancient civilizations, revealing strong medical efficacy for many
severe conditions.
"Linalool has been shown to be a
major anti-inflammatory, meaning it helps those with cancer and arthritis.
Research has also proven the value of this terpene for treating anxiety and
insomnia due to its sedative properties.
"Linalool is actually one of the
minor terpenes available in certain strains of cannabis. It is found in smaller
quantities than major terpenes like myrcene (the most common), pinene, and
limonene. It emits a floral, sometimes spicy aroma. Hundreds of species of
plants produce linalool, including a variety of mints and herbs."
http://www.mrstinkysgreengarden.com/2017/06/the-terpene-linalool-vs-opioid-addiction.html
[975]
"It comes in two main forms: an R isomer
(R-linalool, also known as licareol) and an S isomer (S-linalool, or
coriandrol).
"Linalool smells floral and musky with a faint hint of spice much like lavender.
However it is far more ubiquitous in nature, with R-Linalool found in over 200
different plants such as flowering plants in the Lamiaceae family (lavender,
lemon balm, bergamot, rosemary, sage) as well as the present in the Lauraceae
and Apiaceae plant families."
https://cannigma.com/plant/terpenes/linalool/ [5447]
One starting point for a
consideration of CCx synergistic or antagonistic effects is sleep.
In your mission to construct an
artificial optimally balanced mix of CCx so you can patent a drug affecting
pathway Y for condition Z, you might start by varying the simplest variables,
THC and CBD, then add linalool, or any one or more of these major or minor
cannabinoids or terpenes, or not.
As you can see, there will be quite a
lot of sleep experiments to do, to invent cannabis.
More sleep might not be the only solution. If
you are simply unable to get enough "β-Caryophyllene (BCP) prevented cognitive
deficits induced by acute sleep deprivation" according to Cao et al (2026):
"Here we administered β-caryophyllene (BCP), the highly selective CB2R agonist,
and observed whether cognitive impairment following acute sleep deprivation
(ASD) was prevented. Our results demonstrated that administration of BCP for 3
days before ASD markedly prevented both long-term spatial learning and memory,
along with short-term episodic recall in mice exposed to ASD, but the four
experimental groups of mice exhibited comparable hippocampal CB2R expression
without marked differences. In addition, BCP effectively reversed the disruption
of long-term potentiation (LTP) in the hippocampal CA1 area induced by ASD, but
failed to reestablish long-term depression (LTD) or paired pulse ratio (PPR).
Furthermore, BCP prevented synaptic ultrastructural alterations and promoted the
recovery of both dendritic spine density and morphological complexity within the
CA1 subfield of the hippocampus. Overall, these results indicate that BCP
prevented cognitive impairment after ASD by preventing damage to synaptic
function and structural plasticity, preventing alterations of pyramidal cell
dendritic complexity and density of dendritic spines within CA1 subregion of
hippocampi of mice."
https://www.sciencedirect.com/science/article/abs/pii/S0028390825004605
[5542]
The Court may wish to note that no clergyman or superstition-encouraging
politician has a problem with in BCP in broccoli, beer, black currant, citrus
fruits, pepper (oil), rosemary, or thyme.
Advances in the relatively recent
tools to study sleep mean that, as with the microbiome and the inflammasome,
most of the findings postdate the applicable treaties and legislation.
Matthew P Walker is a British author,
scientist and professor of neuroscience and psychology at the University of
California, Berkeley. He is a public intellectual focused on the subject of
sleep. A list of studies to which has contributed can be located at
https://scholar.google.com/citations?user=11L5sOQAAAAJ&hl=en [3090]
Matt Walker has a 19 minute talk
about the deleterious effects of poor sleep. (Warning: contains testicles).
"Sleep is your life-support system
and Mother Nature's best effort yet at immortality, says sleep scientist Matt
Walker. In this deep dive into the science of slumber, Walker shares the
wonderfully good things that happen when you get sleep -- and the alarmingly bad
things that happen when you don't, for both your brain and body. Learn more
about sleep's impact on your learning, memory, immune system and even your
genetic code..."
In case you are too tired to watch it
all, Walker emphasizes that sleep is not a luxury but a biolgical necessity, and
declares
"the shorter your sleep, the shorter
your life"
The genetic profile of healthy adults
limited to six hours' sleep for one week was compared to their baseline profile
when they received a "normal" eight hours.
"First, a sizeable and significant
711 genes were distorted in their activity, caused by a lack of sleep. The
second result was that about half of those genes were actually increased in
their activity. The other half were decreased.
"Now those genes that were switched
off by a lack of sleep were genes associated with your immune system....in
contrast, those genes that were actually upregulated or increased by way of a
lack of sleep were genes associated with the promotion of tumours, genes
associated with long-term chronic inflammation of the body, and genes associated
with stress, and, as a consequence, cardiovascular disease. There is simply no
aspect of your wellness that can retreat at the sign of sleep deprivation."
and
"And let me just tell you about one
area that we've moved this work out into, clinically, which is the context of
aging and dementia. Because it's of course no secret that, as we get older, our
learning and memory abilities begin to fade and decline. But what we've also
discovered is that a physiological signature of aging is that your sleep gets
worse, especially that deep quality of sleep that I was just discussing. And
only last year, we finally published evidence that these two things, they're not
simply co-occurring, they are significantly interrelated. And it suggests that
the disruption of deep sleep is an underappreciated factor that is contributing
to cognitive decline or memory decline in aging, and most recently we've
discovered, in Alzheimer's disease as well."
https://www.ted.com/talks/matt_walker_sleep_is_your_superpower [3086]
In a poll of 229 "mental health experts" the
statement "sleep deprivation can reduce mental health" was pronounced true by a
ratio of 110:1. We may conclude from the 1.8% don't-knows that in fact only 2
experts disagreed with this idea.
[sleep deprivation number 2 5046]
https://podcasts.apple.com/us/podcast/what-experts-really-think-about-smartphones-and/id1594471023?i=1000711141508
[5046]
NECUD may affect quality of sleep.
According to Möller-Levet et al (2013):
"Insufficient sleep and circadian
rhythm disruption are associated with negative health outcomes, including
obesity, cardiovascular disease, and cognitive impairment, but the mechanisms
involved remain largely unexplored. Twenty-six participants were exposed to 1 wk
of insufficient sleep (sleep-restriction condition 5.70 h, SEM = 0.03 sleep per
24 h) and 1 wk of sufficient sleep (control condition 8.50 h sleep, SEM = 0.11).
Immediately following each condition, 10 whole-blood RNA samples were collected
from each participant, while controlling for the effects of light, activity, and
food, during a period of total sleep deprivation. Transcriptome analysis
revealed that 711 genes were up- or down-regulated by insufficient sleep.
Insufficient sleep also reduced the number of genes with a circadian expression
profile from 1,855 to 1,481, reduced the circadian amplitude of these genes, and
led to an increase in the number of genes that responded to subsequent total
sleep deprivation from 122 to 856. Genes affected by insufficient sleep were
associated with circadian rhythms (PER1, PER2, PER3, CRY2, CLOCK, NR1D1, NR1D2,
RORA, DEC1, CSNK1E), sleep homeostasis (IL6, STAT3, KCNV2, CAMK2D), oxidative
stress (PRDX2, PRDX5), and metabolism (SLC2A3, SLC2A5, GHRL, ABCA1). Biological
processes affected included chromatin modification, gene-expression regulation,
macromolecular metabolism, and inflammatory, immune and stress responses. Thus,
insufficient sleep affects the human blood transcriptome, disrupts its circadian
regulation, and intensifies the effects of acute total sleep deprivation. The
identified biological processes may be involved with the negative effects of
sleep loss on health, and highlight the interrelatedness of sleep homeostasis,
circadian rhythmicity, and
metabolism."
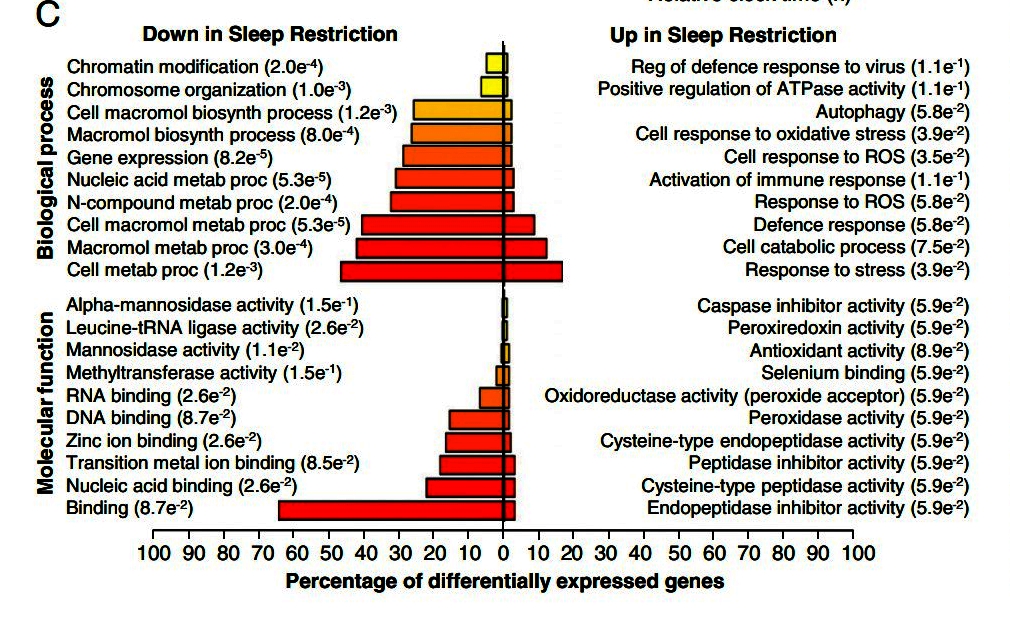
https://www.pnas.org/doi/pdf/10.1073/pnas.1217154110 [3651]
Forbes (6 April 2025) reports:
"Medical cannabis is a significantly more effective sleep aid than prescription
and over-the-counter sleep remedies, according to a survey of medical cannabis
patients....The survey of more than 1,000 people who have been using medical
cannabis to help them sleep found that nearly 70% of patients reported that
cannabis is a better sleep aid than prescription sleeping pills. More than nine
out of 10 (91.2%) said medical cannabis was more effective than OTC sleep
remedies.
"The survey was conducted by Bloomwell Group GmbH, a Frankfurt, Germany-based
medical cannabis company. The survey included 1,086 people who have been using
cannabis to treat sleep disorders since 2023. The survey is the largest in
Europe to date to study the effectiveness of medical cannabis as a sleep aid,
Bloomwell reports."
https://www.forbes.com/sites/ajherrington/2025/04/06/medical-cannabis-is-a-better-sleep-aid-than-otc-and-rx-pills-new-survey/
[4915]
"Effectiveness of a Cannabinoids Supplement on Sleep and Mood in Adults With
Subthreshold Insomnia: A Randomized Double-Blind Placebo-Controlled Crossover
Pilot Trial" from Hausenblas et al (2025) at Jacksonville University, Florida
reported results in 20 insomnia patients:
"When compared to PC [Placebo Condition], the CS [Cannabinoids Supplement]
Condition had significantly improved sleep quality/efficiency, insomnia
symptoms, and health-related quality of life, p < 0.05."
https://onlinelibrary.wiley.com/doi/10.1002/hsr2.70481 [5209]
NECUD can accelerate aging by inducing sleep deprivation. Even one night's
sleeplessness increases amyloid accumulation. [see
3557 on cannabis and amyloid
clearance]. The study "β-Amyloid accumulation in the human brain after one night
of sleep deprivation" is from Shokri-Kojori et al (2018) at the NIH Laboratory
of Neuroimaging, National Institute on Alcohol Abuse and Alcoholism:
"The effects of acute sleep deprivation on β-amyloid (Aβ) clearance in the human
brain have not been documented. Here we used PET and 18F-florbetaben to measure
brain Aβ burden (ABB) in 20 healthy controls tested after a night of rested
sleep (baseline) and after a night of sleep deprivation. We show that one night
of sleep deprivation, relative to baseline, resulted in a significant increase
in Aβ burden in the right hippocampus and thalamus. These increases were
associated with mood worsening following sleep deprivation, but were not related
to the genetic risk (APOE genotype) for Alzheimer’s disease. Additionally,
baseline ABB in a range of subcortical regions and the precuneus was inversely
associated with reported night sleep hours. APOE genotyping was also linked to
subcortical ABB, suggesting that different Alzheimer’s disease risk factors
might independently affect ABB in nearby brain regions. In summary, our findings
show adverse effects of one-night sleep deprivation on brain ABB and expand on
prior findings of higher Aβ accumulation with chronic less sleep."
https://www.pnas.org/doi/10.1073/pnas.1721694115 [4802]
NECUD-induced poor sleep quality could make your balls smaller. Here's Figure 2
from one testicle study by Zhang et al (2018):
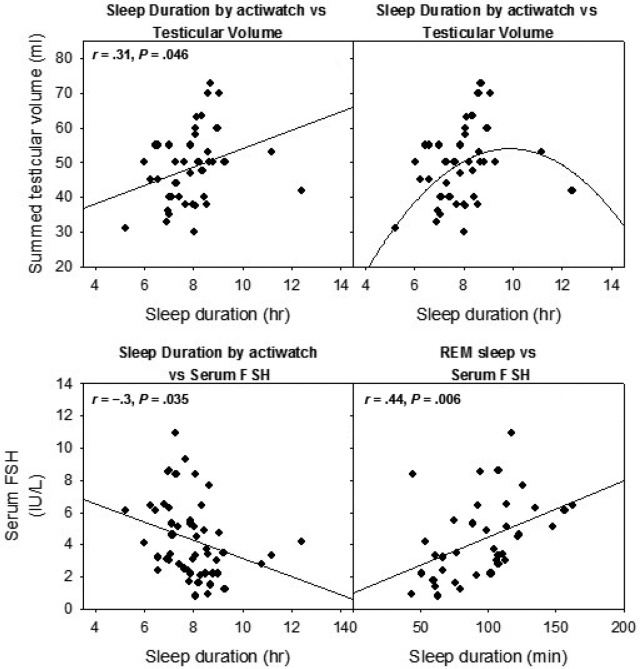
"Sleep duration and architecture were
measured by actigraphy and polysomnography, testicular volume by Prader
orchidometer, total testosterone by liquid chromatography tandem mass
spectrometry, free testosterone by equilibrium dialysis, and luteinizing hormone
and follicle-stimulating hormone (FSH) by immunochemiluminometric assay."
They note:
"An earlier study showed inverse-U
shaped relationships between sleep duration and semen parameters and concluded
that semen volume and total sperm count fell with sleep durations less than or
equal to 6.5 hours or more than 9 hours."
While...
"Testicular volumes measured by
Prader orchidometer remain the foundation of the standard andrological
examination, and such measurements have long been accepted as important clinical
markers of male fertility that correlate positively with sperm count."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6175801/ [3089]
Does Slovenia want or need a law to
prevent the dimensional adequacy of its testicles?
Along the way we should not exclude the
possibility of cannabis effects on semen quality. Avoiding the expectancy of
preconceptions by the use of direct measurements, Joseph et al (2025) found a
similarly non-linear association:
"Overall, 22.6% of participants reported current cannabis use and 3.3% reported
daily use. Nearly 6% of participants had low semen volume (≤1.5 mL), 13% low
sperm concentration (≤15 million/L), 8% low TSC (≤39 million), 25% low sperm
motility (≤40%), and 11% low TMSC (≤16 million). Adjusted %Ds (95% CIs)
comparing current cannabis use versus non-use were −3.2 (−9.1, 2.7) for semen
volume, 3.5 (−10.3, 19.5) for sperm concentration, −0.6 (−14.3, 15.3) for TSC,
2.5 (−2.9, 8.0) for motility, and 3.0 (−13.4, 22.4) for TMSC. Cannabis use ≥1
times/week (vs. non-use) was associated with low semen volume (RR = 2.16, 95% CI
= 0.93–5.04). Associations were imprecise and showed no monotonic association
between frequency of cannabis use and the semen parameters evaluated.
"Conclusion
In this North American preconception cohort study, current cannabis use was not
appreciably associated with semen quality."
https://onlinelibrary.wiley.com/doi/10.1111/andr.70056 [5533]
In 2021 scientists stumbled upon an
amazing discovery for sufferers of chronic insomnia.
Happily the restorative effect on
testicles via REM sleep latency is not confined to cannabis, as reported by
Dudysová et al in Czechia in "The Effects of Daytime Psilocybin Administration
on Sleep: Implications for Antidepressant Action" (2020):
"Serotonergic agonist psilocybin is a
psychedelic with antidepressant potential. Sleep may interact with psilocybin’s
antidepressant properties like other antidepressant drugs via induction of
neuroplasticity. The main aim of the study was to evaluate the effect of
psilocybin on sleep architecture on the night after psilocybin administration.
Regarding the potential antidepressant properties, we hypothesized that
psilocybin, similar to other classical antidepressants, would reduce rapid eye
movement (REM) sleep and prolong REM sleep latency. Moreover, we also
hypothesized that psilocybin would promote slow-wave activity (SWA) expression
in the first sleep cycle, a marker of sleep-related neuroplasticity. Twenty
healthy volunteers (10 women, age 28–53) underwent two drug administration
sessions, psilocybin or placebo, in a randomized, double-blinded design. Changes
in sleep macrostructure, SWA during the first sleep cycle, whole night EEG
spectral power across frequencies in non-rapid eye movement (NREM) and REM
sleep, and changes in subjective sleep measures were analyzed. The results
revealed prolonged REM sleep latency after psilocybin administration and a trend
toward a decrease in overall REM sleep duration. No changes in NREM sleep were
observed. Psilocybin did not affect EEG power spectra in NREM or REM sleep when
examined across the whole night. However, psilocybin suppressed SWA in the first
sleep cycle. No evidence was found for sleep-related neuroplasticity, however, a
different dosage, timing, effect on homeostatic regulation of sleep, or other
mechanisms related to antidepressant effects may play a role. Overall, this
study suggests that potential antidepressant properties of psilocybin might be
related to changes in sleep."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7744693/ [3088]
While the Defendant completely understand
Slovenians' desire to limit the size of each others' testicles, on a careful
viewing of the antediluvian condition of the legislative instruments compared to
these researches with implications for testicle health, I'd like to see the
ZPPPD's classification of cannabis and psychedelics justified in the context of
everything we do know about these substances and sleep, and by extension the
measurement in question.
Zhai et al (2025) examined "The Intersection
of Psychedelics and Sleep: Exploring the Impacts on Sleep Architecture, Dream
States, and Therapeutic Implications", saying:
"Psychedelics hold promise as therapeutic agents for sleep disorders such as
insomnia, PTSD, and nightmares, which are often linked to underlying
psychological conditions like anxiety, depression, and trauma. These substances,
particularly psilocybin, LSD, and DMT, may offer novel treatment options by
modulating sleep architecture, emotional processing, and neurotransmitter
activity."
https://pubs.acs.org/doi/10.1021/acsptsci.5c00234 [5089]
In "Treating insomnia symptoms with
medicinal cannabis: a randomized, crossover trial of the efficacy of a
cannabinoid medicine compared with placebo" (2021) Walsh et al
"...employed a double-blind,
randomized, placebo-controlled, crossover design to evaluate the safety and
efficacy of a cannabinoid formulation which included THC, CBD, and CBN
(ZTL-101), for treating insomnia symptoms in patients with chronic insomnia
disorder."
and
"Of the 23 participants who completed
the protocol, 12 (52%) were taking a double dose of ZTL-101 on the 14th night.
Sixteen (69.5%) were taking a double dose of placebo on the 14th night.
Twenty-one of 21 participants (100%) (n = 2 missing data) guessed that they were
receiving the active medication when taking ZTL-101. 'Improvement in sleep
quality' was the reason for their guess in 17 (81%) with adverse reactions the
reason in the remaining four participants. When taking the placebo, 18 of 23
participants (78%) thought they were receiving placebo. Sixteen noted 'lack of
improvement in sleep quality' as the reason for their guess that they were
receiving placebo."
...leading Walsh et al to conclude:
"Two weeks of nightly sublingual
administration of a cannabinoid extract (ZTL-101) is well tolerated and improves
insomnia symptoms and sleep quality in individuals with chronic insomnia
symptoms."
https://academic.oup.com/sleep/article/44/11/zsab149/6296857#311780504
[3087]
We have a graphic from the Sleep
Foundation about brain waves:
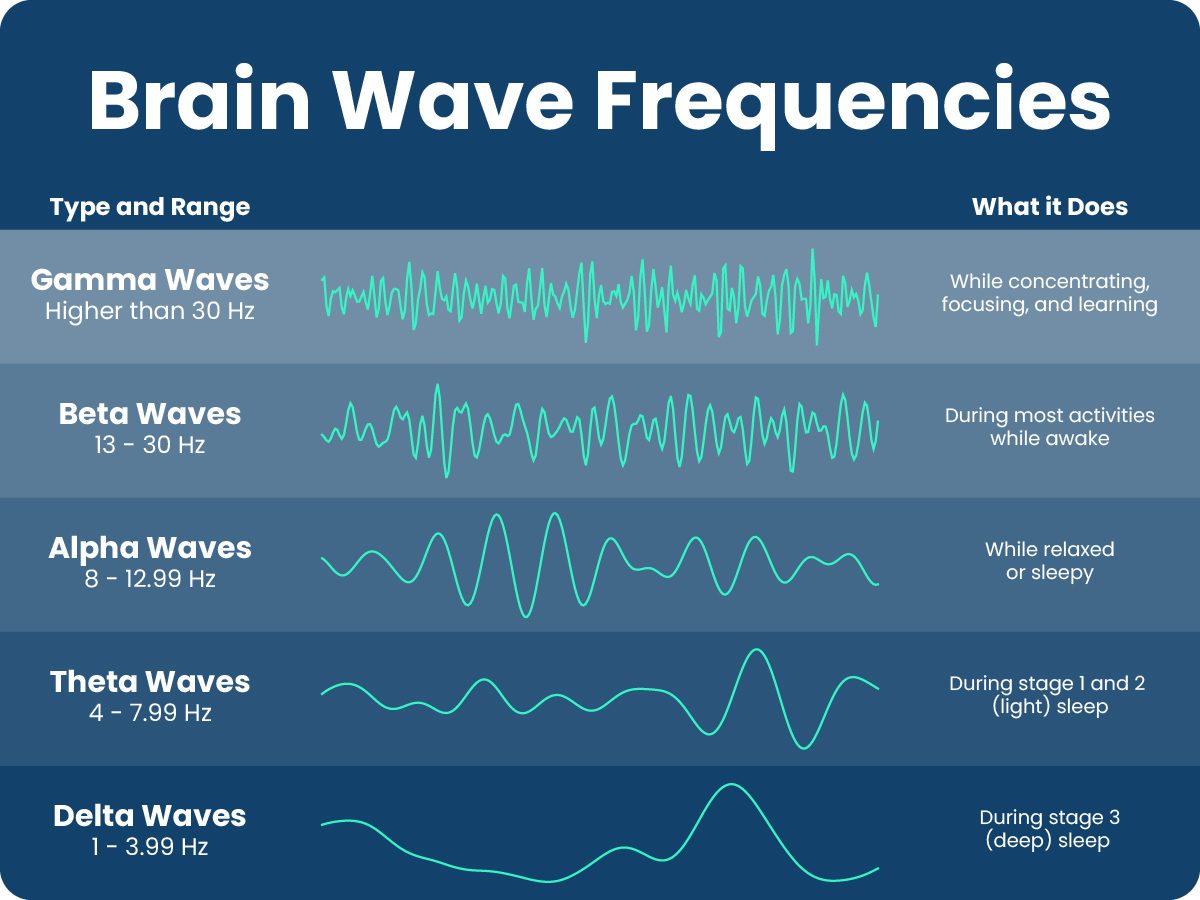
"Alpha brain waves are the main brain
wave pattern that develops when a person becomes drowsy and transitions from
wakefulness to sleep. They continue during the early phase of sleep until they
are replaced by slower theta waves.
"Alpha waves are also present when a
person is awake and relaxing, such as with the eyes closed or during meditation
Alpha wave production is associated with states of creativity, but they tend to
disappear when a person performs mental activity requiring greater attention."
and
"Alpha-delta sleep is an abnormal
brain wave pattern associated with certain health conditions. In alpha-delta
sleep, the brain produces alpha waves during deep sleep, when it would normally
be producing slow delta waves. The intrusion of alpha waves can make sleep
unrefreshing and leave people feeling sleepy during the day.
"Alpha-delta sleep is found in many
people with fibromyalgia, a chronic pain condition. It can also affect people
with arthritis, depression, sleep disorders, and lupus. Some evidence suggests
that alpha-delta sleep can cause pain or make pain worse for people with
fibromyalgia. But more research is needed to determine whether alpha-delta sleep
causes pain, or if it is caused by pain instead."
https://www.sleepfoundation.org/how-sleep-works/alpha-waves-and-sleep [3091]
Data of interest to those willing to
risk illegal sleeping continued in 2022's "Acute effects of combined cannabidiol
(CBD) and ∆9-tetrahydrocannabinol (THC) in insomnia disorder: A randomised,
placebo-controlled trial using high-density EEG" by Suarez et al:
"Compared to placebo, CBD/THC
significantly decreased TST [total sleep time] (-24.5 min, p=0.047) with no
significant change to WASO [wake after sleep onset] (+10.7 min, p=0.422).
CBD/THC significantly decreased time spent in REM (rapid eye movement] sleep
(-33.9min, p<0.001) and increased REM sleep latency (+65.6 min, p=0.008).
Preliminary high-density EEG analysis revealed increased alpha activity during
REM sleep overlying the parietal cortex (p<0.05). CBD/THC did not impair
next-day (+12 h post-treatment) cognitive performance, alertness or simulated
driving performance (all p’s>0.05). Eighty-five mild, non-serious, adverse
events were reported (55 during CBD/THC; most common dry mouth, drowsiness, and
fatigue).
"Conclusions
An acute dose of 200 mg CBD and 10 mg
THC reduced TST and the time spent in REM sleep. Analysis of all high-density
EEG outcomes is ongoing. CBD/THC did not affect next-day performance. Further
research is required to determine the impact of chronic cannabinoid dosing on
REM sleep and other objective sleep outcomes in insomnia disorder."
https://academic.oup.com/sleepadvances/article/3/Supplement_1/A3/6811668?login=false
[1875]
The trials continued. In 2024 Surayev
et al looked at possible "next day" impairment in insomnia patients using an
oral THC/CBD cannabis product:
"Here, we examined possible ‘next
day’ impairment following evening administration of a typical medicinal cannabis
oil in adults with insomnia disorder, compared to matched placebo. This paper
describes the secondary outcomes of a larger study investigating the efects of
THC/CBD on insomnia disorder. Twenty adults [16 female; mean (SD) age, 46.1
(8.6) y] with physician-diagnosed insomnia who infrequently use cannabis
completed two 24 h in-laboratory visits involving acute oral administration of
combined 10 mg THC and 200 mg CBD (‘THC/CBD’) or placebo in a randomised,
double-blind, crossover trial design. Outcome measures included ‘next day’ (≥9 h
post-treatment) performance on cognitive and psychomotor function tasks,
simulated driving performance, subjective drug efects, and mood. We found no
diferences in ‘next day’ performance on 27 out of 28 tests of cognitive and
psychomotor function and simulated driving performance relative to placebo.
THC/CBD produced a small decrease (-1.4%, p=.016, d=-0.6) in accuracy on the
Stroop-Colour Task (easy/congruent) but not the Stroop-Word Task
(hard/incongruent). THC/ CBD also produced a small increase (+8.6, p=.042,
d=0.3) in self-ratings of Sedated at 10 h post-treatment, but with no
accompanying changes in subjective ratings of Alert or Sleepy (p’s>0.05). In
conclusion, we found a lack of notable ‘next day’ impairment to cognitive and
psychomotor function and simulated driving performance following evening use of
10 mg oral THC, in combination with 200 mg CBD, in an insomnia population who
infrequently use cannabis."
https://link.springer.com/content/pdf/10.1007/s00213-024-06595-9.pdf [3124]
On the other hand, Suraev et al found
in "Acute effects of combined cannabidiol (CBD) and ∆9-tetrahydrocannabinol
(THC) in insomnia disorder: A randomised, placebo-controlled trial using
high-density EEG" (2022) that a high THC:CBD ratio product actually shortened
total sleep time (TST).
"Compared to placebo, CBD/THC
significantly decreased TST (-24.5 min, p=0.047) with no significant change to
WASO [wake after sleep onset] (+10.7 min, p=0.422). CBD/THC significantly
decreased time spent in REM sleep (-33.9min, p<0.001) and increased REM [rapid
ey movement] sleep latency (+65.6 min, p=0.008). Preliminary high-density EEG
analysis revealed increased alpha activity during REM sleep overlying the
parietal cortex (p<0.05). CBD/THC did not impair next-day (+12 h post-treatment)
cognitive performance, alertness or simulated driving performance (all
p’s>0.05). Eighty-five mild, non-serious, adverse events were reported (55
during CBD/THC; most common dry mouth, drowsiness, and fatigue)." [1875]
In 2024 prohibition was no longer
able to prevent Arnold et al publishing "A sleepy cannabis constituent:
cannabinol and its active metabolite influence sleep architecture in rats" in
Nature:
"Medicinal cannabis is being used
worldwide and there is increasing use of novel cannabis products in the
community. Cannabis contains the major cannabinoids, Δ9-tetrahydrocannabinol
(Δ9-THC) and cannabidiol (CBD), but also an array of minor cannabinoids that
have undergone much less pharmacological characterization. Cannabinol (CBN) is a
minor cannabinoid used in the community in “isolate’ products and is claimed to
have pro-sleep effects comparable to conventional sleep medications. However, no
study has yet examined whether it impacts sleep architecture using objective
sleep measures. The effects of CBN on sleep in rats using polysomnography were
therefore examined. CBN increased total sleep time, although there was evidence
of biphasic effects with initial sleep suppression before a dramatic increase in
sleep. CBN increased both non-rapid eye movement (NREM) and rapid eye movement
(REM) sleep. The magnitude of the effect of CBN on NREM was comparable to the
sleep aid zolpidem, although, unlike CBN, zolpidem did not influence REM sleep.
Following CBN dosing, 11-hydroxy-CBN, a primary metabolite of CBN surprisingly
attained equivalently high brain concentrations to CBN. 11-hydroxy-CBN was
active at cannabinoid CB1 receptors with comparable potency and efficacy to
Δ9-THC, however, CBN had much lower activity. We then discovered that the
metabolite 11-hydroxy-CBN also influenced sleep architecture, albeit with some
subtle differences from CBN itself. This study shows CBN affects sleep using
objective sleep measures and suggests an active metabolite may contribute to its
hypnotic action."
https://www.nature.com/articles/s41386-024-02018-7 [3844]
Wu et al (2025) found that "Cannabidiol regulates circadian rhythm to improve
sleep disorders following general anesthesia in rats":
"An electrode was embedded in the skull for cortical EEG recording in 24 male SD
rats, which were randomized into control, propofol, CBD treatment, and diazepam
treatment groups (n=6). Eight days later, a single dose of propofol (10 mg/kg)
was injected via the tail vein with anesthesia maintenance for 3 h in the latter
3 groups, and daily treatment with saline, CBD or diazepam was administered via
gavage; the control rats received only saline injection. A wireless system was
used for collecting EEG, EMG, and body temperature data within 72 h after
propofol injection. After data collection, blood samples and hypothalamic tissue
samples were collected for determining serum levels of oxidative stress markers
and hypothalamic expressions of the key clock proteins.
"Results: Compared with the control rats, the rats with CBD treatment showed
significantly increased sleep time at night (20:00-6:00), especially during the
time period of 4:00-6:00 am. Compared with the rats in propofol group, which had
prolonged SWS time and increased sleep episodes during 18:00-24:00 and
sleep-wake transitions, the CBD-treated rats exhibited a significant reduction
of SWS time and fewer SWS-to-active-awake transitions with increased SWS aspects
and sleep-wake transitions at night (24:00-08:00). Diazepam treatment produced
similar effect to CBD but with a weaker effect on sleep-wake transitions.
Propofol caused significant changes in protein expressions and redox state,
which were effectively reversed by CBD treatment."
https://pubmed.ncbi.nlm.nih.gov/40294924/ [5181]
According to "Pilot Study on the Effect of Cannabidiol-Coated Fabric for Pillow
Covers Improves the Sleep Quality of Shift Nurses" by Afzal et al (2025):
"Of the 55 participants, 10 were men (18.2%) and 45 were women (81.8%). At
baseline, all participants exhibited poor sleep quality (PSQI ≥ 5). However,
after three weeks of using CBD-coated pillow covers, subjective sleep quality
significantly improved, with 7.3% of participants achieving PSQI scores <5.
Additionally, slight changes in sleep patterns were observed, with increases in
both light sleep and deep sleep durations. Light sleep duration increased from a
baseline of 196.21 ± 65.28 to 206.57 ± 59.15 min two weeks after intervention (p
= 0.337). Similarly, deep sleep duration showed a modest increase from 61.97 ±
21.01 min to 64.35 ± 22.19 min (p = 0.288). Furthermore, a significant reduction
in anxiety levels was reported (p < 0.005)."
https://www.mdpi.com/2227-9032/13/6/585 [5205]
Twelve years after the ZPPPD came
into force, the importance of the glymphatic system, a CNS garbage disposal
system, was discovered. Here's a beginners' guide.
https://pmc.ncbi.nlm.nih.gov/articles/PMC4636982/ [3653]
Was General Smuts right to interfere with
the human race's sleep? Overall, authors find equivocal help with sleep from CBD
but more positive results with THC [5522].
Assistance to the recently discovered glymphatic system has downstream benefits
in dementia and cardiovascular health via improved sleep - Hong et al (2025)
find support for this in "MRI markers of cerebrospinal fluid dynamics predict
dementia and mediate the impact of cardiovascular risk":
"Using the UK Biobank, we measured CSF dynamics: perivascular space (PVS)
volume, diffusion tensor image analysis along the PVS (DTI-ALPS), blood oxygen
level–dependent CSF (BOLD-CSF) coupling, and choroid plexus (CP) volume. We
assessed cardiovascular risk factors and their associations with CSF dynamics
and dementia based on general practitioner, mortality, and hospital records.
Mediation analysis evaluated CSF dysfunction in cardiovascular risk–dementia
relationships.
"RESULTS
Lower DTI-ALPS, lower BOLD-CSF coupling, and higher CP volume predicted
dementia, but PVS volume did not. DTI-ALPS and CP volume mediated the effect of
white matter hyperintensities and diabetes duration on dementia.
"DISCUSSION
Impaired CSF dynamics may lead to dementia and partially mediate cardiovascular
risk–dementia associations."
https://alz-journals.onlinelibrary.wiley.com/doi/10.1002/alz.70699 [5528]
In 2025 hemifusomes, a new organelle, arrived:
"Hemifusomes are fused vesicles, or sacs of fluid, that were previously unknown
to exist inside cells.
"They were discovered using cryo-electron tomography, which literally freezes
them in time, and confirmed to be actual organelles and not just background
noise.
"Because hemifusomes collect and recycle junk proteins, they could mean more
effective treatments for diseases caused and aggravated by protein plaque
buildup, such as Alzheimer’s."
https://www.popularmechanics.com/science/health/a65284366/new-cell-organelle/
[5148]
According to the NIH authors of the discovery:
"The pleiomorphic structure and dynamic behavior of cellular endomembrane
systems have been extensively studied using classical electron microscopy.
However, fixation and staining constraints limit the in situ visualization of
transient interactions, such as membrane fusion, scission, and intraluminal
vesicle formation, potentially overlooking intermediate structures like membrane
hemifusion. Using in situ cryo-electron tomography in four mammalian cell lines,
we identify heterotypic hemifused vesicles featuring an extended hemifusion
diaphragm consistently associated with a 42-nanometer proteolipid nanodroplet
(PND). We designate these vesicular organelle complexes as 'hemifusomes.'
Hemifusomes constitute up to 10% of vesicular organelles at the cell periphery
but do not engage in canonical endocytic pathways. These structures exhibit
diverse conformations and frequently contain intraluminal vesicles. Building on
the continuum of related morphologies observed, we propose that hemifusomes
serve as platforms for vesicular biogenesis, mediated by the PND. These findings
provide direct in situ evidence of long-lived hemifused vesicle complexes and
introduce an ESCRT-independent model for multivesicular body (MVB) formation."
Asked about these and their apparent common aim with the glymphatic system, Grok
offered its opinion as follows:
"At first glance, hemifusomes and the glymphatic system operate at different
scales and contexts: hemifusomes are intracellular organelles found across
various cell types, while the glymphatic system is a macroscopic network
specific to the brain’s waste clearance. However, there are intriguing points
where they might intersect or complement each other:
"Shared Goal of Waste Management:Hemifusomes are hypothesized to recycle or
dispose of cellular membranes and junk proteins within individual cells. The
glymphatic system, on the other hand, clears interstitial waste (including
proteins like amyloid-beta) from the brain’s extracellular space. If hemifusomes
are involved in breaking down intracellular protein aggregates, they could feed
into the glymphatic system by preparing waste for extracellular clearance. For
instance, proteins processed by hemifusomes might be exocytosed into the
interstitial space, where the glymphatic system could then transport them out
via CSF.
"Cellular vs. Systemic Scale:
The glymphatic system relies on the coordinated action of glial cells, blood
vessels, and CSF flow, but the efficiency of this system depends on the health
of individual cells, including their ability to manage internal waste. If
hemifusomes enhance intracellular protein recycling, they could reduce the
burden on the glymphatic system by preventing excessive waste accumulation that
would otherwise need to be cleared externally. This aligns with Ebrahim’s
hypothesis that hemifusomes prevent the 'buildup of stuff' that could 'gum up'
cellular operations, as noted in the Live Science article.
"Neurodegenerative Disease Link:
Both systems are relevant to neurodegenerative diseases. The glymphatic system’s
role in clearing amyloid-beta during sleep is well-documented, while
hemifusomes’ potential to manage protein plaques could address the intracellular
origins of such aggregates. A study from PMC on protein recycling pathways in
neurodegenerative diseases highlights how impaired intracellular mechanisms lead
to aggregate formation, suggesting that hemifusomes might act as an upstream
regulator, feeding into the glymphatic system’s downstream clearance process.
"Independence from Endosomes:
Ebrahim’s research indicates hemifusomes do not work with endosomes, which are
involved in endocytosis and vesicle trafficking. This independence suggests
hemifusomes might represent a novel pathway for waste handling, potentially
interfacing with the glymphatic system in brain cells where both processes could
coexist. For example, hemifusomes might process waste internally, while the
glymphatic system handles the extracellular efflux, creating a two-tiered waste
management strategy."
And Grok's suggestions for future research as of 8 July 2025:
"To confirm any relationship, researchers could:Use cryo-ET to image hemifusomes
in brain tissue, particularly in glial cells where AQP4 channels are active.
"Track fluorescently labeled proteins processed by hemifusomes to see if they
enter the glymphatic pathway.
"Conduct longitudinal studies in mouse models, combining glymphatic tracers with
hemifusome-specific markers, to observe waste flow from intracellular to
systemic levels."
https://x.com/i/grok/share/g4OriPUD4oT3VIy2CfnWT2psv [5147]
While it is too soon to speculate on interactions between the ECS and
vesiculogenesis via hemifusomes, endocannabinoids have been shown to have an
influence on the canonical ESCRT endocytic pathways, as DeMarino et al reported
in 2022:
"Our data suggest that CBD significantly reduces the number of EVs released from
infected cells and that this may be mediated by reducing viral transcription and
autophagy activation. Therefore, CBD may exert a protective effect by
alleviating the pathogenic effects of EVs in HIV-1 and CNS-related infections."
https://pmc.ncbi.nlm.nih.gov/articles/PMC8869966/ [5149]
And of the "Interplay between the
Glymphatic System and the Endocannabinoid System: Implications for Brain Health
and Disease" (2023) Osuna-Ramos et al say:
"The GS is subject to dynamic
regulation by various factors. Sleep plays a crucial role in modulating
glymphatic function, with increased glymphatic activity occurring during
non-rapid eye movement stage 3 (NREM 3). Arousal level, blood-brain barrier
(BBB) permeability, and neurotransmitters such as norepinephrine, adenosine, and
gamma-aminobutyric acid (GABA) influence glymphatic clearance efficiency. The GS
is also influenced by vascular pulsatility, glial cell activity, and the
glymphatic-lymphatic interaction."
and
"Scientific evidence has effectively
showcased the potential of cannabinoids, both endogenous and exogenous in origin
(derived from cannabis or synthesized), in mitigating symptomatic manifestations
associated with diverse neurodegenerative ailments encompassing MS, HD, PD, AD,
and ALS. This influence may stem from their effects on the GS, facilitating the
clearance of neurotoxic substances and protein aggregates, regulating
neuroinflammatory responses, and upholding cerebral equilibrium (Figure 2).
Increased expression of cannabinoid receptors, particularly CB2R, has been noted
in human brain tissues afflicted by ALS, MS, and AD. The interplay between the
BBB and potential shifts in the expression of cannabinoid receptors within
cerebral endothelium has been the subject of investigation.
"These insights collectively suggest
that a compromised or dysregulated ECS could potentially contribute to the
symptomatology observed in these conditions through direct modulation of the GS
and the BBB."
See the aforementioned Figure 2 for a
schematic representation of the BBB under varying conditions.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10743431/ [3654]
Lundgaard et al (2018) propose
"Beneficial effects of low alcohol exposure, but adverse effects of high alcohol
intake on glymphatic function":
"Prolonged intake of excessive
amounts of ethanol is known to have adverse effects on the central nervous
system (CNS). Here we investigated the effects of acute and chronic ethanol
exposure and withdrawal from chronic ethanol exposure on glymphatic function,
which is a brain-wide metabolite clearance system connected to the peripheral
lymphatic system. Acute and chronic exposure to 1.5 g/kg (binge level) ethanol
dramatically suppressed glymphatic function in awake mice. Chronic exposure to
1.5 g/kg ethanol increased GFAP expression and induced mislocation of the
astrocyte-specific water channel aquaporin 4 (AQP4), but decreased the levels of
several cytokines. Surprisingly, glymphatic function increased in mice treated
with 0.5 g/kg (low dose) ethanol following acute exposure, as well as after one
month of chronic exposure. Low doses of chronic ethanol intake were associated
with a significant decrease in GFAP expression, with little change in the
cytokine profile compared with the saline group. These observations suggest that
ethanol has a J-shaped effect on the glymphatic system whereby low doses of
ethanol increase glymphatic function. Conversely, chronic 1.5 g/kg ethanol
intake induced reactive gliosis and perturbed glymphatic function, which
possibly may contribute to the higher risk of dementia observed in heavy
drinkers."
https://www.nature.com/articles/s41598-018-20424-y [3655]
An explanation of aquaporin:
https://x.com/NikoMcCarty/status/1969407466141335631 [5445]
GFAP appeared in 1969, becoming a
standard marker for fundamental and applied CNS and research into
neurodegenerative diseases, TBI, genetic disorders, and chemical insults (such
as going outside in Ptuj or drinking in Ptuj) in 1989.
https://www.uniprot.org/uniprotkb/P14136/publications [3656]
https://pubmed.ncbi.nlm.nih.gov/11059815/ [3658]
The glymphatic system was
characterized and named by Maiken Nedergaard in 2012.
https://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC3551275&blobtype=pdf
[3657]
Alcohol also affects REM and slow
wave sleep:
"Alcohol before sleep increased the
rate of slow-wave-sleep (SWS) accumulation across all three nights and decreased
the rate of REM sleep accumulation at the start of each night. Alcohol also
decreased the total amount of REM sleep but did not affect the total amount of
SWS each night.
"Conclusions
These data indicate that drinking
alcohol before sleep substantially affects sleep architecture, including changes
to the rate of accumulation of SWS and REM sleep. We show that alcohol disrupts
normal sleep architecture, leading to a significant decrease in REM sleep; thus,
the use of alcohol as a sleep aid remains a public health concern."
https://academic.oup.com/sleep/advance-article-abstract/doi/10.1093/sleep/zsae003/7515846?redirectedFrom=fulltext&login=false
[4390]
To complete the circle, Davis et al (2025)
found "Daily associations between sleep quality, stress, and cannabis or alcohol
use among veterans":
"Poor sleep quality predicts increased stress and higher next-day alcohol use in
veterans.
"Cannabis use is linked to reduced stress and better same-night sleep quality.
"Stress mediates the relationship between poor sleep quality and alcohol
consumption.
"Dynamic structural equation modeling reveals bidirectional sleep-stress
interactions.
"Results emphasize the need for tailored sleep and substance use interventions
for veterans."
https://www.sciencedirect.com/science/article/abs/pii/S0376871625001140
[5186]
A not unreasonable belief is that you
might get away with less sleep if sleep is of higher quality.
In 2000 Cantero observed:
"...transient REM-alpha bursts, which
lasted about 3 s and were accompanied by no increase in the EMG amplitude,
appeared in all subjects who participated in this study, showing a higher
density in the third and fourth REM cycle during phasic in comparison with tonic
periods. The bandpass filtered signals showed the highest spectral contribution
for the slower alpha components (8-9 Hz), the occipital scalp regions being the
main generator source of this brain activity."
This led "Alpha burst activity during
human REM sleep: descriptive study and functional hypotheses" (2000) to conclude
"...that REM-alpha bursts may work as
micro-arousals (or incomplete arousals) facilitating the brain connection with
the external world in this cerebral state, whereas REM-alpha arousals - usually
longer and accompanied by changes in the EMG amplitude - generate a shift of
brain state associated with sleep fragmentation (complete arousal)."
"REM-alpha bursts described in this
work should not be mistaken for arousals or, at least, for complete arousals."
https://www.sciencedirect.com/science/article/abs/pii/S1388245799003181?via%3Dihub
[3092]
And back in 1984, when government
decisions about the quantity and quality of your sleep were not perceived as an
issue, Tyson et al found:
"Alpha activity during REM sleep
without signs of awakening can discriminate between the blind classification of
prelucid, lucid, and nonlucid dreams. 10 good dream recallers (aged 19–31 yrs)
were aroused after relatively high or low amplitude REM alpha. The spectral and
temporal characteristics of EEG alpha within each REM period were associated
with lucidity and other content dimensions. Each type of dream had a reasonably
distinct pattern of REM alpha. High amplitude alpha was found to be associated
with prelucid dreams and bizarre content, which is consistent with theories of
waking alpha activity and the hypothesis that lucidity sometimes emerges from
prelucid experiences. Data are also consistent with the idea that lucidity is a
viable dream content dimension. When interpreted in terms of systems theory,
results imply that training that emphasizes dream content control may constrain
the potential information integration function of lucid dreams."
https://psycnet.apa.org/record/1985-11505-001 [3092]
One thing that could keep you awake
is an addiction of some kind. In 2021 when Oruç Yunusoğlu at the Department of
Pharmacology, Faculty of Medicine, Bolu Abant Izzet Baysal University, Bolu,
Turkey, using the CPP technique, found that linalool has anti-addiction
properties:
"Treatment with linalool reduced the
acquisition and reinstatement, and precipitated the extinction of
ethanol-induced CPP in mice. Acquisition and reinstatement of alcohol-induced
CPP were significantly reduced by acamprosate, which also precipitated
extinction. Ethanol alone and the combination with linalool or acamprosate did
not alter locomotor activity. The results of this study suggest that linalool
may have pharmacological effects for the treatment of alcohol addiction."
https://www.sciencedirect.com/science/article/abs/pii/S0741832921001385
[977]
An addiction not everyone goes to the
doctor about.
So can linalool be bad in cannabis
but good in mint? Was Plato on to something with the kykeon?
We haven't tried to make a pill to
replace a cup of tea, have we?
So why do it to replace cannabis?
The greater good, the public good,
and the good news for pharmaceutical companies, are not continguous benefits.
So to the extent that cannabis is
being used medically, cannabis interdiction therefore represents commercial
favouritism as well as inflicting unnecessary suffering.
Thomas Clark, in "Cannabis Use Is
Associated with a Substantial Reduction in Premature Deaths in the United
States", published by Indiana University South Bend, 11 Aug. 2017, writes:
"Cannabis use prevents thousands of
premature deaths each year, and Cannabis prohibition is revealed as a major
cause of premature death in the U.S."
"Marijuana use is estimated to reduce
premature deaths from diabetes mellitus, cancer, and traumatic brain injury by
989 to 2,511 deaths for each 1% of the population using Cannabis."
"prohibition is estimated to lead to
similar numbers of premature deaths as drunk driving, homicide, or fatal opioid
overdose."
"23,500 to 47,500 deaths [would be]
prevented annually if medical marijuana were legal nationwide".
This, though, is "an underestimate"
says the Professor and Chair of the Department of Biology at South Bend Tom
Clark - this is because, and this was published August 2017, "a number of other
potential causes of reduced mortality due to Cannabis use were revealed, but
were excluded from the analysis because quantitative data were lacking."
His estimate of the odds ratio for
cancers of the head and neck is 0.83 for cannabis users.
"The relationship between Cannabis
and cancer is complex. Cancer is positively correlated with obesity, and obesity
decreases in a dose-dependent fashion with Cannabis use, whereas Cannabis smoke
contains carcinogens. On the other hand, a casual examination of the literature
reveals numerous laboratory studies demonstrating that cannabinoids have potent
anti-tumoral properties in vitro and in mouse models. Cancers inhibited by
cannabinoids include gliomas, thyroid epithelioma, lymphoma, neuroblastoma, and
carcinomas of the oral region, lung, skin, uterus, breast, prostate, pancreas,
and colon. Thus, Cannabis may reduce the risk of getting cancer by reducing
obesity rates and by direct inhibition of tumor formation or growth."
https://scholarworks.iu.edu/dspace/handle/2022/21632 [501]
Returning in 2021 with a broader look
at cancer and cannabis data, Clark published "Scoping Review and Meta-Analysis
Suggests that Cannabis Use May Reduce Cancer Risk in the United States":
"A total of 55 data points,
consisting of risk ratios of cancer in Cannabis users and nonusers, were
identified from 34 studies. Of these, 5 did not contain data essential for
inclusion in the meta-analysis. The remaining data showed a nonsignificant trend
to an association with reduced risk (relative risk [RR]=0.90, p>0.06, N=50)
although heterogeneity is high (I2=72.4%). Removal of data with high risk of
selection bias (defined as those from North Africa and those that failed to
adjust for tobacco) and data with high risk of performance bias (defined as
those with fewer than 20 cases or controls among Cannabis users) resulted in an
RR <1.0 (RR=0.86, p<0.017, N=24) and large effect size (Hedges g=0.66), but did
not decrease heterogeneity (I2=74.9). Of all cancer sites, only testicular
cancer showed an RR value >1, although this was not significant and had a
negligible effect size (RR=1.12, p=0.3, Hedges g=0.02). Following removal of
testicular cancers the remaining data showed a decrease in risk (RR=0.87,
p<0.025, N=41). Cancers of the head and neck showed a negative association with
cancer risk (RR=0.83, p<0.05), with a large effect size (Hedges g=0.55), but
high heterogeneity (I2=79.2%). RR did not reach statistical significance in the
remaining cancer site categories (lung, testicular, obesity-associated, other).
The data are consistent with a negative association between Cannabis use and
nontesticular cancer, but there is low confidence in this result due to high
heterogeneity and a paucity of data for many cancer types."
https://www.liebertpub.com/doi/10.1089/can.2019.0095 [2779]
Clark's findings were further confirmed in a 2025 meta-analysis by Castle et al:
"This meta-analysis was conducted to determine the scientific consensus on
medical cannabis's viability in cancer treatment. Objective: The aim of this
meta-analysis was to systematically assess the existing literature on medical
cannabis, focusing on its therapeutic potential, safety profiles, and role in
cancer treatment. Methods: This study synthesized data from over 10,000
peer-reviewed research papers, encompassing 39,767 data points related to
cannabis and various health outcomes. Using sentiment analysis, the study
identified correlations between cannabis use and supported, not supported, and
unclear sentiments across multiple categories, including cancer dynamics, health
metrics, and cancer treatments. A sensitivity analysis was conducted to validate
the reliability of the findings. Results: The meta-analysis revealed a
significant consensus supporting the use of medical cannabis in the categories
of health metrics, cancer treatments, and cancer dynamics. The aggregated
correlation strength of cannabis across all cancer topics indicates that support
for medical cannabis is 31.38X stronger than opposition to it. The analysis
highlighted the anti-inflammatory potential of cannabis, its use in managing
cancer-related symptoms such as pain, nausea, and appetite loss, and explored
the consensus on its use as an anti-carcinogenic agent.
https://www.frontiersin.org/journals/oncology/articles/10.3389/fonc.2025.1490621/abstract
[4853]
According to "Psychedelics for Brain
Injury: A Mini-Review" by Khan et al (2021), NECUD has a poor prognosis in TBI
patients:
"Presence of THC on urine drug screen
is associated with decreased mortality in adult patients sustaining TBI.
However, randomized control trials of a non-psychoactive cannabinoid analog,
dexanabinol, administered once after TBI has failed to show benefit over placebo
in increasing Glasgow Coma Scores at 6 months post-injury. One explanation for
this discrepancy may be the lack of 'entourage' effect whereby various
cannabinoids and cannabis phytochemicals are clinically more efficacious when
working synergistically compared to administration of a single cannabinoid in
isolation, though the existence of such an effect with cannabis is contentious
with mixed evidence for its existence. Of note, an 'entourage' effect has been
demonstrated with psychedelic mushrooms in which whole mushroom extracts are on
the order of 10 times more potent than purified psilocin administered alone in
neurobehavioral rat models."
https://www.frontiersin.org/articles/10.3389/fneur.2021.685085/full [776]
Meanwhile, "Inside One of the World's
Biggest Magic Mushroom Farms", similar issues to those of cannabis strength and
nature-identicalness have been carefully considered for the (probably US not
Canadian) $22 million investment:
"The company’s operation could have
been much more straightforward: Many mushroom companies just produce pure
psilocybin through chemical processes in the lab. Others simply grow mycelial
grain and sell it packaged as mushrooms. But Marshall believes that the
botanical route, to organically grow real mushrooms, is more beneficial.
To do so, the company had to invest
around $22 million to create this state-of-the-art farm. It includes rooms in
which levels of humidity, moisture, and heat can be altered to replicate the
climates of places where particular mushrooms thrive, like parts of Oregon and
Costa Rica; enabling them to grow such a diverse range, from phallic wands to
fluffy mycelial growths. Marshall has also built up a genetics bank of around
100 different strains, as he seeks to cultivate the most powerful mushrooms
possible so that patients can consume less."
https://www.vice.com/en/article/3akw7j/inside-one-of-the-worlds-biggest-magic-mushroom-farms
[3230]
Shahar et al (2024) compared "Effect
of chemically synthesized psilocybin and psychedelic mushroom extract on
molecular and metabolic profiles in mouse brain":
"In most clinical studies chemically
synthesized forms of these compounds are used. Naturally occurring psychedelic
compounds do not exist in isolation but are produced by the organism as part of
an extensive milieu that includes molecules of many different types. It is
possible that these molecules exert significant biological effects or modulate
the action of the active molecule in different ways. In regard to cannabis, it
is recognized that not only cannabidiol, but a number of other 'entourage'
molecules exert significant biological effects."
Once again, as with cannabinoids,
nature did it better:
"We compared the effects of PME to
those of PSIL on the head twitch response (HTR), neuroplasticity-related
synaptic proteins and frontal cortex metabolomic profiles in male C57Bl/6j mice.
HTR measurement showed similar effects of PSIL and PME over 20 min. Brain
specimens (frontal cortex, hippocampus, amygdala, striatum) were assayed for the
synaptic proteins, GAP43, PSD95, synaptophysin and SV2A, using western blots.
These proteins may serve as indicators of synaptic plasticity. Three days after
treatment, there was minimal increase in synaptic proteins. After 11 days, PSIL
and PME significantly increased GAP43 in the frontal cortex (p = 0.019; p =
0.039 respectively) and hippocampus (p = 0.015; p = 0.027) and synaptophysin in
the hippocampus (p = 0.041; p = 0.05) and amygdala (p = 0.035; p = 0.004). PSIL
increased SV2A in the amygdala (p = 0.036) and PME did so in the hippocampus (p
= 0.014). In the striatum, synaptophysin was increased by PME only (p = 0.023).
There were no significant effects of PSIL or PME on PSD95 in any brain area when
these were analyzed separately. Nested analysis of variance (ANOVA) showed a
significant increase in each of the 4 proteins over all brain areas for PME
versus vehicle control, while significant PSIL effects were observed only in the
hippocampus and amygdala and were limited to PSD95 and SV2A. Metabolomic
analyses of the pre-frontal cortex were performed by untargeted polar
metabolomics utilizing capillary electrophoresis – Fourier transform mass
spectrometry (CE-FTMS) and showed a differential metabolic separation between
PME and vehicle groups. The purines guanosine, hypoxanthine and inosine,
associated with oxidative stress and energy production pathways, showed a
progressive decline from VEH to PSIL to PME. In conclusion, our synaptic protein
findings suggest that PME has a more potent and prolonged effect on synaptic
plasticity than PSIL. Our metabolomics data support a gradient of effects from
inert vehicle via chemical psilocybin to PME further supporting differential
effects. Further studies are needed to confirm and extend these findings and to
identify the molecules that may be responsible for the enhanced effects of PME
as compared to psilocybin alone."
and
"The variability in effects produced
mushroom extracts compared to chemical psilocybin may be explained by differing
psilocybin content as well as by the presence and varying levels of other
potentially bioactive compounds in the different species of mushrooms. These
include tryptamines, such as 4- phosphoryloxy-N-methyltryptamine (baeocystin),
4-phosphoryloxy-N,N,N-trimethyltryptamine (aeruginascin),
4-hydroxy-Nmethyltryptamine (norpsilocin) and 4-phosphoryloxytryptamine
(norbaeocystin) as well as β-carbolines such as harmine and harmaline, and
terpenes. Little is known about the effects of these additional components of
psychedelic mushrooms in animal models, although there is accumulating evidence
regarding the effect of some of the tryptamines of the psilocybin biosynthetic
chain. Glatfelter et al. recently showed that only the tertiary amines,
psilocybin, psilocin, and 4- acetoxy-N,N-dimethyltryptamine (psilacetin) induced
HTR in mice while secondary amines such as baeocystin and norpsilocin and
quaternary ammonium compounds such as aeruginascin had little or no effect. It
is possible, however, that these tryptamines present in psychedelic mushroom
extracts may modulate the effects of psilocybin. In particular, it has been
speculated that baeocystin or norpsilocin could potentially contribute to
variable subjective effects. Furthermore, additional components of mushroom
extract such as betacarbolines may exert biologically meaningful effects in
spite of their low concentrations."
https://www.nature.com/articles/s41380-024-02477-w.pdf [3246]
"When an animal is given a drug, different metabolites accumulate as a result of
the drug’s interaction with the body. Predictably, the results showed that the
extract, which included a number of compounds in addition to psilocybin, created
a larger metabolic response. But more surprising, [Hadassah BrainLabs, a center
for psychedelics research
affiliated with Hebrew University's Bernard] Lerer says, was the extract’s
effect on proteins involved in making new connections between brain cells. 'What
we found was that there is a greater production of synaptic proteins following
administration of mushroom extract containing psilocybin than there is giving
psilocybin alone,' Lerer says. The researchers used Western blot analysis to
measure synaptic protein production. “It would appear that mushroom extract
increases synaptic plasticity."
...
"Further differences between mushroom extract and synthetic psilocybin were seen
in a second study on mice. Lerer and his colleagues found the mushroom extract
produced a stronger effect on reducing behaviors associated with anxiety than
did the synthetic psilocybin. But they found mushroom extract and synthetic
psilocybin had the same effect on reducing excessive self-grooming, a trait
representing OCD. While the study has seen some criticism for its methods and
analysis, the findings, if proven, could help demonstrate the potential for
targeted strategies using magic mushrooms to treat OCD and anxiety."
https://pubs.acs.org/doi/pdf/10.1021/acscentsci.5c01146?ref=article_openPDF
[5362]
That study, Brownstien et al (2024) "Striking long-term beneficial effects of
single dose psilocybin and psychedelic mushroom extract in the SAPAP3 rodent
model of OCD-like excessive self-grooming" relates how...
"There is increasing interest in the use of psilocybin and other tryptaminergic
psychedelics to treat a range of psychedelic disorders including major
depression, alcohol and nicotine addiction, and end of life anxiety. In an open
study, 9 patients with OCD were administered 29 doses of psilocybin ranging from
sub-hallucinogenic to frankly hallucinogenic. Reductions in OCD symptoms were
observed in all subjects and these generally lasted for at least 24 h."
The study set out to elucidate any differences between the synthetic psilocybin
and a natural mushroom extract containing the same amount of psilocybin,
attributable to the entourage ingredients in the extract, given to OCD-prone
mice:
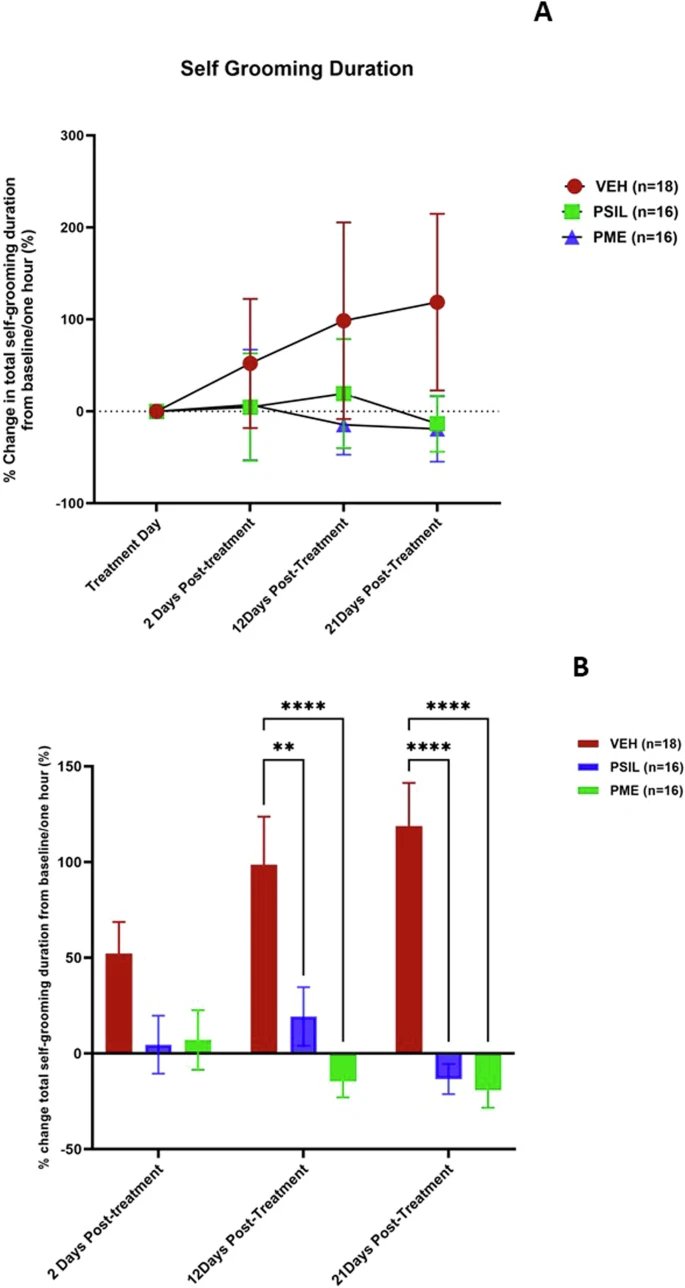
https://www.nature.com/articles/s41380-024-02786-0 [5363]
"Even if magic mushrooms’ secondary compounds are ultimately not found to have
any medical benefits, a natural product could still have value. When psilocybin
is administered medically, the patient’s environment and mindset are important
in the outcome of the psychedelic trip. 'Having the participant know that this
drug you’re taking came from a natural source and was actually grown and things
like that might, at least for some people, offer some reassurance in the
sometimes challenging experience,' [chief science officer at Filament Health
Ryan] Moss says."
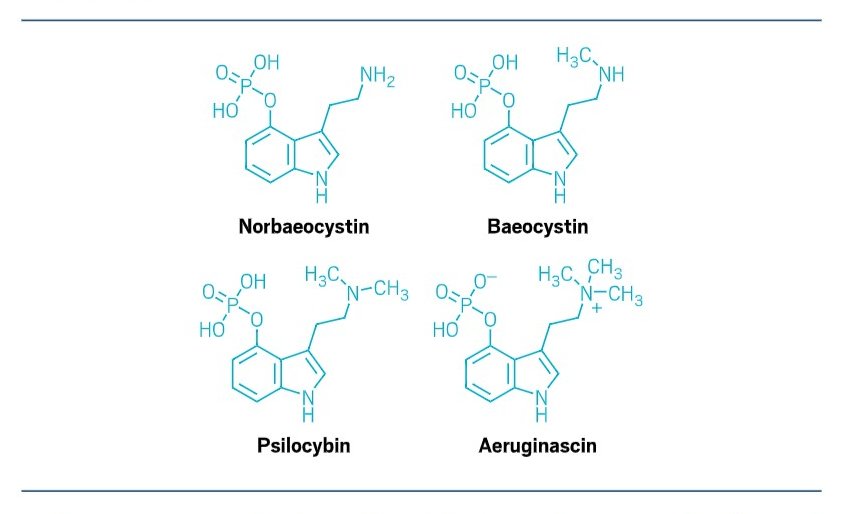 [5362]
[5362]
Addressing the problem that "few
empirical studies have systematically evaluated" the entourage effect, it became
a clinical reality three years later with the publication of "Vaporized
D-limonene selectively mitigates the acute anxiogenic effects of
Δ9-tetrahydrocannabinol in healthy adults who intermittently use cannabis"
(2024) in which Spindle et al report:
"Administration of 15 mg and 30 mg
THC alone produced subjective, cognitive, and physiological effects typical of
acute cannabis exposure. Ratings of anxiety-like subjective effects
qualitatively decreased as d-limonene dose increased and concurrent
administration of 30 mg THC+15 mg d-limonene significantly reduced ratings of
“anxious/nervous” and “paranoid” compared with 30 mg THC alone. Other
pharmacodynamic effects were unchanged by d-limonene. D-limonene plasma
concentrations were dose orderly, and concurrent administration of d-limonene
did not alter THC pharmacokinetics."
Leading to the conclusion that:
"D-limonene selectively attenuated
THC-induced anxiogenic effects, suggesting this terpenoid could increase the
therapeutic index of THC."
https://www.sciencedirect.com/science/article/abs/pii/S0376871624001881
[4519]

As for connectivity within the
associative, limbic, and sensorimotor striata, results have been mixed. A 2022
fMRI study found it reduced less by THC+CBD than by THC alone.
No one has tested to this level for
combinations of coffee and cigarettes, nicotine and alcohol, or alcohol and
caffeine.
There has been no discussion of
legislating against these particular types of alterations in connectivity, or
for what reasons that might be desirable, or how this would be measured in vivo
on a continuous basis.
https://journals.sagepub.com/doi/10.1177/02698811221092506 [1415]
Research into alcohol's effects on
brain biochemistry is full of holes. For instance Urbanik et al in Poland (2020)
considered themselves the first to examine changes in brain lipids after
administration, using proton magnetic resonance spectroscopy (1HMRS) and
diffusion weighted imaging (DWI):
"A peak corresponding to lipids (Lip)
is not visible in 1H MR spectrum of a healthy brain. In pathological conditions
it reflects either damage to cell membrane or necrosis (Cichocka and Urbanik,
2017). It was established that concentrations of lipids in tissues correlate
with the intensity of necrosis (Cichocka and Urbanik, 2017). Lipids are visible
in 1H MR spectra during ischemic stroke (Seeger et al., 2003, Gasparovic et al.,
2001). In the current study lipid concentrations in the volunteers exposed to
alcohol tended to increase during the first hour, and then the levels started to
decrease. These changes were statistically significant, and their profile was
positively correlated to the changes in EtOH levels. No analyses of changes in
Lip levels, in relation to alcohol consumption, were found in the available
literature."
https://academic.oup.com/alcalc/article/56/4/415/5974947 [2144]
WebMD lists some physical
characteristics of a genius brain.
"Signs of a Genius Brain
"There are some certain physical
traits shared by the brains of people who are geniuses or who have extreme
intelligence.
"Larger regional brain volume.
Contrary to popular myth, intellect does not result from brain size. But brain
scans have shown that gifted people or geniuses have more grey matter. This is
the part of your brain responsible for computing and processing information. It
directs your attention, memory, language, perception, and interpretations.
"Increased brain region connectivity.
Highly gifted or genius individuals typically have more active white matter in
their brains. White matter is responsible for the communication between
different parts of your brain. Genius brains seem to have a better network of
these connections. It results in very quick and complex thinking.
"Increased sensory sensitivity and
emotional processing. Genius brains can experience 'superstimulability.' Some
genius brains are highly sensitive to other people’s emotions. This can help
relate to other people. But at times it can be overwhelming and tiring."
https://www.webmd.com/balance/what-are-signs-of-genius [1588]
Measuring white matter phospholipid
damage from alcohol exposure (in 2001):
"Background: Phosphorus magnetic
resonance spectroscopy (31P MRS) allows for the measurement of phospholipids and
their breakdown products in the human brain. Fairly mobile membrane
phospholipids give rise to a broad signal that co-resonates with metabolic
phosphodiesters. Chronic alcohol exposure increases the rigidity of isolated
brain membranes and, thus, may affect the amount and transverse relaxation times
(T2) of MRS-detectable phospholipids. We tested the hypothesis that subjects who
were heavy drinkers have stiffer membranes than controls who were light
drinkers, as reflected in a smaller broad signal component and a shorter T2 of
the broad signal in 31P MR spectra of the brain.
"Methods: Thirteen alcohol-dependent
heavy drinkers (mean age 44 years) were studied by localized 31P MRS in the
centrum semiovale and compared with 17 nondependent light drinkers of similar
age. The broad component signal was separated from the metabolite signal by
convolution difference, which is based on the large difference in line widths of
these two signals. Longitudinal and T2 relaxation times were measured using
standard methods.
"Results: The broad component
integral was 13% lower in the brain of heavy drinkers compared with light
drinkers (p < 0.001) and remained significantly smaller after corrections for
both longitudinal and transverse relaxations (p < 0.01). The T2 distribution of
the broad component consistently showed two resolvable components in both
groups. The fast relaxing component had the same T2 in both groups (T2 = 1.9
msec). The slower relaxing component T2 was 0.6 msec shorter in heavy drinkers
compared with light drinkers (p = 0.08).
"Conclusions: These results, observed
in the absence of white matter volume loss, are consistent with biochemical
alterations and higher rigidity of white matter phospholipids associated with
long-term chronic alcohol abuse. The observed smaller broad signal component in
these relatively young heavy drinkers is a sensitive measure of white matter
phospholipid damage."
https://pubmed.ncbi.nlm.nih.gov/11198719/ [2141]
Happily. according to Chamoso-Sanchez
(2025):
"The comprehensive characterization of cellular lipids unveiled several classes
significantly affected by CBD treatment. Most of the differences correspond to
phospholipids, including cardiolipins (CL), phosphatidylcholines (PC) and
phosphosphingolipids (SM), and also triacylglycerols (TG), being many TG species
increased after CBD treatment in the acute and chronic models, whereas
phospholipids were found to be decreased. The results highlight some important
lipid alterations related to CBD treatment, plausibly connected with different
metabolic mechanisms involved in the process of cell death by apoptosis in
cancer cell lines."
https://pubmed.ncbi.nlm.nih.gov/39824876/ [2841]
Meanwhile, for those who just want to
get high, an unpublished study by Bosnjak et al has compared THC alone with THC
plus other CCx.
"...finding that cannabis products
with a more diverse array of natural cannabinoids produce an even stronger
psychoactive experience that lasts longer than the high generated by pure THC
products.
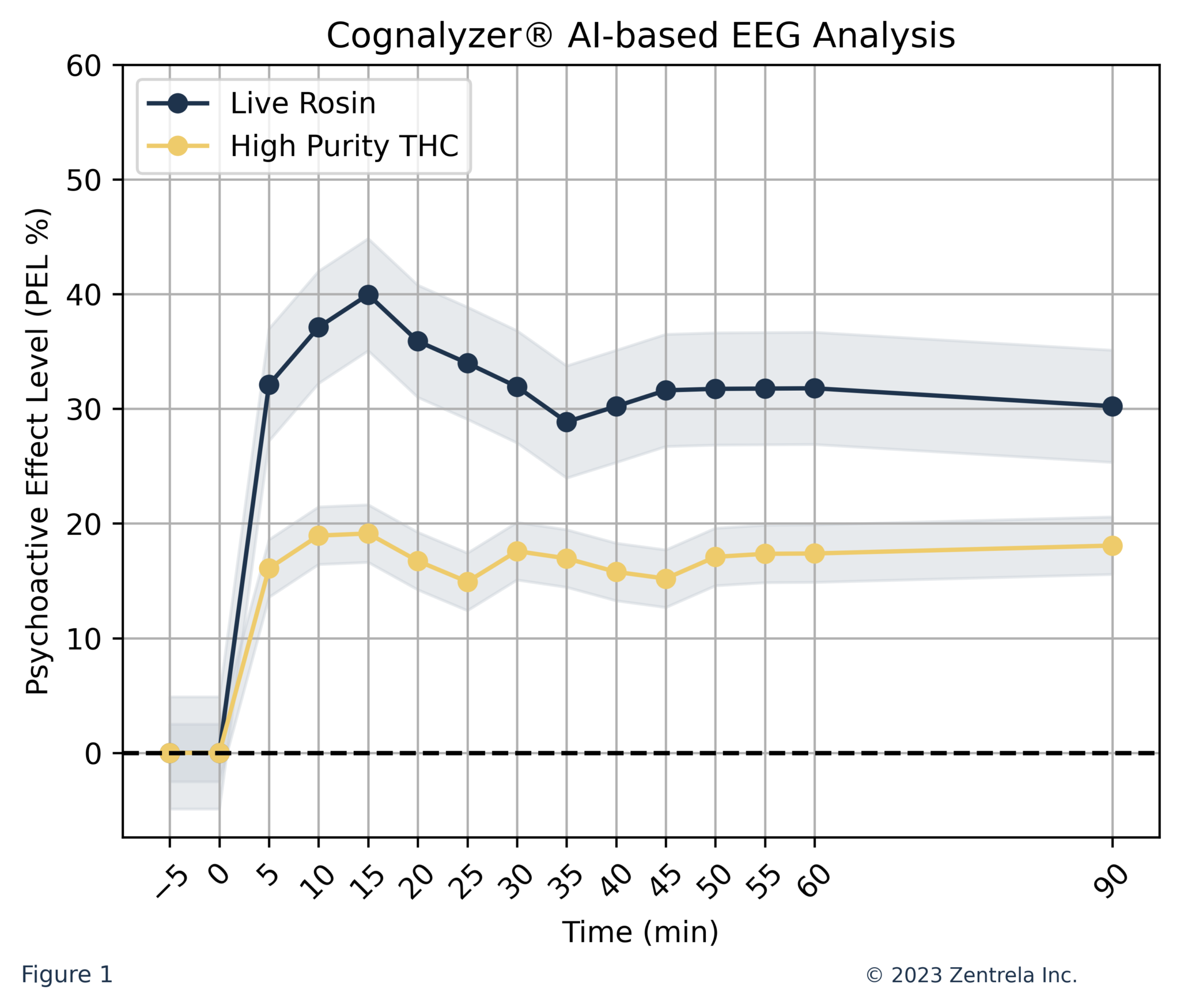
"The study utilized novel
electroencephalogram (EEG) technology supported by AI to quantify the “high”
people experienced when vaping two different products: 1) a full-spectrum live
rosin with average 85 percent THC as well as other natural cannabinoids and
terpenes, and 2) a high purity THC oil with 82-85 percent potency.
“The first group exhibited a
considerably faster and more potent psychoactive response compared to the latter
group.”
"A total of 28 adults participated in
the study, strapping on the EEG headset developed by the cannabis technology
company Zentrela and taking two hits (8 mg) of either the full-spectrum or pure
THC varieties from a vape manufactured by PAX, which also supported the study.
"After getting a baseline reading
before the participants consumed the products, the EEG monitored activity in
eight regions of the brain over the course of 90 minutes. The tests were then
converted into “psychoactive effect levels (PEL) in a standardized scale from
zero percent to 100 percent.”
"The results showed that the
full-spectrum live rosin with THC and other cannabinoids and terpenes had a
slightly earlier onset of three minutes, a higher potency reading for the onset
(20.8 percent) and higher potency at the peak after 15 minutes (40 percent) and
after 90 minutes (30.2 percent)."
https://zentrela.com/publication/cusic-6/ [4047]
https://www.marijuanamoment.net/marijuana-entourage-effect-with-multiple-cannabinoids-produces-a-stronger-and-longer-lasting-high-than-pure-thc-study-finds/
[4048]
To add to the fun, CCx do not end
with cannabinoids and terpenes, says a 2023 paper by Oswald et al:
"Here, we show that across Cannabis
sativa L. varieties with divergent aromas, terpene expression remains remarkably
similar, indicating their benign contribution to these unique, specific scents.
Instead, we found that many minor, nonterpenoid compounds correlate strongly
with nonprototypical sweet or savory aromas produced by Cannabis sativa L.
Coupling sensory studies to our chemical analysis, we derive correlations
between groups of compounds, or in some cases, individual compounds, that
produce many of these diverse scents. In particular, we identified a new class
of volatile sulfur compounds (VSCs) containing the 3-mercaptohexyl functional
group responsible for the distinct citrus aromas in certain varieties and
skatole (3-methylindole) as the key source of the chemical aroma in others. Our
results provide not only a rich understanding of the chemistry of Cannabis
sativa L. but also highlight how the importance of terpenes in the context of
the aroma of Cannabis sativa L. has been overemphasized."
https://pubs.acs.org/doi/10.1021/acsomega.3c04496 [4049]
----------------------------------------------------------------------------
The Englishman stands
for the rights of everyone disadvantaged, discriminated against, persecuted, and
prosecuted on the false or absent bases of prohibition, and also believes the
victims of these officially-sanctioned prejudices have been appallingly treated
and should be pardoned and compensated.
The Englishman requests the return of his CaPs
and other rightful property, for whose distraint Slovenia has proffered no
credible excuse or cause.
The Benedictions represent both empirical entities as well as beliefs. Beliefs
which the Defence evidence shows may be reasonably and earnestly held about the
positive benefits of CaPs at the population level, in which the good
overwhelmingly outweighs the bad. Below, the latest version of this dynamic
list.
THE BENEDICTIONS
REFERENCES
TIMELINE OF DRUG LAW v. SCIENCE